Koeckerling et al. just dropped in @JACCJournals: a reconstructed-IPD meta-analysis of all 5 RCTs comparing PCI vs CABG for left main disease (LE MANS, SYNTAX, PRECOMBAT, EXCEL, NOBLE). 4,499 patients pooled. The headline: 10-year all-cause mortality is virtually identical — 23.4% vs 23.3%, HR 1.02 (0.89–1.17), RMST difference of exactly 0.0 years.
This is genuinely good news. For patients with left main disease and low-to-intermediate anatomic complexity who are eligible for both strategies, we can now tell them with reasonable confidence: your chances of being alive at 10 years are the same regardless of which path you choose.
The methodology deserves praise. The team used reconstructed time-to-event IPD (via the IPDfromKM algorithm) with 98.7% fidelity, pooled in a 1-stage Cox model with γ-frailty for trial, verified proportional hazards (Schoenfeld P=0.59), ran RMST as a complementary analysis, and confirmed everything with conventional fixed/random effects meta-analysis. Every approach converges to the same number. That's reassuring.
But as with any meta-analysis, the fine print matters. A few observations:
𝗧𝗵𝗲 𝗘𝗫𝗖𝗘𝗟 𝗾𝘂𝗲𝘀𝘁𝗶𝗼𝗻
EXCEL is the largest trial (n=1905, 23% of the weight) and the only one with contemporary 2nd-gen DES (everolimus). It's also the only trial censored at 5 years — no 10-year follow-up, none planned. And it was the only trial showing a statistically significant excess in all-cause mortality with PCI at 5 years (13.0% vs 9.9%, difference 3.1 pp).
@GreggWStone et al. themselves wrote in NEJM 2019: "at this time point the hazard curves were continuing to diverge. Ten-year follow-up is needed."
Administrative censoring at 5 years is statistically valid — it doesn't bias the HR within the observed window. But it removes the possibility of detecting whether the divergence continued or reversed. The other 4 trials that DO have 10-year data all used 1st-gen DES or BMS. So the question "what happens to everolimus-eluting stents in left main at 10 years?" remains genuinely unanswered.
𝗥𝗲𝗰𝗼𝗻𝘀𝘁𝗿𝘂𝗰𝘁𝗲𝗱 𝗜𝗣𝗗 ≠ 𝘁𝗿𝘂𝗲 𝗜𝗣𝗗
The reconstruction method is validated and reliable for time-to-event data. But it cannot recover individual covariates. This means the meta-analysis cannot test treatment-by-subgroup interactions for diabetes, acute coronary syndromes, or SYNTAX score at 10 years. The Sabatine et al. IPD meta-analysis (Lancet 2021) found no interaction at 5 years — but extrapolating that to 10 years is an assumption, not a finding.
This matters because the NOBLE 10-year paper (Holck et al., Lancet 2026) found a significant interaction between ACS presentation and mortality (HR 0.57 favoring PCI in ACS, p_interaction=0.049). If confirmed, this would have major practical implications. But it couldn't be tested in the pooled analysis.
𝗠𝗼𝗿𝘁𝗮𝗹𝗶𝘁𝘆 𝗲𝗾𝘂𝗮𝗹 ≠ 𝗼𝘂𝘁𝗰𝗼𝗺𝗲𝘀 𝗲𝗾𝘂𝗮𝗹
The meta-analysis only reports mortality. No MI, no stroke, no repeat revascularization. This is a deliberate and defensible choice (mortality is the hardest endpoint, immune to ascertainment bias). But it leaves the conversation incomplete.
As an exercise, I pooled the 3 trials that report non-mortality endpoints at their longest available follow-up (LE MANS 10yr, PRECOMBAT 10yr, EXCEL 5yr — ~2,610 patients). Exploratory, not definitive, but informative:
→ Repeat revascularization: RR 1.66 (1.36–2.03). Significantly and consistently higher with PCI. No surprise — but the magnitude matters for shared decision-making.
→ Total MI: RR 1.12 (0.87–1.46). Apparently neutral. But EXCEL shows why this is misleading: periprocedural MI favored PCI (RR ~0.66) while spontaneous MI favored CABG (RR ~1.92). They cancel out in the composite. Classic Simpson's-adjacent phenomenon — the total hides a divergence that matters clinically.
→ Spontaneous MI (EXCEL-driven): RR 1.64 (1.14–2.38), P=0.008. This is the trade-off the patient needs to hear. CABG appears to protect better against late spontaneous infarction — plausibly because grafts bypass vulnerable proximal plaques that stents don't address.
Caveat: SYNTAX and NOBLE didn't collect these endpoints between 5–10 years, so this analysis is incomplete. It's a conversation starter, not a conclusion.
𝗛𝗼𝘄 𝗱𝗼𝗲𝘀 𝗢𝗣𝗧𝗜𝗠𝗔𝗟 𝗳𝗶𝘁 𝗶𝗻?
The OPTIMAL trial (Testa et al., NEJM 2026) just showed that IVUS-guided PCI adds no benefit over angiography-guided PCI in left main (HR 1.11, 0.87–1.42). This seems to contradict the NOBLE IVUS substudy (20% vs 31% mortality with/without final IVUS).
But there's no contradiction. The NOBLE observation was confounded by indication. OPTIMAL randomized the comparison and found that in expert hands — operators who already internalize IVUS-derived optimization criteria — the imaging itself doesn't add incremental value. The control arm had 96% post-dilation rates and 85% POT. That's not "angiography-naïve" PCI — it's PCI done by people who think with IVUS even when they don't use it.
This actually reinforces the Koeckerling findings: PCI in the included trials, even without mandated imaging, achieved equivalent mortality to CABG. If even IVUS doesn't move the needle in expert centers, then the mortality equivalence reported in the meta-analysis is likely robust and not contingent on a hypothetical "better PCI."
𝗧𝗮𝗸𝗲-𝗮𝘄𝗮𝘆
My thoughts:
1. PCI and CABG offer the same probability of being alive at 10 years in patients with left main disease and SYNTAX ≤32. This is established.
2. But equal survival is not the same as equal outcomes. PCI means ~66% more repeat revascularization and likely more spontaneous MI. CABG means more periprocedural stroke and a harder early recovery.
3. The choice isn't about which is "better." It's about which set of trade-offs aligns with the patient sitting in front of you — their anatomy, their comorbidities, their values, their fear of surgery vs. their tolerance for reintervention.
Equal mortality is the foundation. The rest is shared decision-making. Again, kudos to the authors. This is beautiful work!
#CardiologyX #InterventionalCardiology #LeftMain
#LAAC where is the truth? whereas #CLOSURE-AF was not totally negative, #CHAMPION-AF is not all positive. methodologically both trials have instrumental limitations leaving the clinical indication of a #LAAC not clear. to me:
1/ important to select the pt who can benefit the most. probably too high risk pts are not a correct target.
2/for the rest, to have a correct informed consent and discussion with the pts is more important now than ever: we need to inform them that with #LAAC we may prevent non-major bleeding, but for the rest is the same. and periprocedural complications should be considered in this equation.
3/role of #AF ablation is likely underestimated. #LAAC advantages may probably come from #AF ablation rather than from the procedure itself? see #OPTION in @NEJM and #CHAMPION-AF where almost half of the pts had such procedure.
4/waiting for a metanalysis in this topic, which will be unfortunately limited by differences in endpoints between the various trials. a MA based on individual patient data would be needed!
5/last but not least we have to admit that in theory #LAAC should have won easily against #NOAC in terms of stroke and reduced bleeding but it did not. We need to be very cautious, thinking that we are not at a stage to make #LAAC to all our patients, but to some of them. and this is important because we should maintain our critical thinking against any kind of industries claims about #LAAC and I would be curious to see if it is cost-effective... #tricuspid interventions docet @PCRonline@ACCinTouch@escardio@TCTMD@shci_sec@sicigise@secardiologia
Pulmonary artery waveform transitioning to PCWP. Measures obtained with Swan-Ganz catheter in a patient with AMI related Cardiogenic Shock. #CardioTwitter#ICU#CriticalCare
In the 1960s, a young cardiologist came to the US with a radical dream.
He wanted to build a device that could shock the heart back to life - from inside the body.
Everyone told him it was insane.
They laughed.
They rejected him.
He built it anyway.
Here's his story:
1️⃣ Be resilient
2️⃣ Take risks and go beyond what you think you are capable of
3️⃣ Enjoy the ride
I look forward to the "Fantastic Voyage" of this next year and beyond! - #ACCPresident@ChrisKramerMD#ACC25
La enfermedad cardiovascular aterosclerótica es la primera causa de muerte en mujeres, y muchas veces subdiagnosticada #goredforwomen#7Febrero
❤️❤️❤️❤️❤️❤️
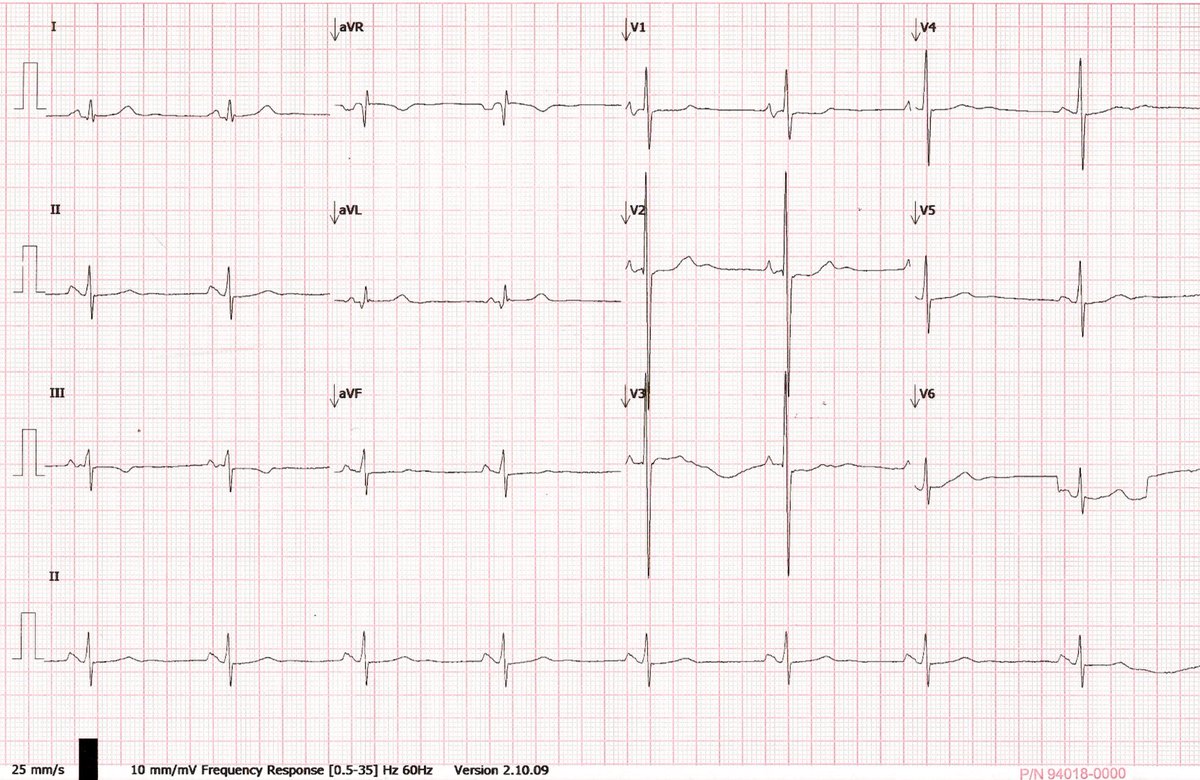
63 Yo With worsening SOB in the ER. Chest X-Ray showed bilat pleural eff, pulmonary edema, left atrial enlargement (4 arch left contour, wide carina), prominent PA branches and EKG with RV strain (Tall R Waves V2) and LAA (Biphasic P wave V1) #ACC#FIT#ESC#EKG#CardioTwitter
Echo showed a left atrial mass occupying >80% of the LA adyacent to the inter atrial septum, px underwent surgery confirming a left atrial myxoma later on pathology #ACC#FIT#ESC#CardioTwitter#echofirst
@MaruanCarlos No Sgarbossa criteria fulfilled but sometimes clinical presentation + having seen a lot of LBBB tells you something is not right at the ST segment in V1-V4 (OMI). Excellent example to remember that cardiology cannot exist without clinical expertise.
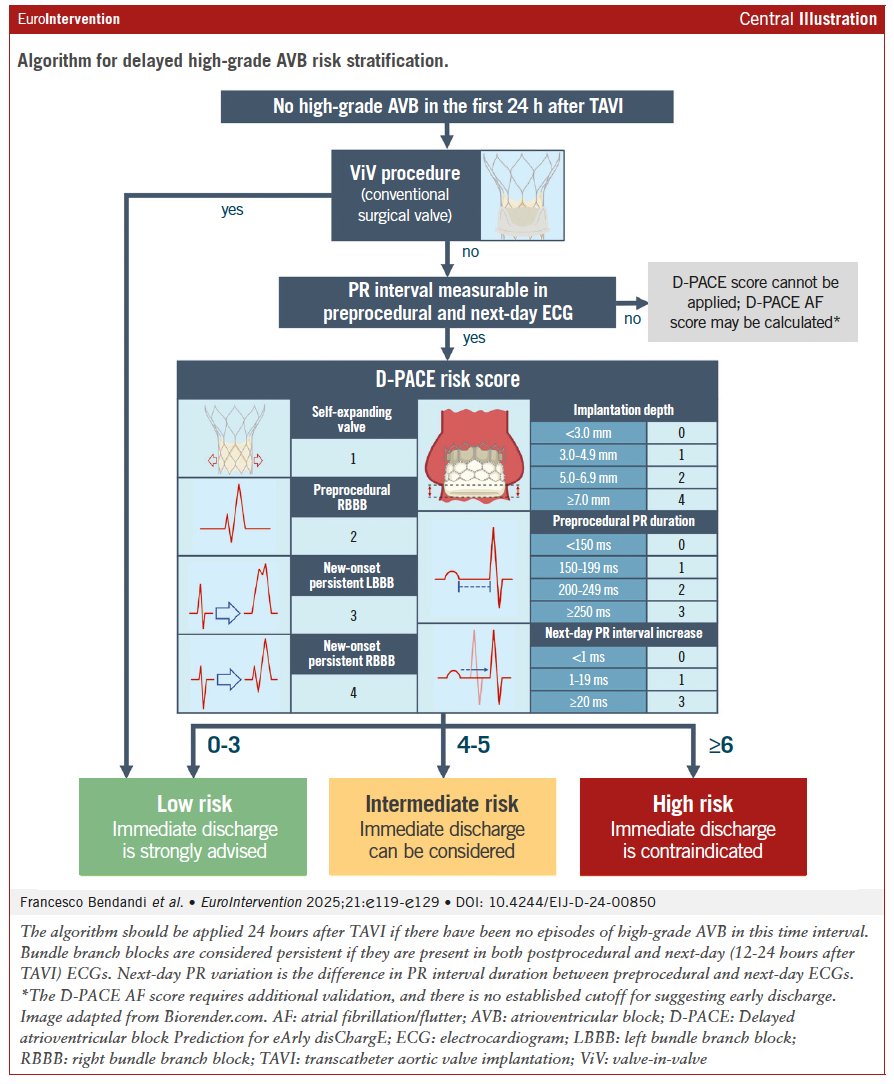
"The Delayed atrioventricular block Prediction for eArly disChargE (D-PACE) score, consisting of procedural and electrocardiographic variables, can be used the day after transcatheter aortic valve implantation to stratify patients according to the risk of delayed high-grade atrioventricular block. Based on the result of the score, it is possible to identify patients who can be safely discharged 24 hours after the procedure." #EAPCI #TAVI
@fra_bendandi@saia_francesco
https://t.co/UiyfXi9QiL
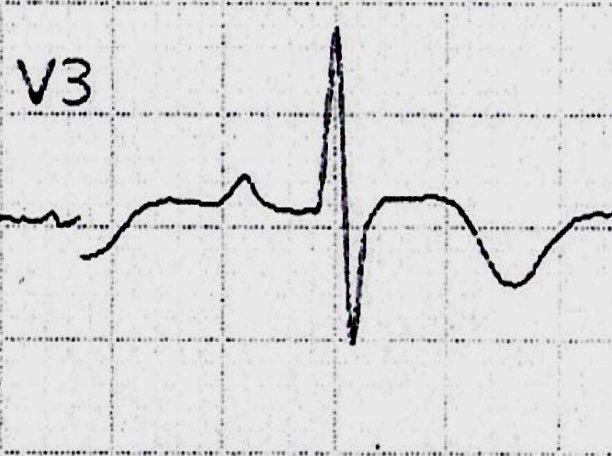
Some of the features you can find on V2-V3 are:
- Downsloping ST segment depression
- ST rectification
- Deep inverted asymmetrical T waves
- R > S
- QRS Fragmentation
- RBBB
- High Voltage P waves
There are very precise features to identify right ventricular strain on EKG, nevertheless focusing on one or two leads for a certain pathology on various EKGs can help you notice small but very distinct signs. #EKG#FIT#ACC#ESC#CardioTwitter
(1/x) Intubating a critically ill patients is the most dangerous procedure we do in the ICU (3.1% cardiac arrest rate) not because of hypoxia or tube placement, but hemodynamic collapse 🫀
(Russotto et al. JAMA 2021)
A 🧵on making high risk hemodynamic intubations as safe as possible.