🌸 THE 10 MOST IMPORTANT BREAST CANCER TRIALS OF #ASCO26
Chicago is loaded this year.
From ctDNA-guided endocrine switching to frontline ADCs and next-gen HER2 platforms, these are the studies most likely to shape breast oncology practice 👇
🩷 HR+ / HER2- DISEASE
1️⃣ persevERA BC (LBA1006)
Giredestrant + palbociclib vs letrozole + palbociclib in 1L metastatic disease
Despite missing the primary PFS endpoint, biomarker/subset analyses may define where oral SERDs still fit.
2️⃣ SERENA-6 (LBA1007)
Camizestrant for emergent ESR1 mutations detected via ctDNA BEFORE radiographic progression
Possibly the biggest ctDNA-guided endocrine strategy discussion of the meeting.
3️⃣ VIKTORIA-1
Gedatolisib + fulvestrant ± palbociclib after AI + CDK4/6i progression
Huge unmet-need population.
Post-CDK4/6 sequencing remains one of the biggest HR+ questions.
4️⃣ lidERA BC (Abstract 502)
Adjuvant giredestrant in early ER+/HER2- disease
Moving oral SERDs into curative-intent therapy.
5️⃣ FOURLIGHT-2 (Abstract 1042)
Next-gen CDK4-selective inhibition with atirmociclib + letrozole
Can we reduce neutropenia while preserving efficacy?
🔥 TNBC & ADC ERA
6️⃣ ASCENT-04 (LBA1000)
Sacituzumab govitecan + pembrolizumab vs chemo + pembrolizumab in PD-L1+ mTNBC
Could ADC + IO combinations become the frontline standard?
7️⃣ TROPION-Breast02
Dato-DXd vs chemotherapy in metastatic TNBC
A major test of the “ADC-first” paradigm.
🎯 HER2+ & NEXT-GEN NEOADJUVANT PLATFORMS
8️⃣ KN026-004 (LBA660)
Novel biparatopic HER2 antibody vs classic CLEOPATRA-style therapy
Watch the pCR data carefully.
9️⃣ I-SPY 2.2 (LBA514)
Rilvegostomig + T-DXd in high-risk HER2-negative disease
IO + ADC combinations continue moving earlier.
🔟 DESTINY-Breast05 Update
Long-term outcomes for T-DXd vs T-DM1 in residual HER2+ disease
Which breast abstract are you watching most closely?
#BCSM #OncoTwitter #ASCO26 #BreastCancer #MedEd @asco@myesmo@esmo_open@OncoAlert@OncBrothers
🚨🚨🚨
RASOLUTE-302 Ph3 is POSITIVE
"Daraxonrasib demonstrated a median OS of 13.2 months versus 6.7 months for chemotherapy, with a hazard ratio of 0.40 (p < 0.0001)".... WOW!
AMAZING news for patients with #PancreaticCancer
The RAS Revolution is ON!!
https://t.co/I59NNWRB1O
#ADC#B7H4
Targeting B7-H4 is beginning to show a growing number of positive signals✅, especially when used with ADCs, in several tumors
-Adenoid Cystic Ca
-Platinum resistant ovarian Ca
-TN breast Ca
The "relative" of PD-L1 (aka B7-H1🤯)
@OncoAlert@brunolarvol
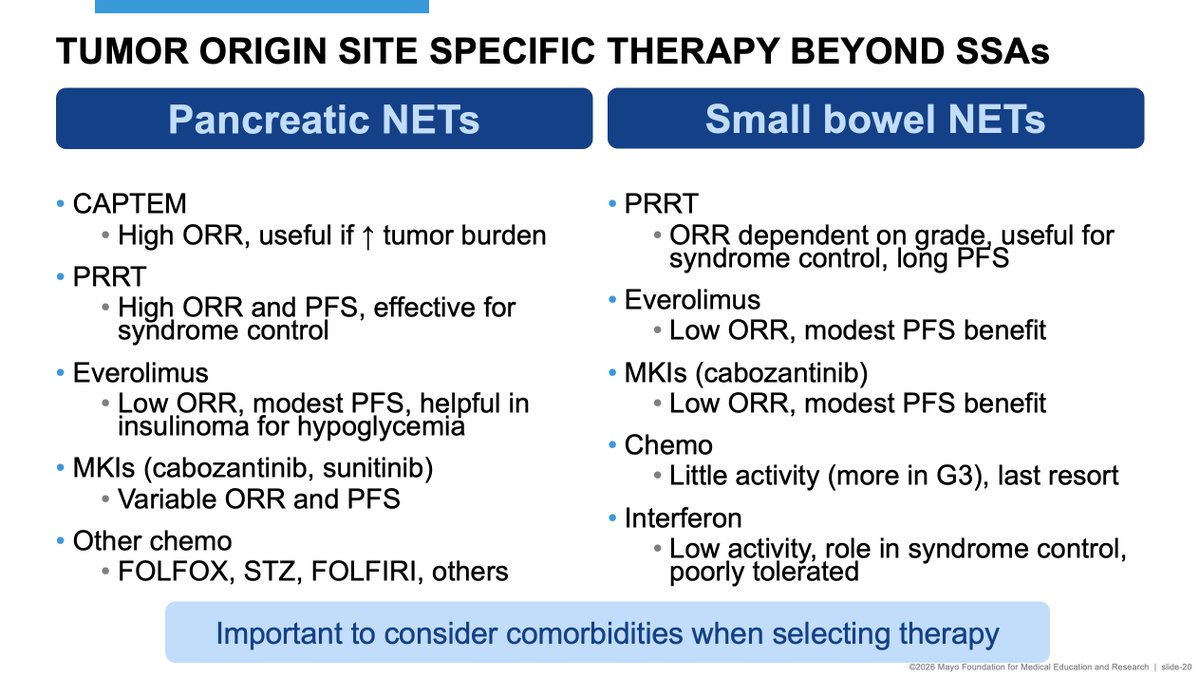
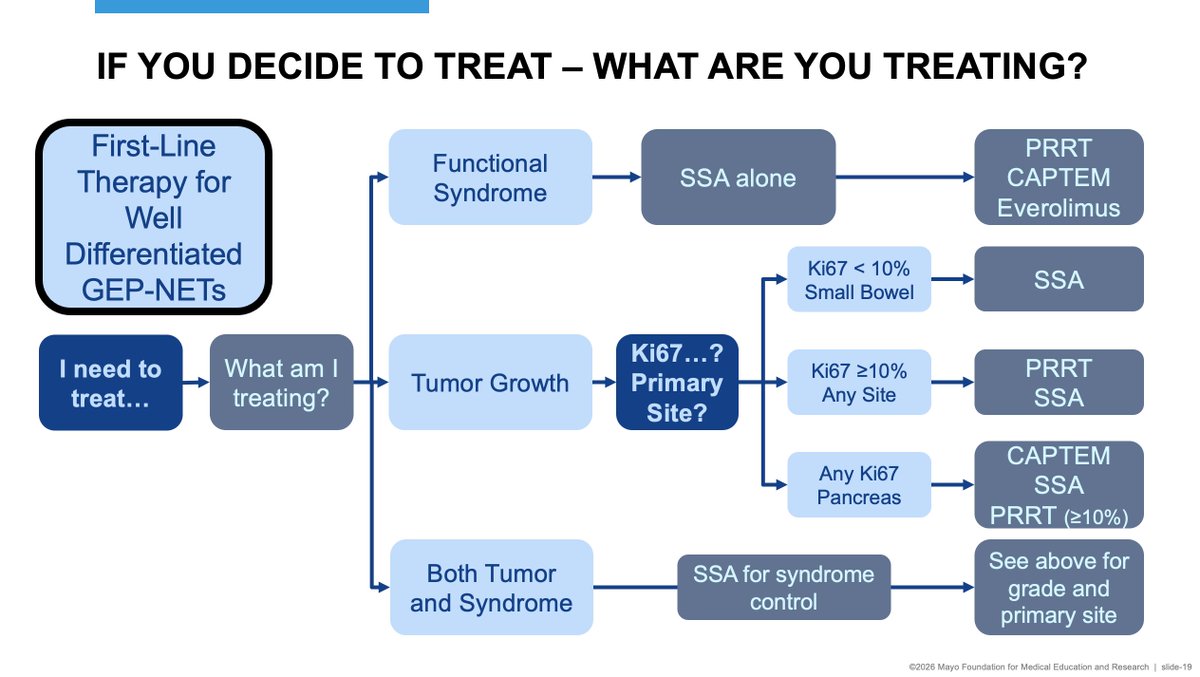
Time for another NET talk - this time on sequencing of systemic therapy. Another excellent @MayoMedEd offering. If you are looking for a good course in pretty much anything in Med Ed, check them out. They have a huge selection of quality courses, not just in oncology.
So how to we select initial therapy for advanced NETs when resection or other regional therapy is not a good option...? Below are some thoughts, as always open to criticism and and comments (snarky comments also welcomed if you feel so inclined...).
Come join us for future Mayo Clinic conferences!
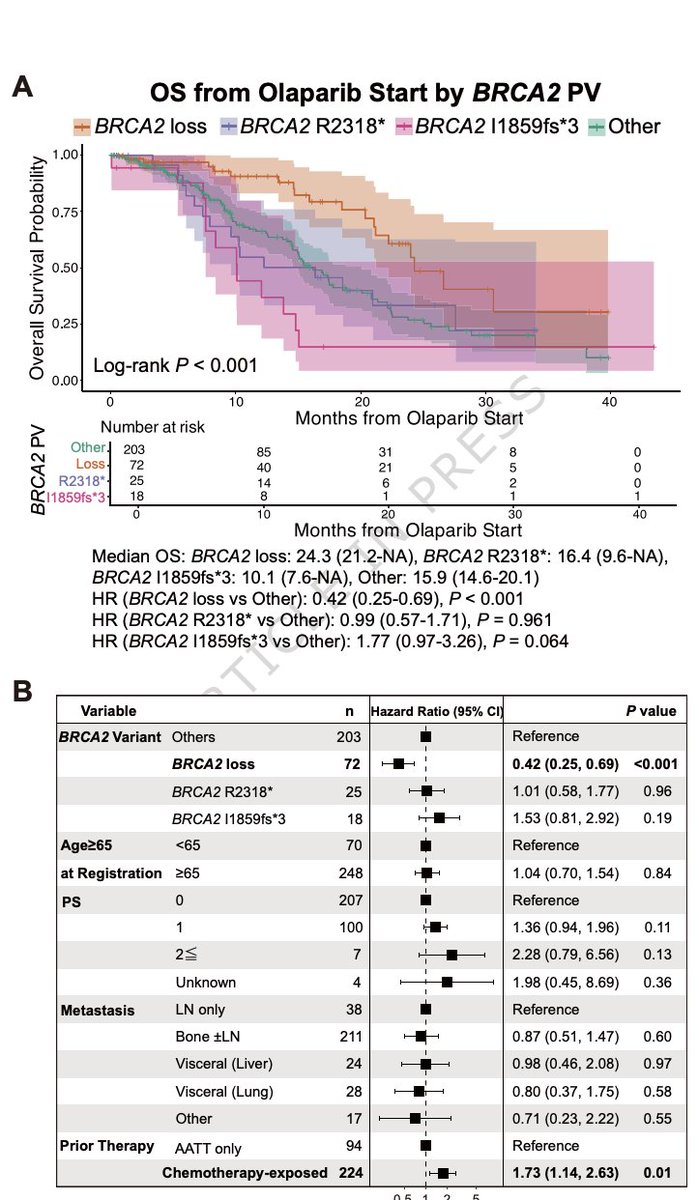
Retrospective real-world clinicogenomic study in @Nature
5893 pts with mCRPC
37% HRR pathogenic variants.
13% BRCA1/2.
389 received olaparib:
BRCA2: median OS 17.5 mo
BRCA1: 8.1 mo
HR 2.23 (P=0.008)
BRCA1 clearly worse.
Within BRCA2, subtype defines benefit ⚠️
BRCA2 loss: median OS 24.3 mo
HR 0.42 (P<0.001)
This is intra-BRCA functional heterogeneity ‼️
Not all BRCA alterations are biologically or therapeutically equivalent.
https://t.co/EVyVPFf7HN @OncoAlert
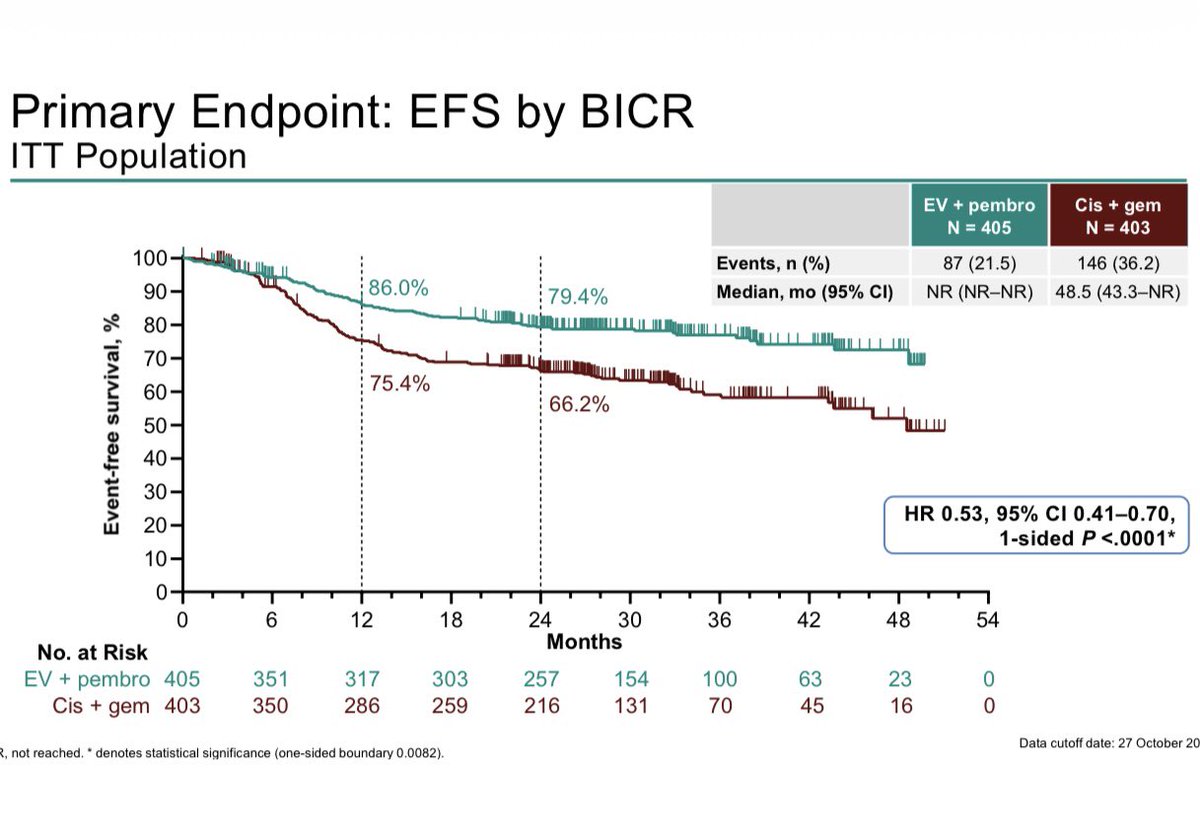
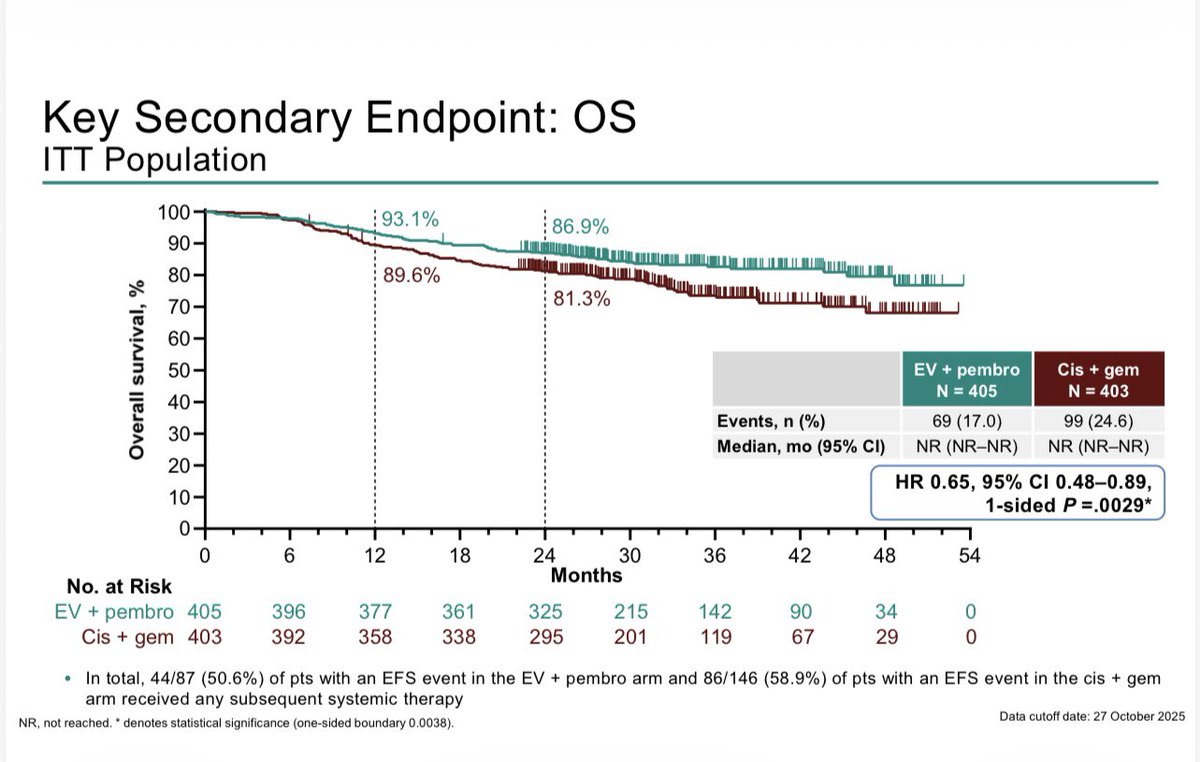
KN-B15/EV303: R3 Perioperative EVP vs Gem/cis in MIBC shows EFS HR 0.53 (0.41–0.70), OS HR 0.65 (0.48-0.89), pCR 56% vs 33%, G3+ tox 76% vs 67% #GU26. About half the patients completed 9 cycles of EVP. These are great results. Gem/cid is harder to beat when not all patients are at risk of relapse. Bladder sparing approaches for cCR (~60%) will be where this ends. ‘EVP 1st, ask questions later’. These studies are needed soon.
Rezatapopt: p53 reactivator!
A target we’ve talked about for years — once thought impossible.
TP53 Y220C may define a small patient subset,
but it proves a big point:
mutant p53 can be restored.
A paradigm-shifting proof!
https://t.co/m91o14ZPHG
📄Nueva publicación internacional liderada por Javier Martin-Broto con los primeros resultados del registro SELNET(SAR-TRACK)
🔍Analiza la calidad del manejo del sarcoma en Iberoamérica y la necesidad de atención multidisciplinar y centros de referencia
🔗 https://t.co/9OO9Q3f4O1
CUP is 2–5% of cancers but causes the 4th most cancer deaths. ⚠️
While tissue of origin can guide treatment, most patients see no clear benefit. ~33% have actionable mutations, targeted therapy won’t help all, but for some, it could change everything.
https://t.co/F1vwqBiz6B
🆕 FDA grants accelerated approval to Dato-DXd for EGFR-mutated NSCLC post-TKI + chemo 👏
But what’s the full picture? 🤔🧵
🔹 Based on 117 pts pooled from TROPION-Lung01 & Lung05
🔹 ORR: 43% | PFS: 5.8 mo | OS: 15.6 mo 📊
🔹 Prior osimertinib in 82% of pts
🔹 Common tox:
Stomatitis (69% any grade) 👄
Ocular events (32%) 👁️
ILD (4%) ☁️
✅ Signal of activity in a high-need population
⚠️ But:
No control arm
No stratification by TROP2 or EGFR mutation subtype
Limited CNS data 🧠
Accelerated based on surrogate endpoints (ORR/DOR)
📌 Dato-DXd brings hope, but confirmatory data is essential.
A step forward—but we must walk with scientific caution 👣
#LungCancer #EGFR #NSCLC #OncoTwitter #ADC @OncoAlert@brunolarvol