Stroke localization is one of the most powerful bedside skills in neurology and also one of the most favorite questions consultants ask during morning rounds.
So if you want to avoid getting embarrassed during rounds, you should definitely know these patterns.
Here are more high yield stroke localization pearls for residents and house officers 👇
➡️ Aphasia = dominant hemisphere lesion (usually left MCA) until proven otherwise.
➡️ Neglect = non-dominant parietal lobe stroke (usually right MCA).
➡️ Crossed signs (cranial nerve deficit on one side + body weakness on opposite side) = brainstem stroke.
➡️ Sudden vertigo + ataxia + diplopia = posterior circulation stroke unless proven otherwise.
➡️ Pure motor hemiparesis with no cortical signs = lacunar infarct.
➡️ Visual field defect without weakness = think PCA territory.
➡️ Locked-in syndrome is basilar artery thrombosis until proven otherwise.
➡️ Face and arm weakness worse than leg = MCA stroke.
➡️ Leg-predominant weakness = ACA stroke.
➡️ Dysphagia + hoarseness + ipsilateral facial sensory loss = lateral medullary syndrome.
➡️ A patient who “cannot speak” may still fully understand you → Broca aphasia.
➡️ Fluent but meaningless speech with poor comprehension → Wernicke aphasia.
➡️ Eye deviation usually points toward the side of hemispheric stroke.
➡️ Thalamic strokes commonly present with pure sensory deficits.
➡️ Sudden coma with pinpoint pupils should raise concern for pontine hemorrhage.
➡️ Severe headache + vomiting + decreased consciousness = think hemorrhagic stroke.
➡️ New atrial fibrillation in stroke patient = always suspect cardioembolic stroke.
➡️ Brainstem strokes can present subtly but deteriorate rapidly.
➡️ Bilateral weakness is never a typical MCA stroke pattern — think brainstem/basilar pathology.
➡️ If symptoms do not fit one vascular territory, reconsider the diagnosis.
➡️ Cortical signs = aphasia, neglect, gaze deviation, visual field defects, seizures.
➡️ Absence of cortical signs strongly favors lacunar stroke.
➡️ Sudden isolated ataxia in elderly hypertensive patient can still be a stroke.
➡️ Posterior circulation strokes are commonly missed in emergency settings.
➡️ Normal CT brain early in ischemic stroke does NOT exclude stroke.
Who needs more evidence to stop placing central venous lines for short term vasopressor use with appropriate monitoring? Yet another study @JAMANetworkOpen shows low incidence of adverse events with avoidance of CVC in a substantial proportion of patients. https://t.co/F4EWBEXS9e
Sometimes in medicine we struggle with futility, but nothing matches the futility of a drug rep earnestly making their pitch to the med student who is only there for food
Couldn’t afford the $1,245 suture ring used for valve training.
So I learned 3D printing and built two… for the price of coffee.
Every resident says they want better training, few create it.
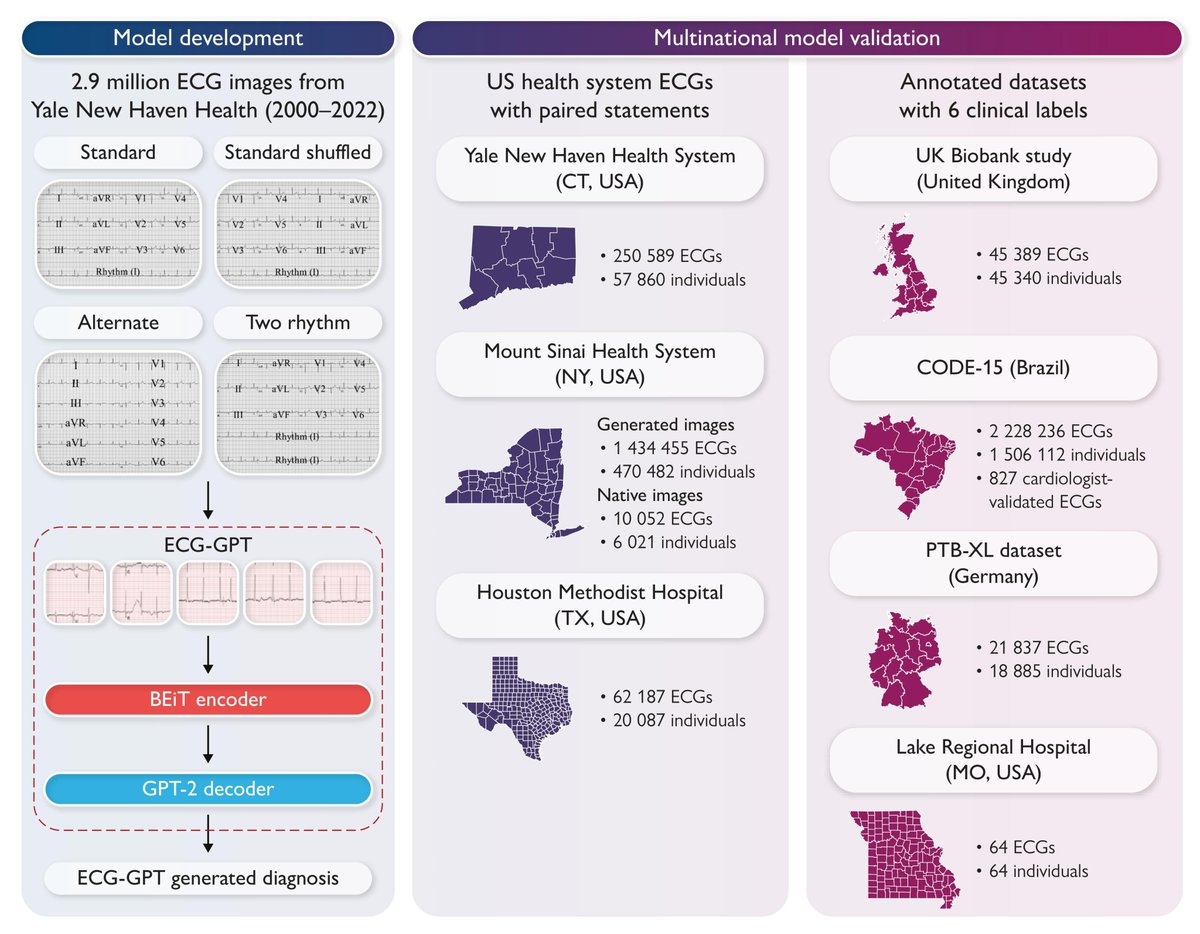
Can AI read an ECG like a cardiologist - from just an image?
We built ECG-GPT, a vision-text transformer that generates complete diagnostic reports directly from photos of 12-lead ECGs
Now out in @ESC_Journals#EHJDigitalHealth
Kudos to @aakhunte & @Veer_Sangha_ for leading this @cards_lab
🧵
First prehospital ECPR pilot in Catalonia. Months of work + training/simulation, within the high-complexity retrieval program @quebecsem and a strategic alliance between @semgencat + ECMO centers. First milestone. Now evaluate, learn & scale. Huge thanks to all teams involved 🙌🏻
Full House - ECMO Conference, Cartagena, Colombia 🇨🇴 (Day 3/3)!
Thank you to all of our colleagues who supported this initiative. I am very grateful. @MayoAnesthesia@MayoClinicCVS