Had a blast talking with @fadamsmd about updated guidelines on steroid use in ARDS, sepsis and CAP on @NYUDocs — though at 6a, my face is only for radio! 😂 Thanks for having me!
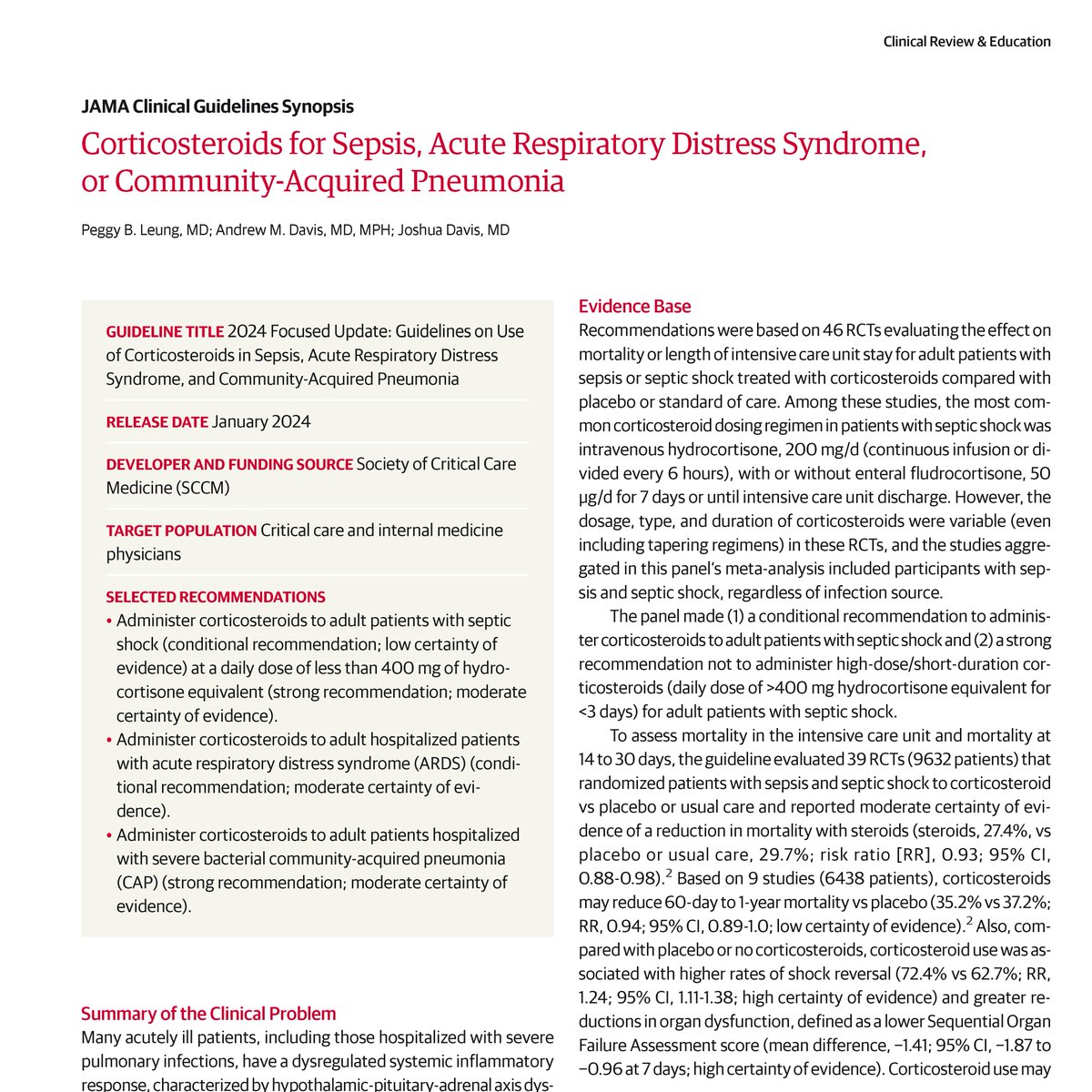
This JAMA Clinical Guidelines Synopsis summarizes the 2024 Society of Critical Care Medicine guidelines on use of corticosteroids in sepsis, acute respiratory distress syndrome, and community-acquired pneumonia.
https://t.co/gADRFLLC8K
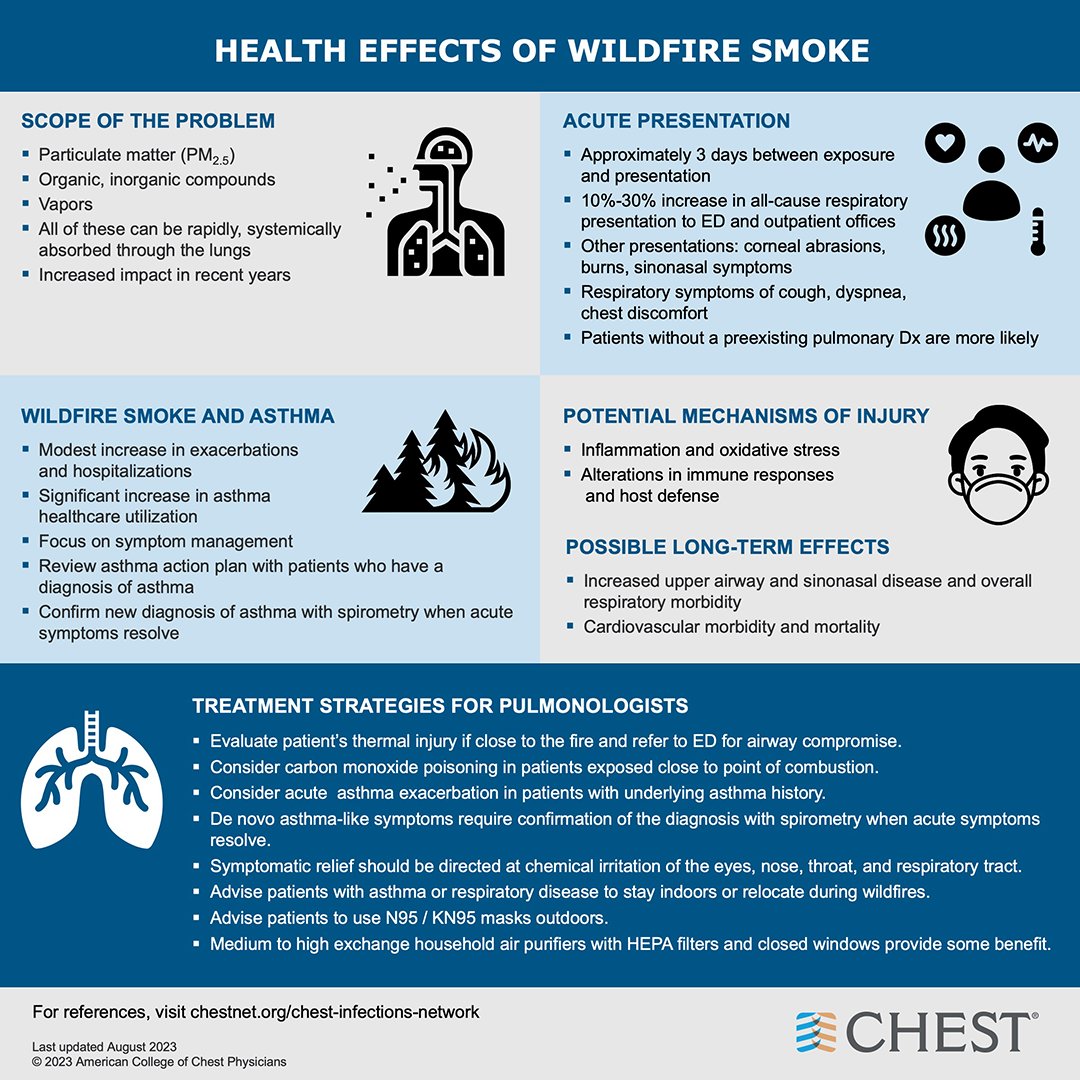
As the tragic #CaliforniaWildfires continue, those with respiratory disease will be most impacted as exposure continues. Learn more about treatment protocols from the Chest Infection and Disaster Response Network: https://t.co/b59vjaGuDH
#WildfireSmoke
Excited to share our @JAMA_current CGS on SCCM’s 2024 guidelines on use of corticosteroids in sepsis, ARDS, and CAP!
📣learn about the nuanced evidence behind the rec for corticosteroid use.
As always it’s great to work with @AndyDavis@JoshDavisMD!
@WCMGIM@WCM_MedChiefs
1. Optimise patient position
Ear-to-sternal notch horizontal alignment with neck flexion never lets you down. Also called 'flextension' this is identical to the optimal direct laryngoscopy position
The iGel is a great supraglottic airway device
But like other supraglottic airway devices (SAD) it's not foolproof
Here's how to maximise your success with the iGel - a thread 🧵
The iGel is a great supraglottic airway device
But like other supraglottic airway devices (SAD) it's not foolproof
Here's how to maximise your success with the iGel - a thread 🧵
Best way to wrap up the pulmonary unit for @WeillCornell MS1s with @Doclief interviewing Dr Chris Belardi — one of our ED physicians, medical educators and COVID ARDS survivor. An inspiration and a privilege!
Here’s another pulmonary physiology question that *everyone* who gives O2 to patients ought to know:
What is the primary mechanism by which supplemental oxygen can increase PaCO2 in someone with severe COPD?
1/
@emily_fri@eemoin@msiuba@iceman_ex Especially so when they’re really sick and can’t lay flat! Yes, higher rate of infections with femoral lines. But femoral line for a few days, then convert to IJ — if we’re talking about avoiding intubation, I think it’s worth it
@meredithturetz gave a ⛹🏻♀️🏀🗑️ (slam dunk) talk about restrictive lung diseases and touched upon the finding of clubbing. We can’t talk about clubbing without the great Dr. Cooper’s tweetorial about it! 🧵👇🏻
1/
Fingernail clubbing is associated with many systemic diseases, from lung cancer to TB to inflammatory bowel disease.
Why would such different diseases all manifest with clubbing?
The answer is surprisingly simple and elegant.
#medtwitter#tweetorial
It’s my favorite time of the year — time to teach pulmonary physiology (and patho-) to the MS1s @WeillCornell with my partner in learning @meredithturetz. Had the opportunity to teach a new lecture today on gas transport — and had so much fun! 🥸🫁💨
@jducanto@hraza222 We don’t get 8 minutes of apnea time in the MICU, so would’ve had a tube loaded on a bronch for anticipated difficult airway & lifted tissue with laryngoscope and pass tube over bronch. Just need 2 operators. Especially love now the side by side VL & bronch on the GlideScope now!
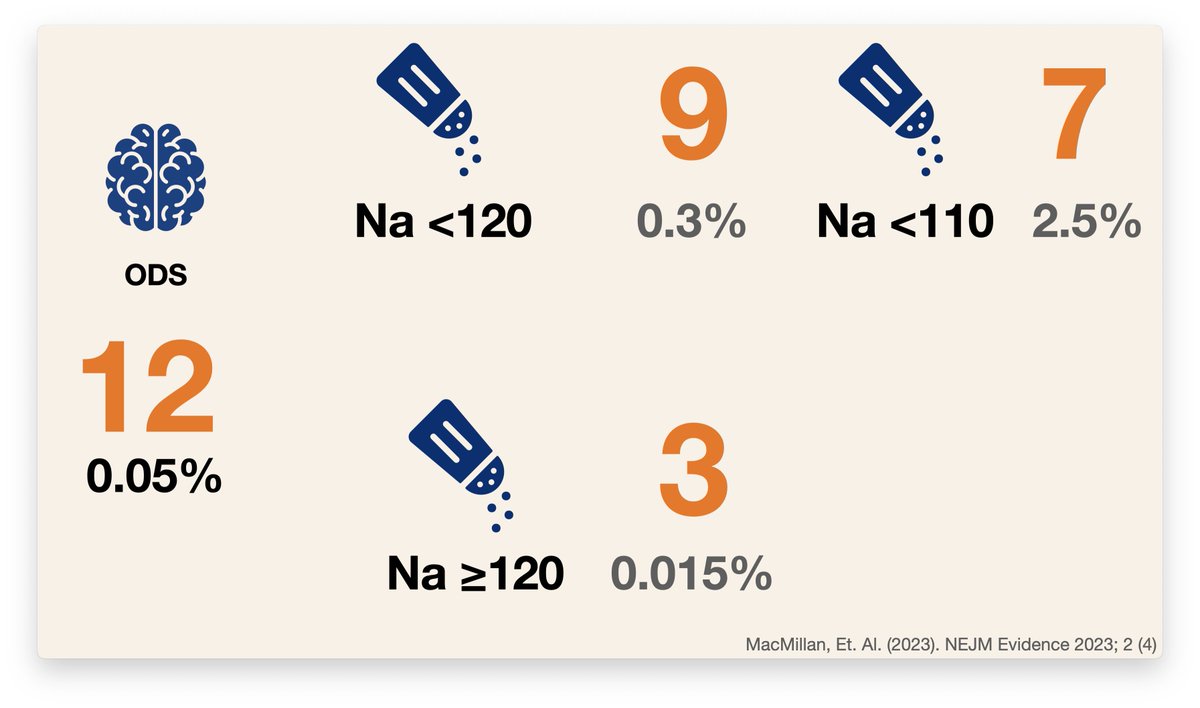
And what was the consequence of all that hyponatremia? All that rapid correction? 12 of osmotic demyelinating syndrome.
12 out of 22,858. 0.05%
If you divide by starting Na they found an incidence of:
0.3% with a Na < 120
0.015% with a Na > 120
**2.5% with a Na < 110**
7/10
🚀Na over-correction (Na📈) as THE (only) cause of ODS/CPM: An absurd over-simplification.
Since 1980s, Na📈 has been portrayed as the main cause of CPM (so far as now the terms ODS and CPM are used synonymously).
However, finding the truth (if it exists) is more complicated.
🧵..
1/
“this bronchoscopy could have been an induced sputum”
“this A-line could have been a cuff pressure”
“this intubation for ‘airway protection’ could have been a sternal rub”
“this swan could have been a POCUS”
“this consult could have been a google search”