Delighted to announce that today I joined the fantastic team @MTWnhs as a Consultant Colorectal & General Surgeon! Excited to get started at what is a very exciting time for our department, and overwhelmed by the support from my new colleagues across the board. Here’s to 2024!
Hypermutator cancers are defined by increased mutation rates.
But do mutation rates evolve with time during tumour growth?⏱️
In this work @NatureGenet we show that hypermutator cancers use an unexpected set of genetic gear switches to adapt mutation rates to immune selection.
Really exciting news this morning that my oncology colleague Dr Vicky Kunene @uhbtrust dosed the first patient in the BioNTech BNT-122 mRNA vaccine trial for personalised therapy in colorectal cancer - @UHBResearch was the first site in UK to do this:
https://t.co/7ZKzhL9JWY
@adbeggs@mstotty88 Totally agree. The days of taking someone off to theatre for complications of a hernia or severe abdo pain with no imaging are largely over. We need to be armed with as much info as we can safely obtain to deliver the best outcomes. Rarely that balance will mean an immediate op.
@AmitBharath Yes, because it’s not what you get referred that should worry you, it’s what you don’t get referred and is sitting elsewhere, getting worse
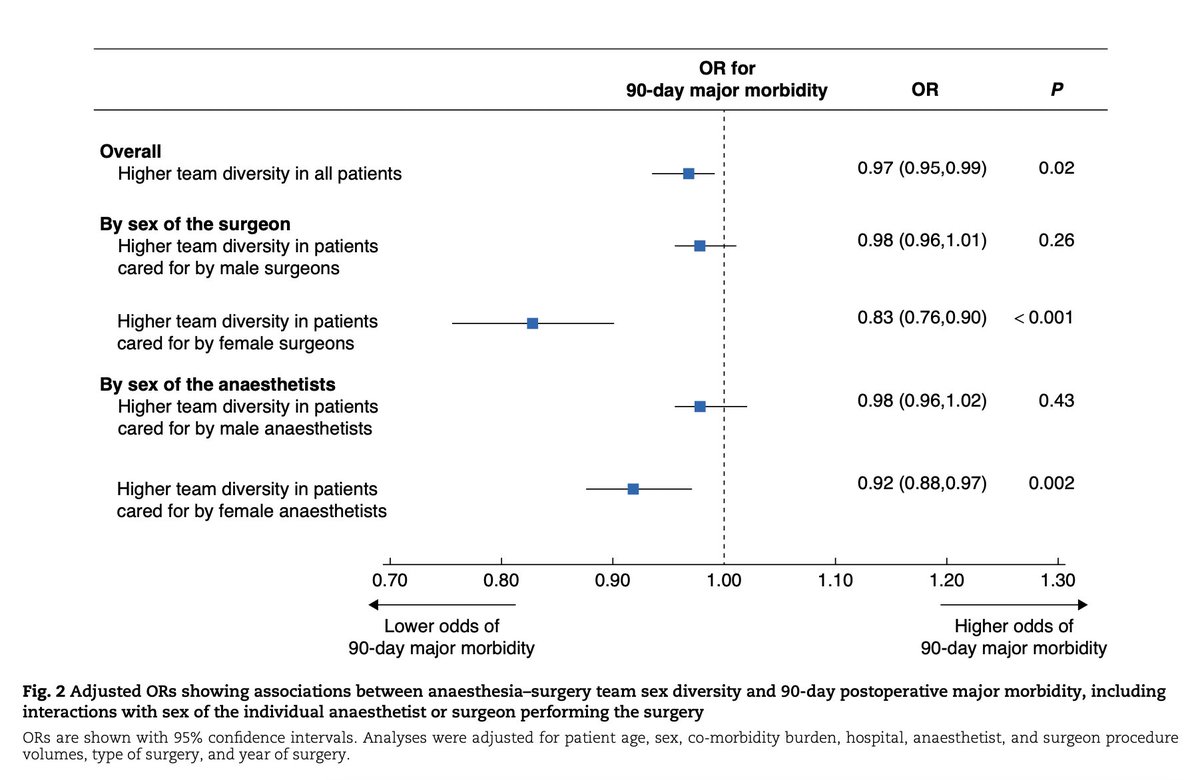
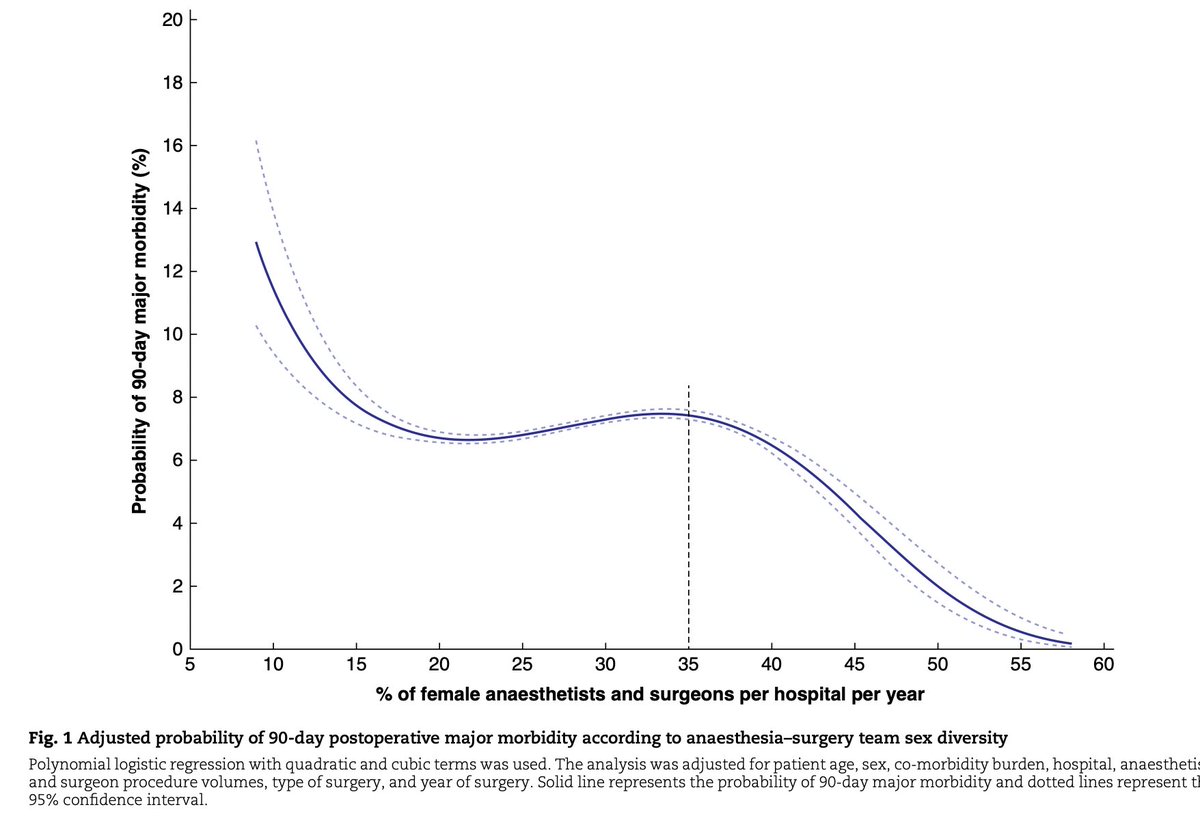
Association between anaesthesia–surgery team sex diversity and major morbidity
➡️ https://t.co/TJP1v1MWML
In this population-based cohort study of 709 899 patients undergoing major inpatient operations, care in a hospital reaching a critical mass of over 35% female anaesthetists and surgeons was independently associated with 3% lower odds of 90-day major morbidity.
Increasing team sex diversity to reach a critical mass of female anaesthetists and surgeons could contribute to improving patient outcomes.
Great work by Julie Hallet, Rinku Sutradhar, Alana Flexman, Daniel I McIsaac, François M Carrier, Alexis F Turgeon, Colin McCartney, Wing C Chan, Natalie Coburn, Antoine Eskander, Angela Jerath, Pablo Perez d’Empaire, Gianni Lorello
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @RCPSGTrainees @aecirujanos@SEIQuirurgica@iss_sic #MedicalTechniques @BJSAcademy@young_bjs@BJSOpen@des_winter@evanscolorectal@robhinchliffe1@bplwijn@ksoreide@MalinASund@nfmkok@TejedorPat@paulo_sutt@PVaughanShaw@JJEarnshaw@juliomayol
Surgery for advanced neuroendocrine tumours of the small bowel: recommendations based on a consensus meeting of the European Society of Endocrine Surgeons (ESES)
➡️https://t.co/dIZfpak81K
This paper provides evidence-based recommendations on the surgical management of locally advanced and metastatic small bowel neuroendocrine tumours, primary tumour resections in the setting of metastatic disease, and surgical indications for grade 3 small bowel neuroendocrine tumours and small bowel neuroendocrine carcinomas.
The recommendations are the result of a working group of experts, created by the European Society of Endocrine Surgeons. The group addressed 11 relevant clinical questions regarding surgery for advanced disease, emphasizing and confirming the key role of the surgeon for advanced small bowel neuroendocrine tumours.
Great work by Klaas Van Den Heede, Dirk-Jan van Beek, Sam Van Slycke, Inne Borel Rinkes, Olov Norlén, Peter Stålberg, Erik Nordenström
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @RCPSGTrainees @aecirujanos@SEIQuirurgica@iss_sic #MedicalTechniques @BJSAcademy@young_bjs@BJSOpen@des_winter@evanscolorectal@robhinchliffe1@bplwijn@ksoreide@MalinASund@nfmkok@TejedorPat@paulo_sutt@PVaughanShaw@JJEarnshaw@juliomayol #endocrine @IfsoSecretariat
@TUIUK your call centre reps are v courteous but today has been a masterclass in not following through on ‘promises’. Told by 2 separate agents they would call by COP re: substantial changes you have had to make to our hol and to make alt booking before everything goes. Nothing
@DrNeilStone It’s fair to say one size doesn’t fit all. There are a select, highly talented few who could comfortably obtain the competencies/experience for CCT in General Surgery (in the current NHSE work climate) by the age of 34, but most of us are mortal. I’m grateful for my extra years…
@lizzyelsey@jamestoml1 Delighted to hear this! I have been similarly welcomed and supported by the brilliant team @MTWnhs. Good luck Lizzy - I had my first rodeo last weekend!
@adbeggs@charlot_summers There is a element of endless obfuscation/closed doors to those of us who chose not to take the formal NIHR ACF/CL route and yet have both achieved PhD and want to continue as clinical academics. There are more of ‘us’ around than is perceived - a significant untapped resource
Important secondary analysis of the OPRA trial with a median f/u of 4 years.
This provides important details from a landmark study, and can help guide patient counseling. Of note, it's not broken down to compare induction TNT to consolidation TNT.
My analysis is long-winded, and the target audience is surgeons who offer organ preservation to patients with rectal cancer:
Patients with a cCR at restaging: 98% offered organ preservation/watch-and-wait (WW), of which 22% experienced local regrowth. Patients with a sustained cCR had a 5% rate of distant metastases.
Of the local regrowths, 93% underwent salvage TME and 7% underwent salvage local excision. For these patients, 33% developed recurrence (4% local, 22% distant, and 7% local+distant).
_______________________________________
Patients with a near-complete CR at restaging: 20 (17.5%) went straight to surgery, of which only 3 (16%) had a pathologic CR (pCR). Recurrence after upfront TME for near-cCR was 30% (15% local, 10% distant, 5% local+distant). These numbers were small (n=3 for local recurrence) and should be interpreted with caution.
Of the remaining 94 patients (82.5%) who underwent WW, 48 (51%) developed local regrowth. Salvage TME was performed in 34 patients (71% compared to 93% for cCRs). 2 of 34 TMEs (6%) had a pCR.
For patients with a near-cCR who developed regrowth after WW, 33% developed recurrence (4% local, 21% distant, 8% local+distant).
Of the 46 patients (40%) with a near-cCR who remained in the WW program, 13% developed distant metastases (compared to 5% for cCRs).
______________________________________
Patients with an incomplete response at restaging:
88% were offered upfront TME, of which 4/51 (8%) had a pCR. For ICR and upfront TME, recurrence rate was 35% (3.5% local, 21% distant, 10.5% local+distant).
8 patients with incomplete response were still enrolled in WW for different reasons, of which 5/8 (63%) developed local regrowth. All 5 underwent TME, and the local recurrence was 20% (1/5). Of the 3/8 that remained in WW without regrowth, 2/3 (66%) developed lung metastases.
_______________________________________
Overall, the 3-year organ preservation rate was 77% for cCRs and 40% for near-cCRs. The median time to TME for near-cCRs was 1 year.
3-year DFS was 88% for cCR, 69% for near-cCR, and 56% for incomplete response.
_____________________________
For patient counseling purposes:
Of the 123 patients with a cCR who were offered WW, the local recurrence rate was 22% (0f which 93% underwent salvage TME) and the rate of distant metastasis was 10.5%.
Of the 94 patients with a near-cCR who were offered WW, local recurrence rate was 51% (of which 71% underwent salvage TME) and the rate of distant metastasis was 15%.
Of the 57 patients with incomplete response who were offered upfront TME, local recurrence was 14% and the rate of distant metastasis was 32%.
@JohnRTMonsonMD@R_Perez_MD@ianmpaquette@JonVogel7@jendavidsmd@KyleCologne@debby_keller@juliomayol@Neil_J_Smart@FergaljFleming@ScottRSteeleMD@JISBMD
Delighted to announce that today I joined the fantastic team @MTWnhs as a Consultant Colorectal & General Surgeon! Excited to get started at what is a very exciting time for our department, and overwhelmed by the support from my new colleagues across the board. Here’s to 2024!
"Hartmann’s procedure no longer has a role in colorectal surgery" is way too strong of a hypothesis.
All retrospective data on HP vs protected anastomosis suffers from selection bias.
RCTs never worked due to low accrual, which is ALSO selection bias, although appropriate, ie decisions at 2am that "this one is too sick for the trial."