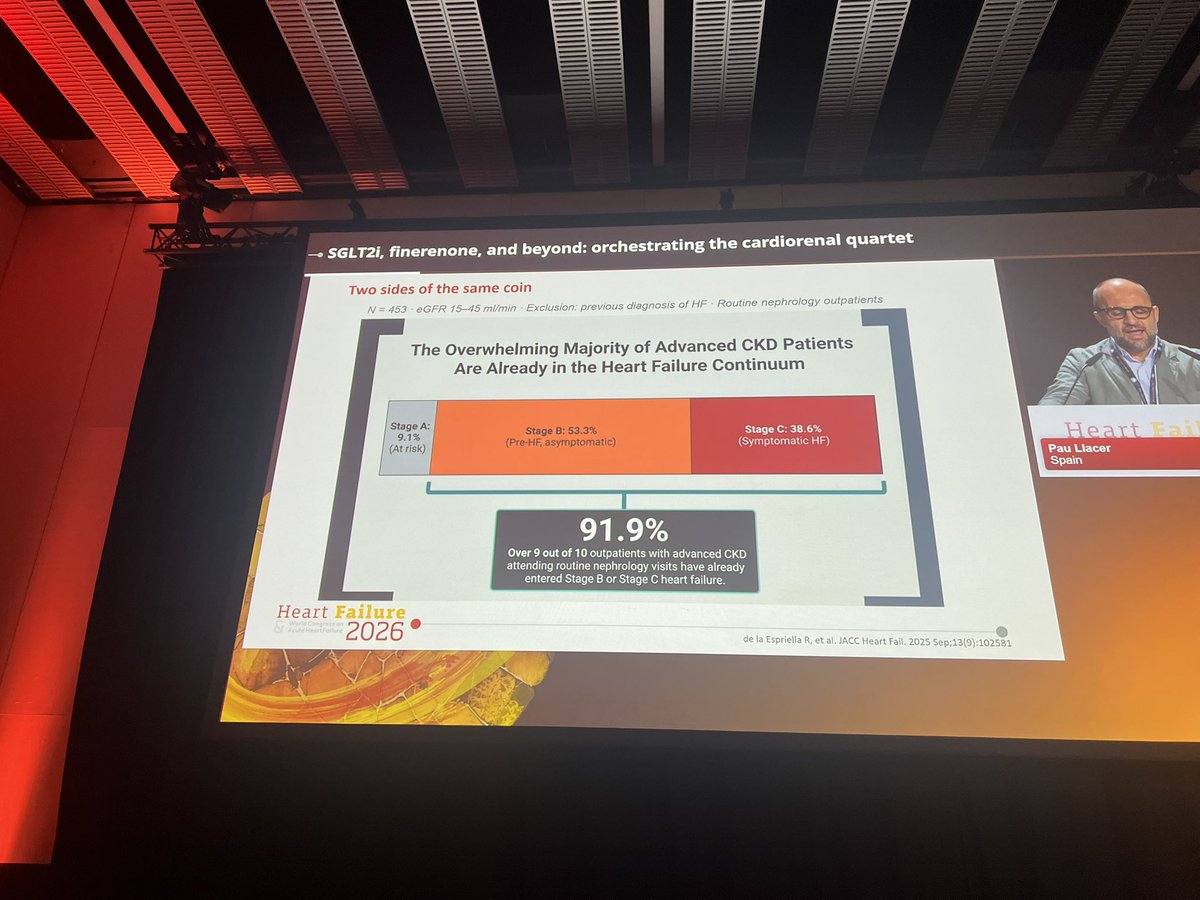
🤯 A striking stat from Pau Llacer at #HeartFailure26
91.9% of advanced CKD patients (eGFR 15-45) attending routine nephrology visits have already entered the heart failure continuum.
Breakdown in 453 outpatients with NO prior HF diagnosis:
• Stage A (at risk): 9.1%
• Stage B (pre-HF, asymptomatic): 53.3%
• Stage C (symptomatic HF): 38.6%
Over 9 in 10. Routine nephrology visits. No known HF.
The cardiorenal overlap isn’t a niche — it’s the rule.
Nephrologists ARE heart failure doctors whether they know it or not. Time to act like it. 🪲❤️
(de la Espriella R et al. JACC Heart Fail. 2025 Sep;13(9):102581)
#CardioTwitter #HeartFailure #Nephrology #CardiorenalSyndrome #CKD
💊 Practical algorithm for diuretic resistance in acute HF from #HeartFailure26— this is the slide to save!
Start: Furosemide 120-160 mg
↓ Still congested?
Add Chlortalidone 12.5-50 mg/24h
↓ Still congested?
Tailor to the problem:
• Metabolic alkalosis → Acetazolamide 120-500 mg/24h
• Hyponatremia → Tolvaptan 15-50 mg/24h
• rLVEF + hypopotassemia → MRA 25-100 mg/24h
And running through the whole algorithm:
➕ Add iSGLT2 throughout
➕ Add sacubitril/valsartan if LVEF <49%
➕ Consider parenteral route if oral absorption is the issue
Clean. Practical. Evidence-based. 💯
(Adapted from de la Espriella R et al. Nefrologia 2021)
#CardioTwitter #HeartFailure #Cardiology #Diuretics #HFrEF
Evil websites like Libgen, Z-library, and Sci-Hub had pirated millions of academic books and papers.
They've been shut down, and rightly so.
We shouldn't use them anyway. We should make billion-dollar academic publishers richer.
Anyway, here's how to access these libraries:
🚨DO NOT DO THIS!
Seminario web GRATUITO de una hora, organizado por EchoNous, pionero en ecografía en el punto de atención (POCUS), dirigido a nefrólogos, médicos de urgencias y otras especialidades médicas. Incluido Dr. José de la Flor Merino (@josedelaflora), Dr. Salvador López Gil (@salvadorlgil), Dr. Eduardo Rios Argaiz (@ArgaizR), y Dr. Abel Torrelles Fortuny.
Expertos destacados explicarán cómo la tecnología POCUS más reciente permite evaluar con precisión el estado del volumen de fluidos y realizar una monitorización dinámica no invasiva en los pacientes.
—
FREE one-hour webinar (in Spanish), organized by EchoNous, aimed at nephrologists, emergency physicians, and other
medical specialties. Including Dr. José de la Flor Merino (@josedelaflora), Dr. Salvador López Gil (@salvadorlgil), Dr. Eduardo Rios Argaiz (@ArgaizR), and Dr. Abel Torrelles Fortuny.
Leading experts will explain how the latest POCUS technology enables the precise assessment of fluid volume status and the performance of non-invasive dynamic monitoring in patients.
Introducing Dr. Smith’s ECG Blog 2.0!
The world’s #1 ECG Blog now features:
- smarter search (try “HATW in aVL”)
- email newsletter for new posts
Join over 200,000 monthly readers on our brand-new custom domain!
🚨 𝗕𝗥𝗘𝗔𝗞𝗜𝗡𝗚 from #ACC2026: Two major RCTs just challenged everything we thought about Impella pumps in cardiac care.
The results? Surprising.
The implications? Massive.
A thread on what every cardiologist needs to know 🧵👇
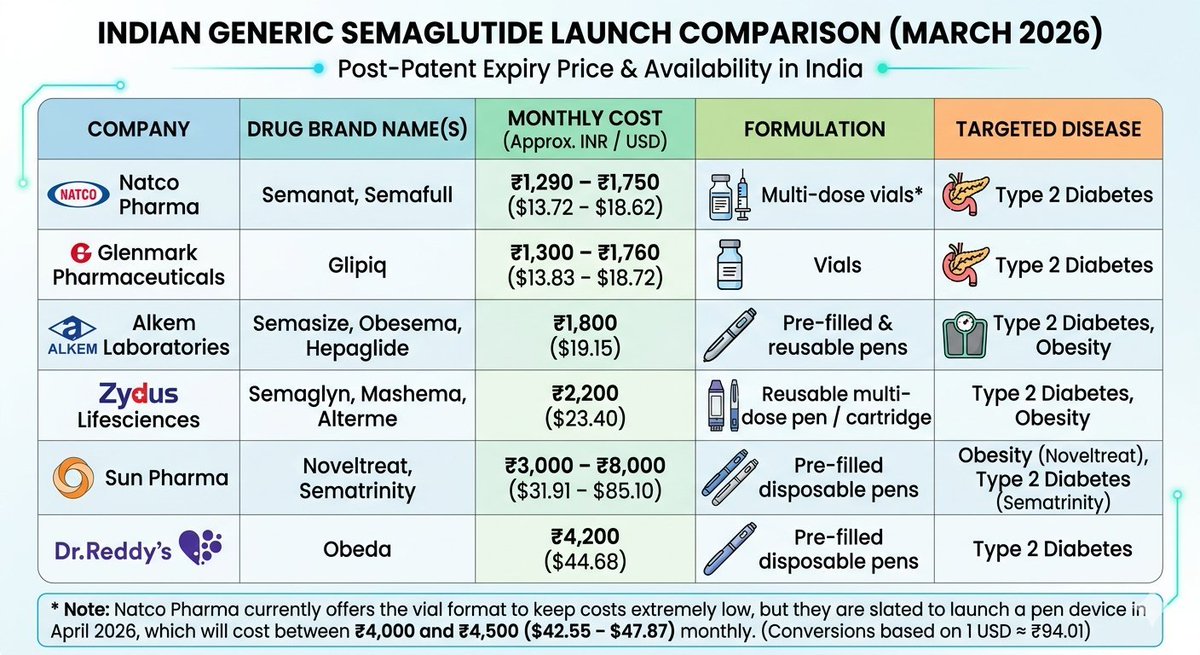
It's a momentous day for healthcare in India, China & Canada today.
With Novo Nordisk's patent for semaglutide officially expiring yesterday (March 20, 2026), several top Indian pharma companies have flooded the market today with generic versions, drastically slashing prices by 50% to 90% compared to innovator brands like Ozempic and Wegovy which traditionally cost between $95-$180 monthly.
Medio millón de pacientes han recibido un dispositivo Watchman en el mundo. El ensayo más riguroso realizado hasta la fecha acaba de cuestionar que sea la mejor opción para los que más parecían necesitarlo.
https://t.co/uGlj3VF43t
🫀 El CLOSURE-AF compara el cierre del apéndice auricular izquierdo frente al tratamiento médico optimizado en pacientes con FA de alto riesgo de ictus y sangrado.
📊 Resultado: el procedimiento no demostró no inferioridad, con 16,8 frente a 13,3 eventos por 100 pacientes-año en el endpoint compuesto.
⚠️ La tasa de complicaciones periprocedimiento fue del 5,7%, incluyendo taponamiento pericárdico y dos muertes en los primeros 7 días.
🔬 El debate está abierto: edad, fragilidad, dispositivos de nueva generación y seguimiento a largo plazo centran la discusión entre los expertos.
📖 Análisis completo con reacciones de la comunidad cardiológica internacional, en CardioTeca.
Recién salidas del horno, las Guías AHA 2026, de Dislipidemia. Algunos cambios importantes:
🟢Se eliminan las calculadoras de cohortes, y ahora se prefiere PREVENT. Se reduce también el umbral para iniciar estatinas (algo agresivo a mi parecer): riesgo a 10 años de ≥3%
🟢 Adiós a Friedewald: para la estimación del LDL-C, las ecuaciones de Martin/Hopkins o Sampson/NIH son ahora la recomendación preferida.
🟢 El retorno de Metas absolutas. Muy alto riesgo: LDL <55 mg/dL. Prevención primaria (Riesgo alto ≥10%): LDL <70 mg/dL. Riesgo intermedio 5-<10%: LDL <100 mg/dL
🟢 Se indica medir Lp(a) al menos una vez en la vida en todos. +50 mg/dL aumentan el riesgo cardiovascular relativo en aproximadamente un 40%
🟢Se instaura el modelo CPR (Calculate, Personalize, Reclassify). Si después hay incertidumbre, Score de Calcio (Reclassify) es el desempate. CAC = 0: sin estatinas.
Voy a revisarlas a fondo para actualizar las apps (https://t.co/O3HpYX0dAx).
Pueden bajar el PDF en el canal (https://t.co/3O93s10lns).
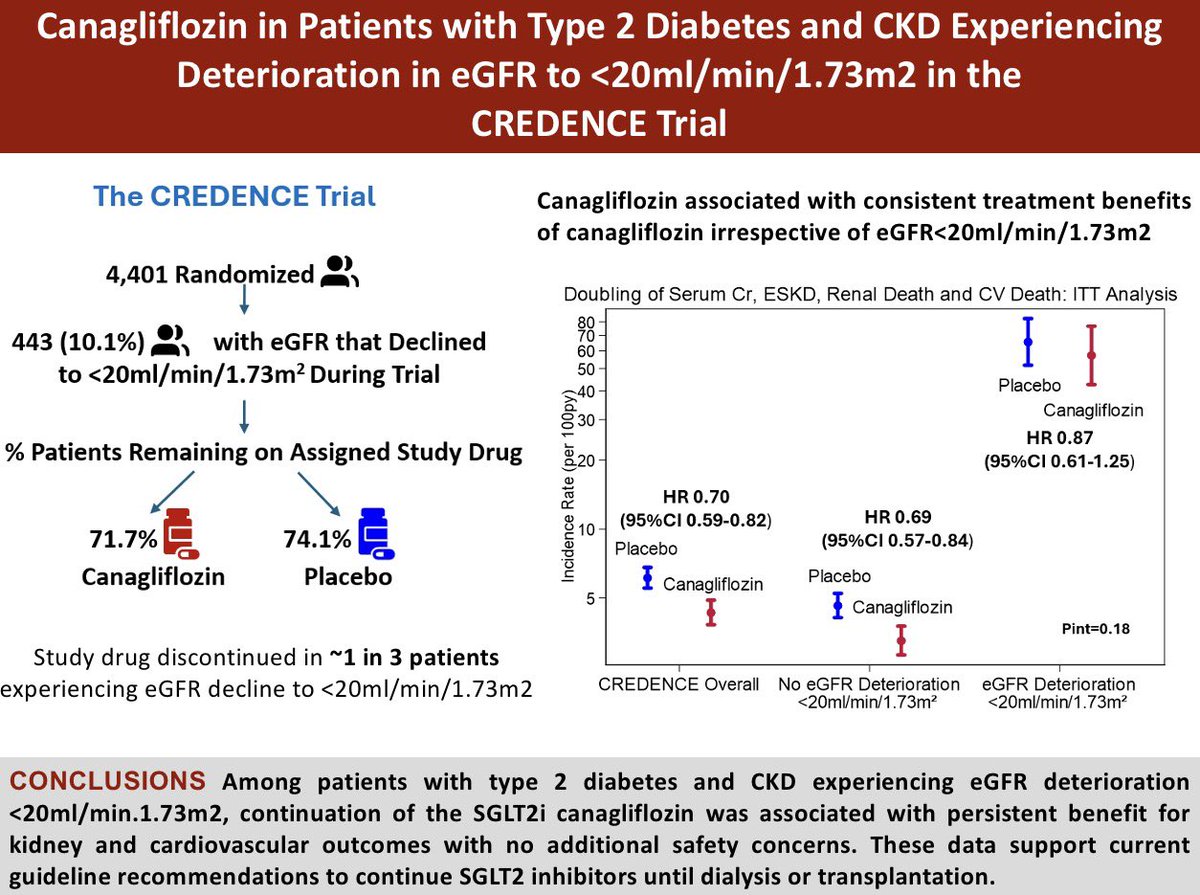
Don’t stop SGLT2i when GFR falls below 20ml/min - continue until dialysis/transplantation
New analysis from CREDENCE led by @safchat in @JCardFail
https://t.co/zVCzjkFj4j
new AHA/ACC guidelines on pulmonary embolism:
similiar to the Surviving Sepsis guidelines
- overall mediocre
- make some nice points
- most folks will accept them because they’re backed by so many societies
- will cause confusion & delay progress
(blog incoming soon)
Con diabetes, iniciar iSGLT2, comparado a aGLP1 durante 5 años; ↓19% el riesgo de evento renal mayor y ↓12% el de lesión renal aguda
Una vez más, se demuestra que iSGLT2 son lo mejor
En emulación de ensayo clínico
JAMA Intern Med 2026
10.1001/jamainternmed.2025.7409
🫀🧠 HFpEF is not just “diastolic dysfunction”: the microcirculation is the missing link
This 2025 JACC: Advances state-of-the-art review reframes heart failure with preserved ejection fraction (HFpEF)through a crucial, often underrecognized lens: coronary microvascular dysfunction (CMD) .
📊 How common is CMD in HFpEF? Very.
Up to 75% of HFpEF patients—even without obstructive coronary disease—have CMD. And this is not an innocent bystander:
CMD is independently associated with higher HF hospitalizations
Increased mortality and MACE
Worse quality of life
Yet, CMD is rarely sought and even more rarely diagnosed in routine HFpEF care.
🧠 Why CMD matters pathophysiologically
CMD disrupts the heart at multiple levels:
🔻 Reduced coronary flow reserve (CFR) → subendocardial ischemia
🔥 Microinfarctions & fibrosis → stiff myocardium
⚙️ Impaired cardiac–coronary coupling → blunted flow during stress
🧬 Inflammation & endothelial dysfunction → vicious cycle of ischemia and diastolic failure
HFpEF and CMD reinforce each other in a bidirectional loop, rather than a simple cause–effect relationship.
👩⚕️ A sex-specific disease
Women are disproportionately affected:
Higher CMD prevalence
Smaller coronary vessels, higher resting flow
Postmenopausal estrogen loss → inflammation, fibrosis, reduced CFR
This helps explain why HFpEF is more common and more complex in women.
🧪 Diagnosis: we’re under-testing
CMD can be assessed by:
PET or CMR perfusion
Invasive coronary functional testing (CFR, IMR, acetylcholine)
But there is no standardized diagnostic pathway in HFpEF—yet.
💊 Therapy: signals, not solutions
Some treatments show promise (SGLT2i, statins, RAAS modulation, lifestyle, GLP-1/GIP agonists), but no therapy specifically targets CMD in HFpEF so far.
🔮 Bottom line
HFpEF is not only a myocardial disease—it’s a microvascular disease.
If we keep ignoring CMD, we will keep failing HFpEF patients.
👉 Understanding and treating HFpEF may finally require looking beyond the ventricle—into the microcirculation.