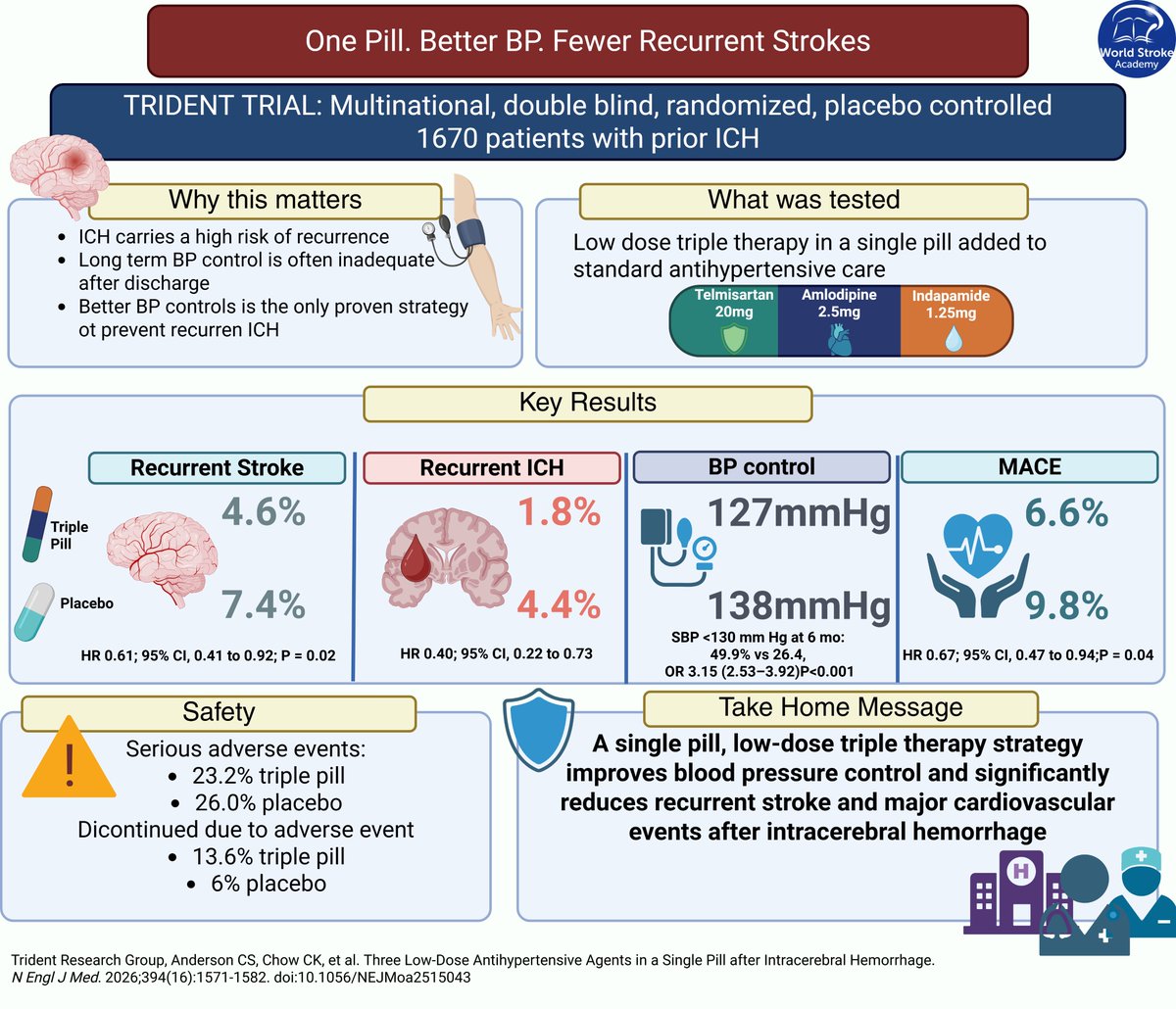
#MondayTip#TRIDENT
💊One pill could change post-ICH care.
🧠Low-dose triple antihypertensive therapy ↓ recurrent stroke by 39% and improved BP control vs standard care
☝️Simpler regimens may beat therapeutic inertia
🔗https://t.co/LUy8wIZ6dD
In-🏨 initiation of quadruple GDMT for HFrEF
(ARNI+BB+MRA+SGLTi) ▶️
Substantially improved use, adherence, persistence ▶️
Substantially improved health status, home-time, survival, and value
AHA/ACC/HFSA Class 1 recommended
Delaying to post-discharge any component = harm
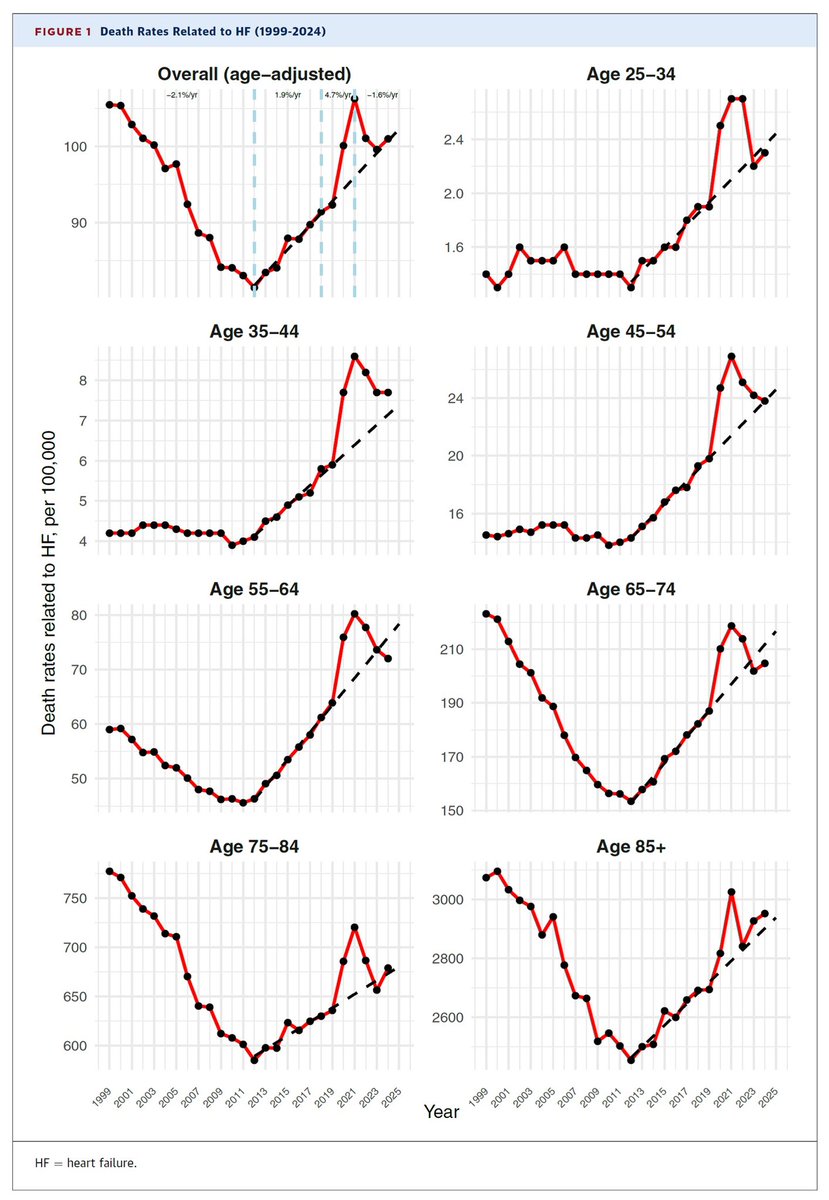
Heart failure related mortality is going…
Up, up, up
(since 2012)
While GDMT implementation in clinical practices has been going almost nowhere
Time to do something about this?
Delaying initiation of any component of foundational quadruple GDMT for HFrEF
…may seem well intentioned and prudent to assess tolerability, monitor for side effects, and judge response
Yet, 9 out of 10 patients die before receiving quadruple GDMT
Preventable ☠️s
💬 Editorial: In the VESALIUS-CV trial, evolocumab reduced major cardiovascular events in high-risk patients, including those with long-standing #diabetes, already receiving statins but not reaching LDL-C targets.
https://t.co/B16RueGnAL
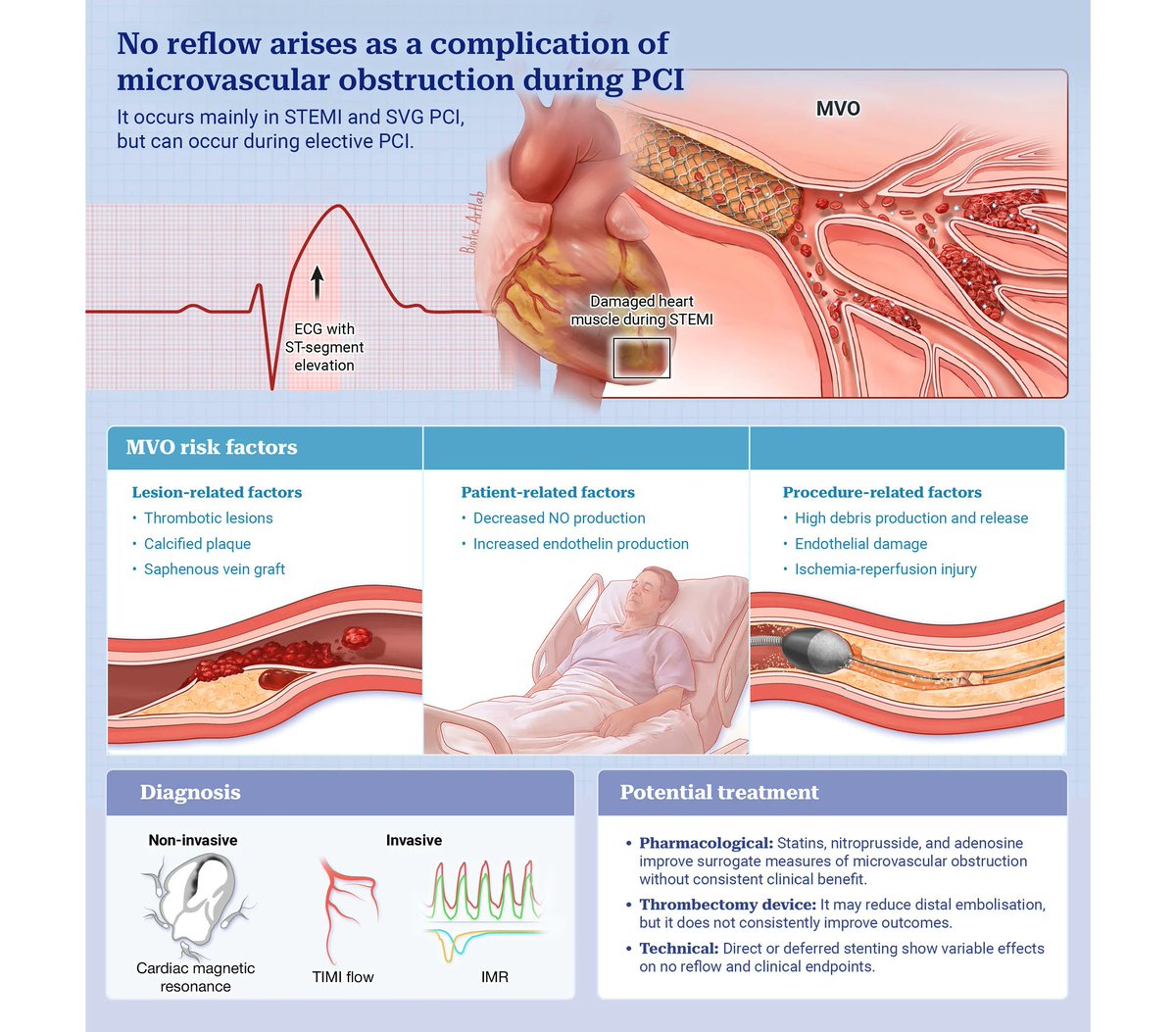
This state-of-the-art review provides a comprehensive overview of the pathophysiological mechanisms underlying the no-reflow/slow-flow phenomenon, covering invasive and non-invasive diagnostic tools, pharmacological and interventional treatment strategies, and the key clinical gaps that still need to be addressed in the field. https://t.co/glYW3u2X2z
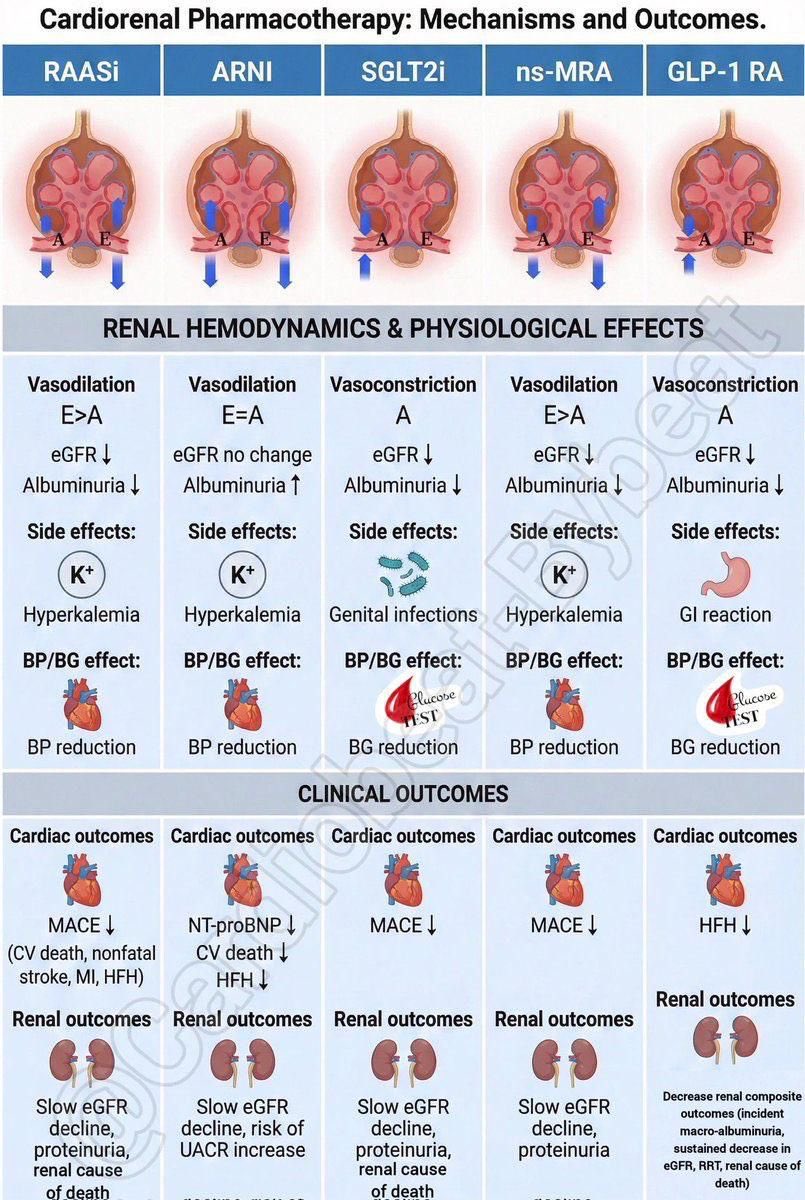
🧵 Cardiorenal pharmacotherapy cheat-sheet — 5 drug classes, one visual.
RAASi | ARNI | SGLT2i | ns-MRA | GLP-1 RA
Key patterns worth knowing:
• 4 of 5 reduce MACE or HFH
• All 5 slow eGFR decline or cut albuminuria
• Hyperkalemia risk: RAASi, ARNI, ns-MRA
• SGLT2i → genital infections | GLP-1 RA → GI side effects
Hemodynamics snapshot:
↓ eGFR on initiation is expected with most — don’t panic, it’s often renoprotective long-term.
ARNI is the outlier: eGFR no change, but watch UACR.
Save this. Share it. Your patients’ kidneys will thank you. 🫀🩺
#Cardiology #Nephrology #HeartFailure #CKD #SGLT2i #GLP1 #MedEd #CardioreналSyndrome
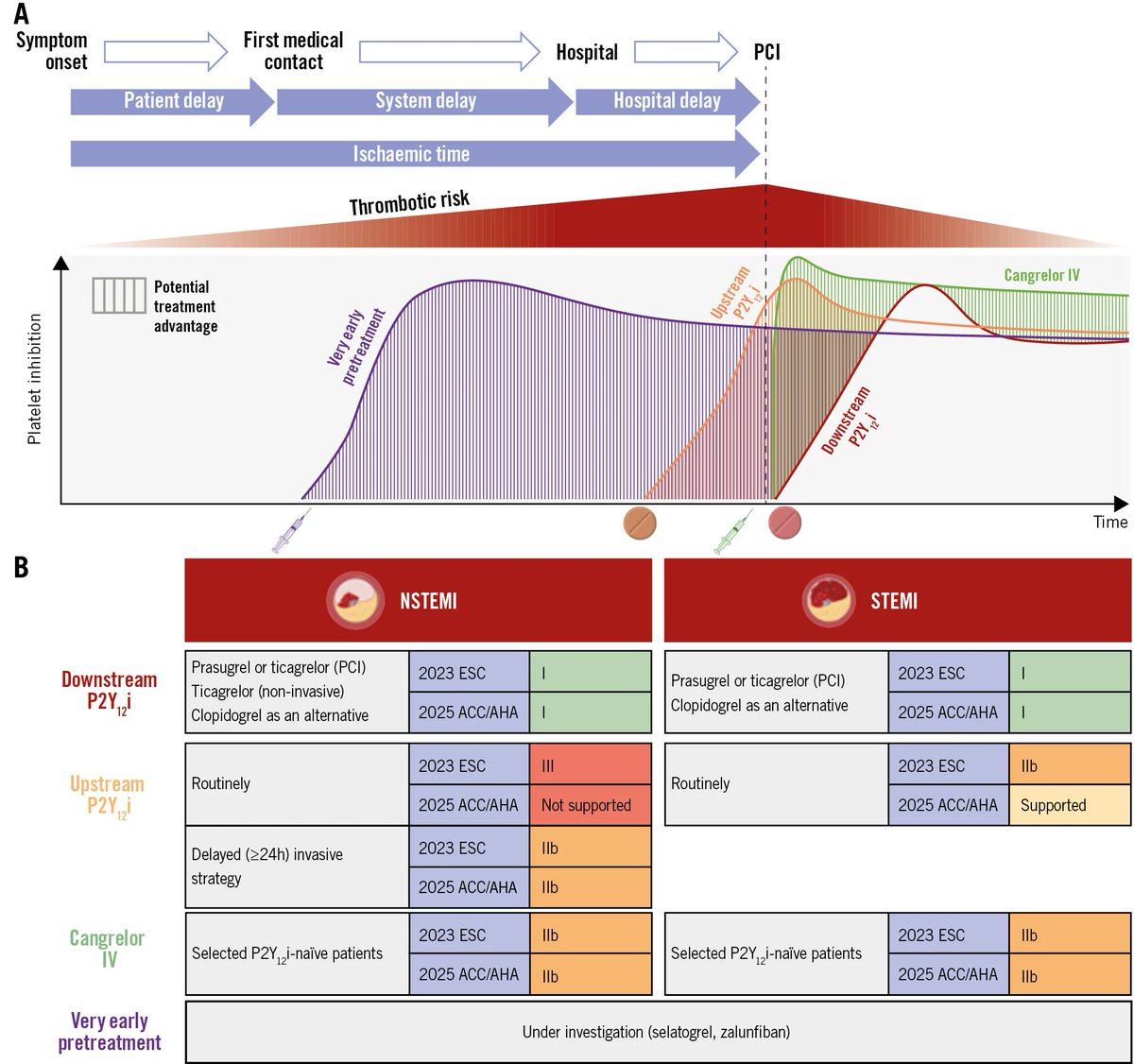
Management of patients undergoing PCI for coronary artery disease has evolved substantially, driven by early invasive strategies and changing use of oral antiplatelet pretreatment. This review synthesizes current evidence on antiplatelet pretreatment across NSTE-ACS, STEMI, and stable disease, and examines emerging data on novel parenteral therapies. https://t.co/pLcvgIZO5E
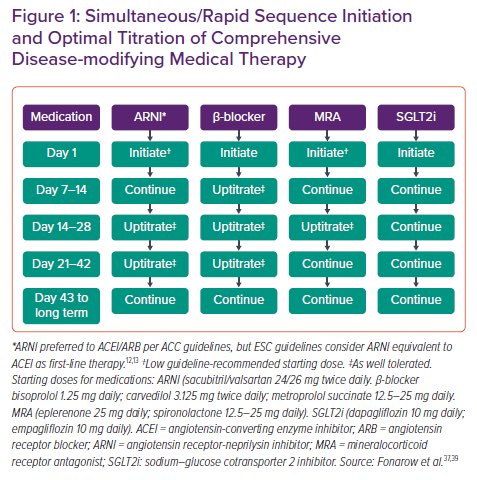
The Gap to Fill: Rationale for Rapid Initiation and Optimal Titration of Comprehensive Disease-modifying Medical Therapy for Heart Failure with Reduced Ejection Fraction
Despite an abundance of evidence for the benefit of HFrEF medical therapy, data from the US and around the world suggests that the use of GDMT and CDMMT has substantial treatment and dosing gaps
#Cardiology #MedTwitter #CardioTwitter #HeartHealth #Healthcare
@gcfmd@SJGreene_md@mvaduganathan@EJHFEiC@BiykemB@DrMarthaGulati@hvanspall@ankeetbhatt@cardioceptor
https://t.co/xm1ZrVed8D
Discontinuation of RAS Inhibition After an Acute Decline in Estimated Glomerular Filtration Rate
This cohort study found that discontinuation of RASIs after an acute decline in eGFR was associated with ESKD and death compared with continuing RASIs. These findings suggest that further study is needed to understand reasons for frequent discontinuation of RASIs and devise strategies to improve their persistent use.
#Cardiology #MedTwitter #CardioTwitter #HeartHealth #Healthcare
@mvaduganathan@hvanspall@ankeetbhatt@SJGreene_md@gcfmd@BiykemB@ShelleyZieroth@goKDIGO
https://t.co/9kcxRXYIAj
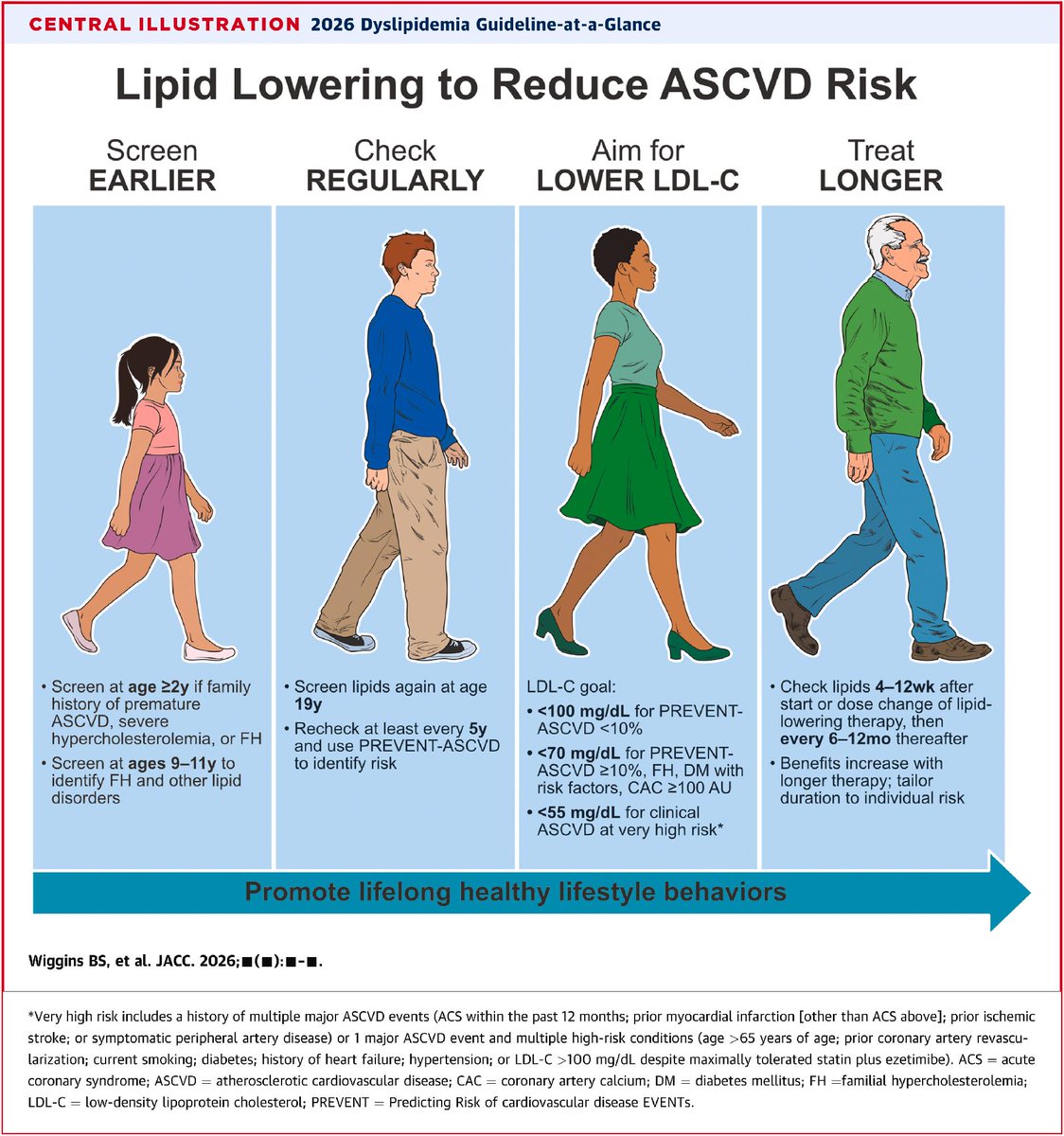
🆕 ACC/AHA Guideline on the Management of Dyslipidemia offers a comprehensive “one-stop shop” for addressing the evaluation, management & monitoring of individuals w/ dyslipidemias.
Read the full guideline in #JACC: https://t.co/rhUKNIRRL4 #cvLipids#ClinicalGuidelines
🫀📉 Can more intensive LDL-lowering improve CT-FFR in stable chest pain?
This new JACC study evaluates whether intensive lipid-lowering therapy (statin + ezetimibe) alters CT-derived fractional flow reserve (FFR-CT) — a noninvasive marker of lesion-specific ischemia — in patients with stable chest pain and coronary atherosclerosis.
🔍 Study essentials
Patients with stable angina and coronary plaque on CT angiography were managed with aggressive lipid-lowering using statins plus ezetimibe, targeting substantial LDL-C reduction. FFR-CT was measured at baseline and on follow-up to assess functional changes in coronary physiology attributable to therapy.
📈 Key message
The core focus — integrating structural and functional imaging — points to a key concept: lipid-lowering can potentially improve lesion physiology, not just plaque burden. By using FFR-CT (a validated surrogate for invasive FFR), the authors are examining whether aggressive LDL-reduction actually shifts physiological indices toward less ischemia.
🧠 Why this matters
Lipid-lowering benefits have traditionally been shown at the event level (MI, death).
Structural plaque regression with statins/ezetimibe is documented in IVUS and CT studies.
But fewer data exist on functional improvement in coronary blood flow with therapy.
Linking lipid therapy to improved FFR-CT suggests that LDL-lowering may not only slow plaque progression but also improve coronary physiology — a potential mechanistic bridge to clinical benefit.
📌 Bottom line:
Intensive lipid-lowering might influence not only plaque morphology but lesion-specific ischemia as assessed noninvasively, expanding our understanding of how therapies translate into physiological improvement.
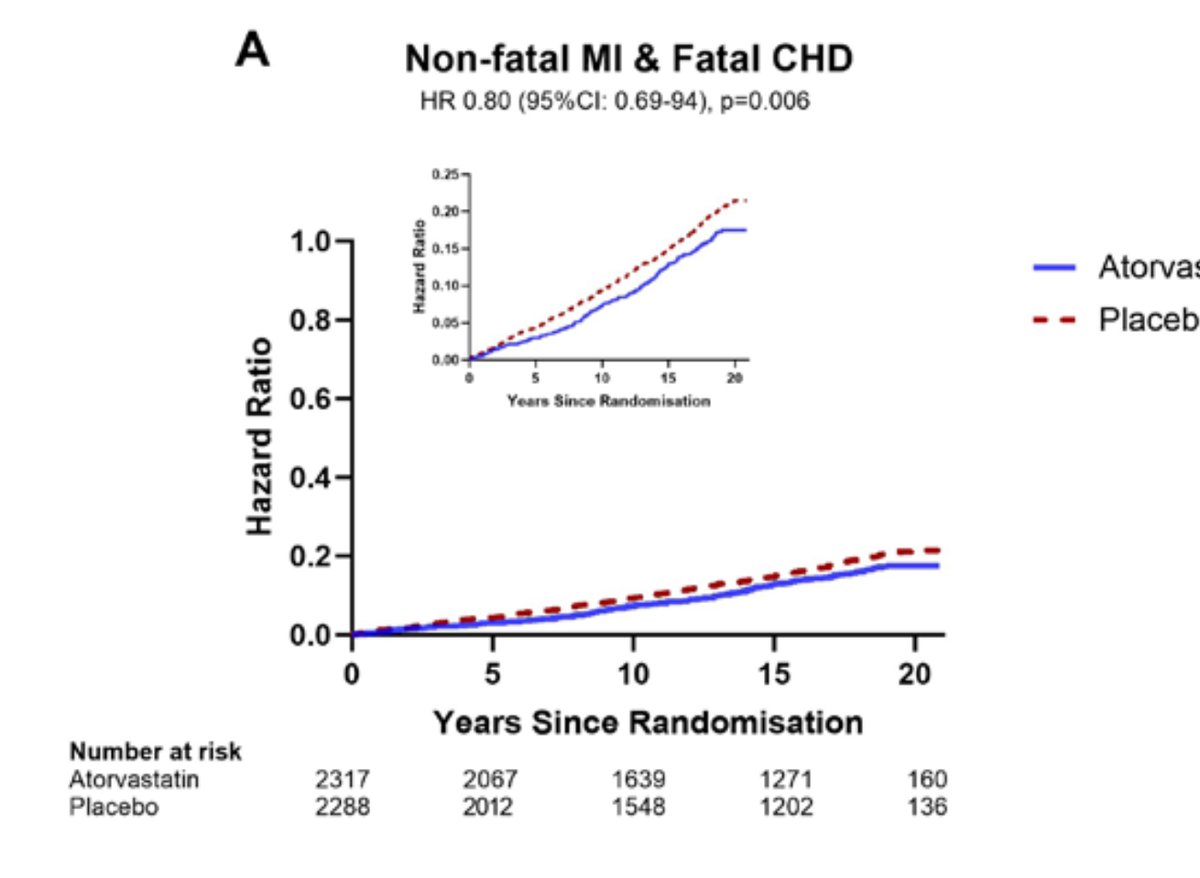
🤔“Statins add 4 days”
❌No
💔They prevent heart attacks for decades
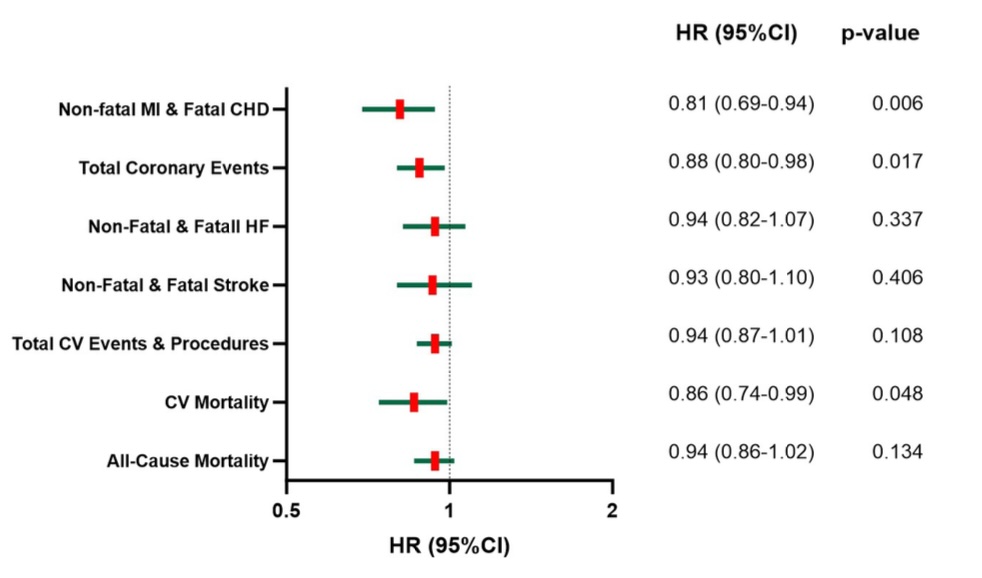
👉ASCOT-Legacy, 20-year follow-up
• ↓ MI + fatal CHD: 19%
• ↓ Total coronary events: 12%
• ↓ CV mortality: 14%
👆And the lower the achieved LDL during the trial, the lower the long-term risk:
Every 1 mmol/L LDL reduction →
31% less MI/CHD
34% less CV death
👉The original RCT lasted 3.3 years
👉The benefit persisted 20 years
📍That’s not “4 days”
📍That’s altering the natural history of atherosclerosis
📍If you truncate survival curves at 4 years, you’ll measure days
📍If you follow patients for decades, you’ll measure prevented infarctions and lives saved
🔗Open Access https://t.co/3IbVELE6qI
@society_eas@mmamas1973@DrMarthaGulati@Drlipid@ethanjweiss@purviparwani@BarteltLab
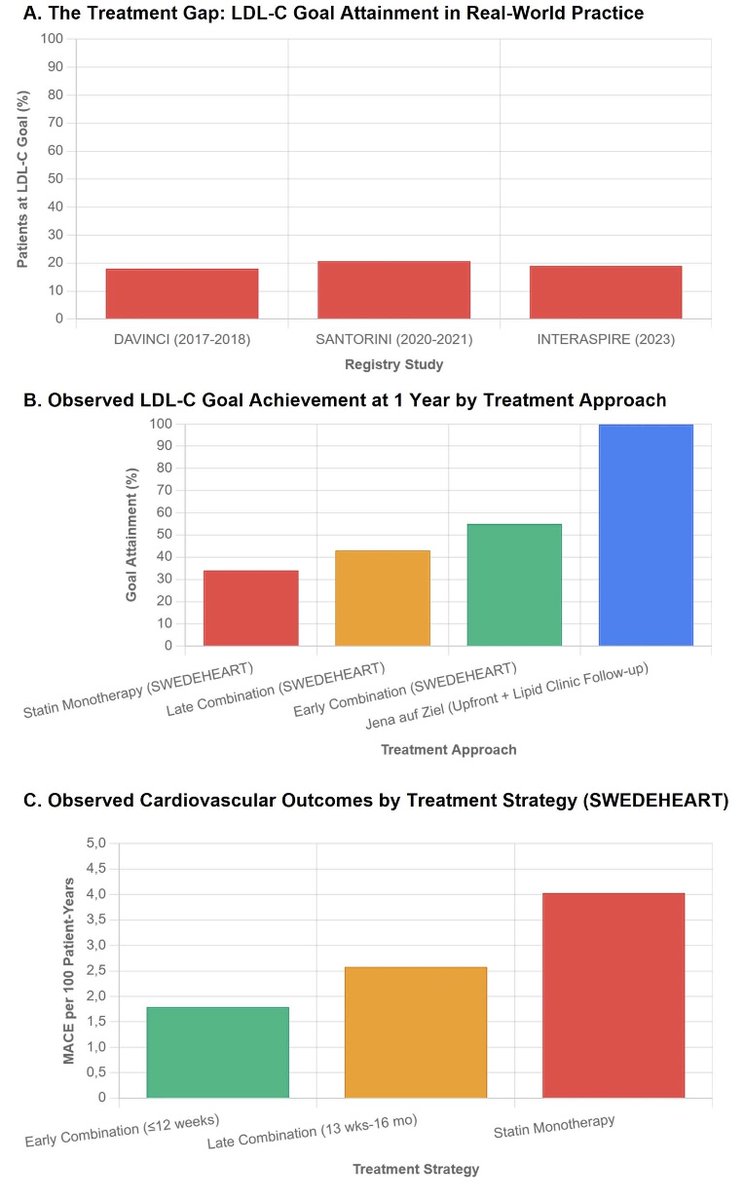
👉 Combination Lipid-Lowering Therapy After ACS: Should this be the New Standard of Care?
👆 LDL-C reduction after ACS shows a log-linear relationship with CV risk reduction, regardless of the drug used. Lower is better. Earlier is better.
👆 Guidelines have moved: ESC/EAS and ACC/AHA now endorse earlier and deeper LDL-C lowering, including upfront combination therapy in selected (or many) patients.
👆 Real life hasn’t caught up: <20% of post-ACS patients reach LDL-C <55 mg/dL. The stepwise “wait-and-see” model fails—predictably.
📍 Evidence is consistent:
IMPROVE-IT, RACING, LODESTAR → combination therapy works, is safe, and improves goal attainment.
ODYSSEY OUTCOMES, FOURIER → add PCSK9 inhibition and events drop further, especially when started early.
📍 Imaging doesn’t lie: PACMAN-AMI and HUYGENS show faster plaque regression and fibrous-cap thickening with early intensive therapy.
📍 Registries (SWEDEHEART, INTERASPIRE): early statin + ezetimibe beats late intensification or statin alone—both for LDL-C targets and hard outcomes.
👆 Fear of “too low LDL-C” is obsolete: benefits persist down to ~20 mg/dL, with no signal for harm. Cholesterol biology is robust; atherosclerosis is not.
📍 Bottom line:
After ACS, default early combination therapy (high-intensity statin + ezetimibe) is not aggressive—it’s rational. Precision medicine is great, but undertreatment kills first.
🔗 Open Access https://t.co/AkTlEYCnyg
@society_eas