Professor @TuftsMedSchool, Co-Founder @Naveris_inc. Dedicated to understanding the biological, molecular, and genetic underpinnings of cancer & prevention.
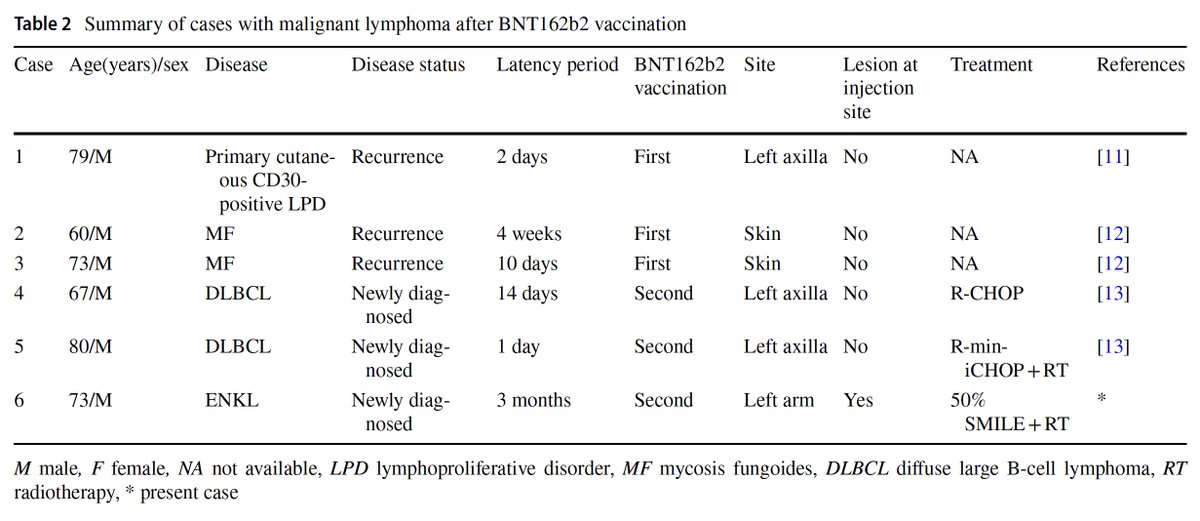
Important case of a 73 year old man with extranodal NK/T cell lymphoma at the injected left arm after BNT162b2 mRNA COVID-19 vaccination 3 months earlier. The authors described 5 other cases with recurrence of T-cell lymphoma or newly diagnosed diffuse large B-cell lymphoma (DLBCL) shortly after BNT162b2 mRNA vaccination.
https://t.co/damIUEZQHC
I’m holding a hearing tomorrow at 2:30pm ET: “Plausible Mechanisms of COVID-19 Injections Causing Cancer and Attacks on Scientific Publications and Research.”
We’ll hear from 6 doctors and a cancer survivor:
- Angus Dalgleish, M.D.
- @weldeiry
- @SabinehazanMD,
- Saskia Mostert, M.D., PH.D.
- @DrAseemMalhotra
- @jrgralow
- Tamika Felder
Tune in on my X account and find more information at the link below⬇️
I’m excited to participate in the #PresCancerPanel meeting on June 8–9.
This meeting will focus on modifiable risk factors for cancer & potential approaches to reduce cancer risk in the United States.
Check it out: https://t.co/v3eumIse9U.
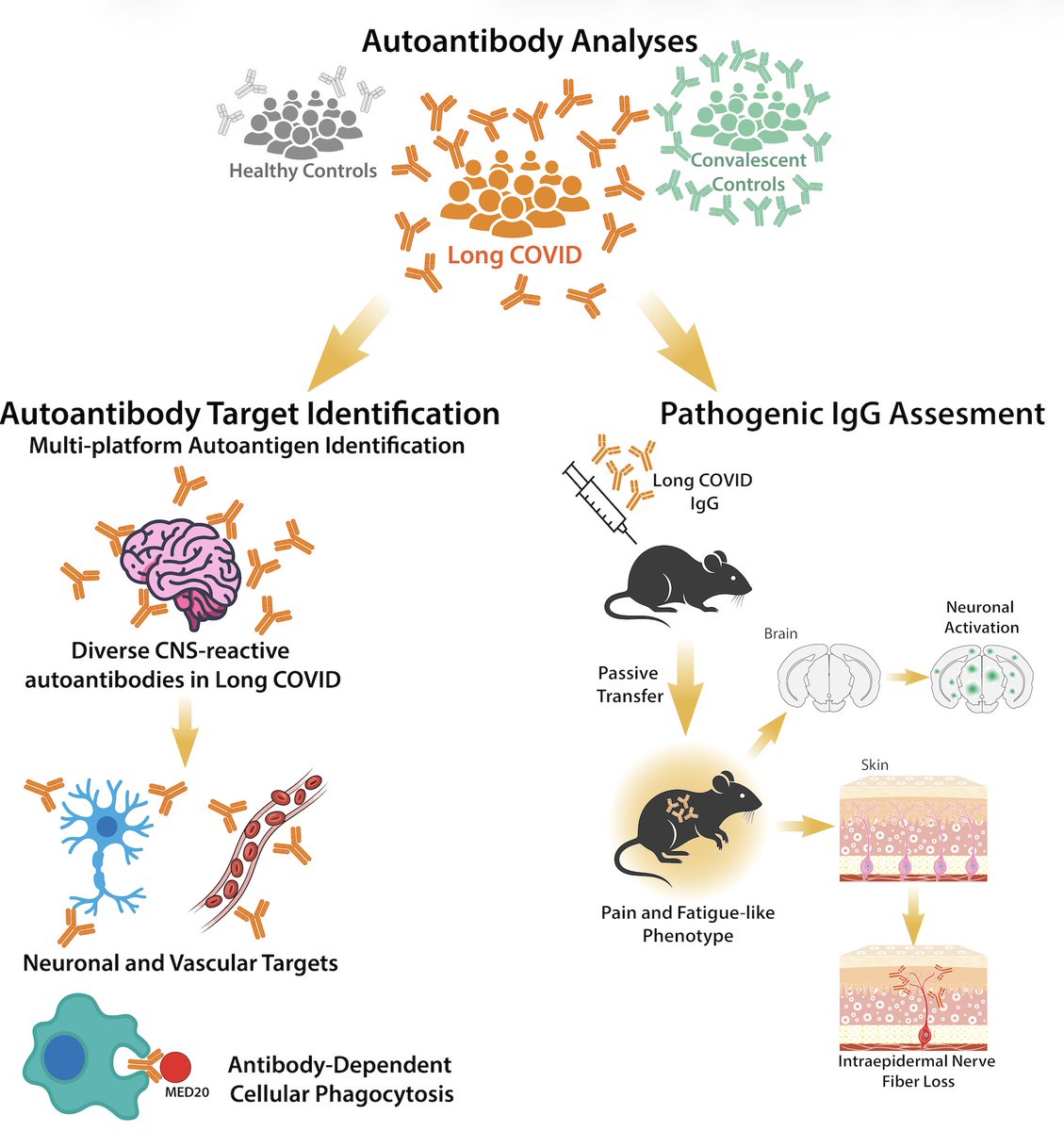
Excited to share our study by @keylas3 et al. on pathological autoantibodies in people with Long COVID. We asked whether IgG in patients with Long COVID bind to human tissues/antigens and cause pathologies when transferred into mice. With @PutrinoLab
https://t.co/tcowCufWyf
@elonmusk No — a synthetic RNA strand cannot “basically cure anything.”
That is Silicon Valley biology, not actual biology.
Synthetic RNA can be powerful. It can tell cells to make a chosen protein. But diseases are not just software bugs waiting for the right line of code.
Cancer, autoimmunity, neurodegeneration, metabolic disease, and chronic inflammatory disorders involve complex tissues, immune responses, genetics, epigenetics, timing, dose, and cellular context.
The hard problems are not just “what sequence do we write?” The hard problems are where it goes, which cells take it up, how long it lasts, how much protein is made, what the immune system does in response, and what unintended effects follow.
And then there is the still-unresolved issue of DNA contaminants and other manufacturing byproducts in synthetic RNA products. Until FDA and other regulators impose rigorous, transparent, product-specific standards, sweeping claims about this platform’s safety and curative power are premature at best.
RNA is a tool.
It is not magic.
And “programmable” does not mean “safe,” “specific,” or “curative.”
Here’s a radical idea: what if we actually funded cancer prevention?
Not just better screening. Not just earlier detection. Prevention.
That means studying, regulating, and when necessary eliminating the hundreds — likely thousands — of environmental chemicals with carcinogenic potential, including both genotoxic agents that directly damage DNA and non-genotoxic compounds that disrupt hormones, inflammation, immune surveillance, development, and tissue repair.
We spend billions treating cancer once it appears. Why are we still so reluctant to ask what is helping cause it in the first place?
Because there are at least 70 papers in the scientific literature that have reported an association between cancer and COVID (both infection and vax) and the FDA and many are ignoring this. This must be studied…not dismissed.
In addition the FDA states clearly that mRNA vaccines have not been tested for carcinogenicity yet everyone seems to believe this means that they are not carcinogenic. There is literally no data or evidence on this.
And finally, the FDA (6 years out) as still failed to provide data related to the fate of the DNA impurities in mRNA vaccines and have failed to establish evidence based regulatory guidance on the manufacturing of these products. Residual DNA does have long/term health and safety implications.
A single paper showjng an association between DES and cancer was sufficient for the FDA to act.
I get your point- I'm just pointing out that it is overly simplistic to keep pointing to crude population-level incidence trends which can obscure relationships because cancer is heterogeneous, latency is variable, exposures are uneven, and screening/diagnosis changes confound the signal.
Some glaring examples of this include DES and clear-cell adenocarcinoma, asbestos and mesothelioma, radon and lung cancer.
This last one is particularly relevant here because radon is known to cause lung cancer, but this signal is masked in population-level data since smoking is such a dominant risk factor and radon exposure varies dramatically by geography and by household...
There are 87,000 chemicals in our environment, only 2-3% that have ever been tested for carcinogenicity. I will not pretend to know what the dominant driver of NHL and leukemia is- and especially in Norway. My expertise is in breast cancer and I'm more than happy to show you data on the endocrine disrupting chemicals that are driving early onset breast cancer trends there.
And now you're bringing up something totally different....I was not talking about "tubro cancer" but if you're referring to the many reports of tumor hyperprogression then you're more likely to see a shift in the stage at diagnosis rather than simply increased incidence.
In fact you might see that early onset cancers, which we have been seeing rise pre-covid might be presenting at advanced stage, larger tumor burden, metastatic disease, or shorter interval between prior normal evaluation and diagnosis.
And mortality may rise only if the effect is large and lethal enough.
No. Mortality data and incidence data measure two different things. Mortality is not a direct mirror of incidence.
1. Mortality lags incidence.
2. Mortality is affected by treatment.
3. Some cancers have high survival.
4. Younger-onset cancer may not immediately affect mortality curves.
I didn't argue that. My point was Alex was claiming "New data shows mRNA Covid shots don't have a long-term cancer risk" and that statement is simply not accurate. Crude population-level data is not the right way to assess this.
And I was not cherry picking data- I was looking at the trend lines. For the fast-latency cancers like NHL and leukemia, those trend lines have been steadily and steeply rising for years....which I specifically called out. There clearly is a signal with those cancers and it predates COVID. If there is already a strong underlying driver pushing those trends seeing a COVID signal will be difficult using the aggregate data. This is akin to the radon association with lung cancer. One cannot see the radon signal in crude population-level data because it is masked by the smoking signal...
And my point about pancreatic and stomach cancers was simply that perhaps a new trend line is starting to form and if it continues that may represent a COVID-associated signal.
Again- puzzled why everyone is so quick to dismiss.
I don't see how everyone can be so confident in dismissing any association when there has been no data either way on this....
Early onset cancer incidence is rising and has been for decades. There are underlying environmental factors driving this that are completely independent from COVID.
That doesn't mean there is no signal from COVID-it may simply be that the signal is not yet strong enough (too early) to be seen at the population level
The cancer signal from DES exposure took ~20–30 years to become apparent. So did the asbestos signal. Depending on when you start the clock, it took 40-70yrs to see the radon signal.
We are only 6 years out....it is too early to see such a population-level signal with COVID unless something pops up in rare cancers where the statistics will show somethign sooner