📌 A randomized, open-label, phase 3 study of gedatolisib + fulvestrant +/- palbociclib vs standard of care in
HR+/HER2-|PIK3CA-mutant advanced breast cancer (VIKTORIA-1 Study 2).
Sara A. Hurvitz, MD, FACP 🎙️✨ #ASCO26@OncoAlert#OncoAlertAF
When @AACR and @ASCO collide and you are reunited with your scientist <-> survivor bestie in Chicago! 🫶 It might sound silly, but when you see someone you mentored thriving it just makes my heart happy! Keep up the amazing work @DonjetaZeqa#ASCO26
PANKU-Breast02:
Izalontamab Brengitecan Redefines Outcomes in Pretreated mTNBC
PANKU-Breast02 demonstrates significant dual PFS/OS benefit, with a 40% reduction in mortality risk and a median OS gain of 3.4 months versus chemotherapy
@OncoAlert#ASCO26#BreastCancer#bcsm
Dr. Tina Cascone outlines rationale & science behind neoadjuvant and perioperative immunotherapy for early stage NSCLC at #ASCO26. How do we isolate the value of the adjuvant component after pCR or non-pCR? How do we best escalate non-pCR? ADC? Vaccine? Insightful discussion.
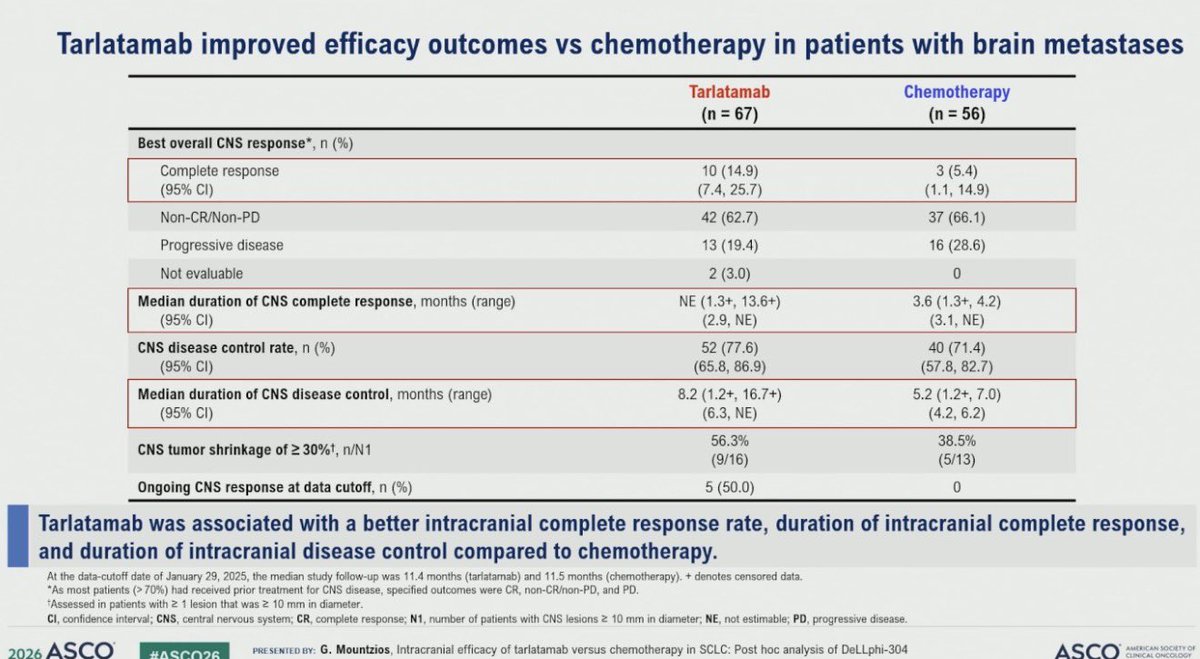
Dr. @g_mountzios#ASCO26 presents CNS outcomes with 2L tarlatamab in DeLLphi-304. Improved time to CNS progression overall (HR 0.54). In pts with brain nets, tarlatamab vs chemo CNS CR rate 15% vs 5% with DCR 78% vs 71% and time to CBS progression 6.5m vs 4.2m, HR 0.40
Dr. @LuisPaz_Ares: biomarkers from phase III IMforte trial of maintenance lurbinectedin in SCLC #ASCO26. PFS & OS benefit of maintenance lurbinectedin seen across molecular subtypes and independent of SLFN11 expression. Suggestion that lurbi may overcome TAM-mediated resistance.
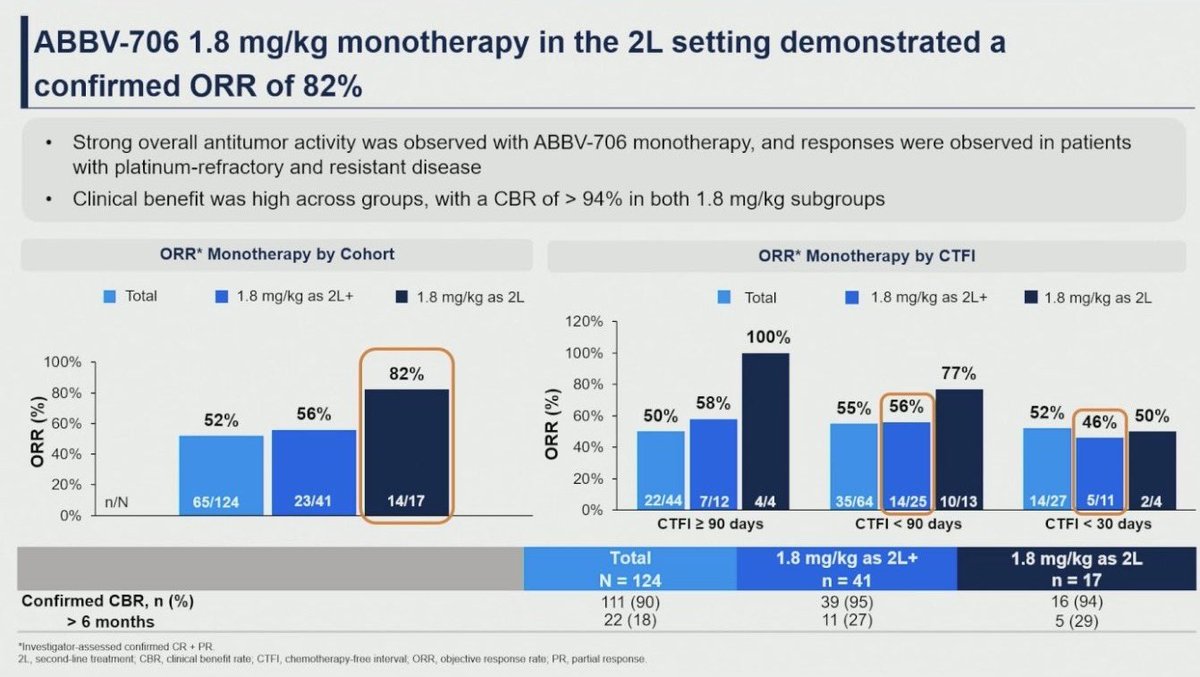
#SCLC Update 🚨
(First-in-Human ABBV-706):🫁 SEZ6-targeted ADC delivers a striking signal in R/R disease with ORR 82% in 2L and deep disease control even in chemotherapy-refractory cohorts (CTFI <30d), with early OS trend 14.3 mo—redefining the ADC landscape in SCLC.
@OncoAlert
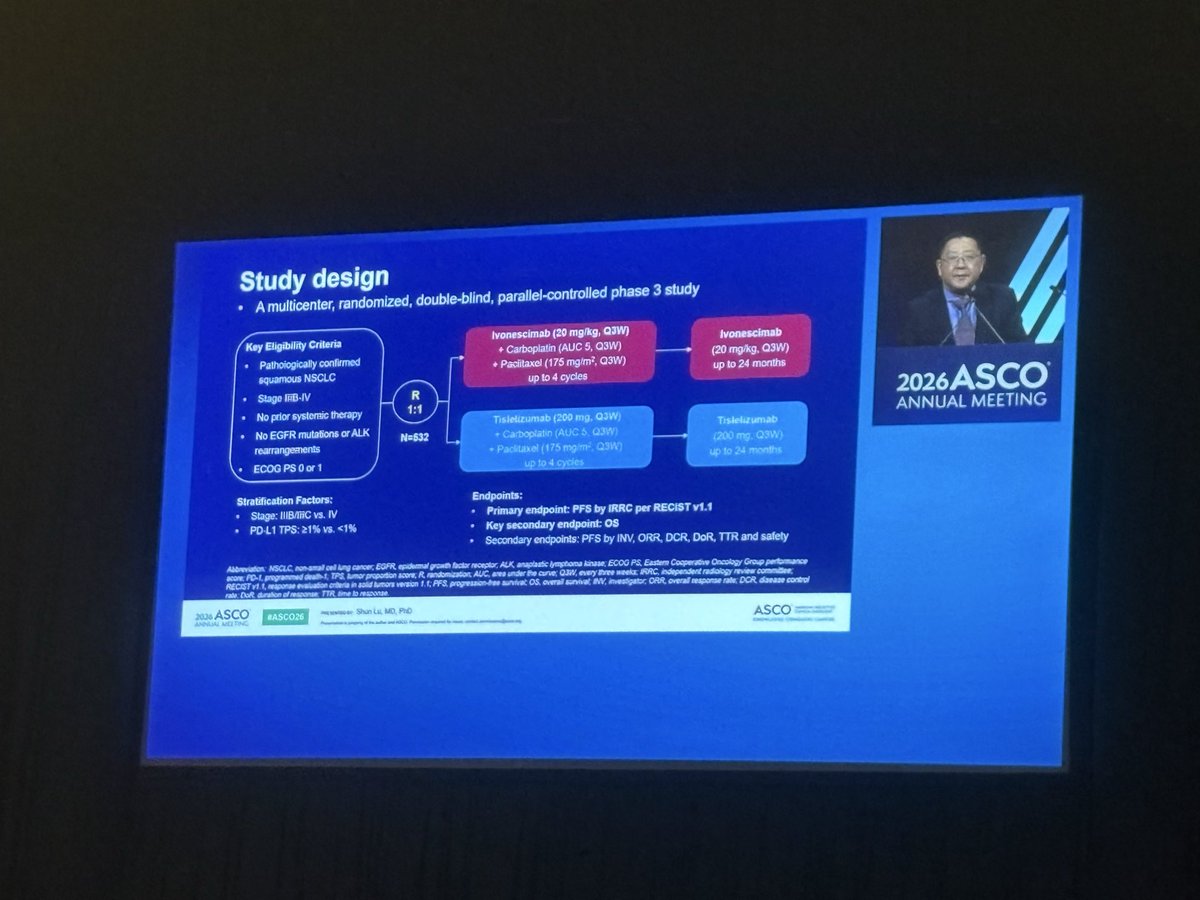
One of the most awaited presentations( at least by me) #ASCO26:
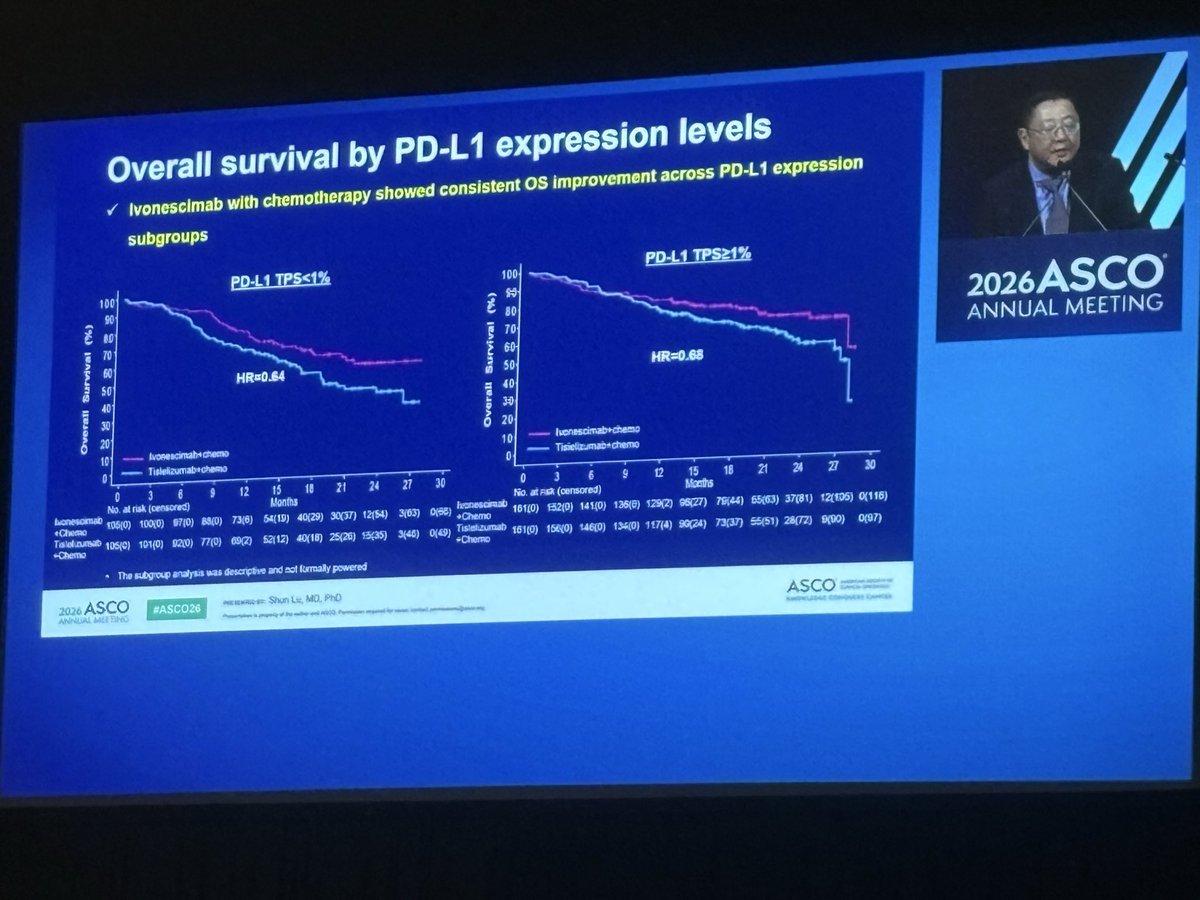
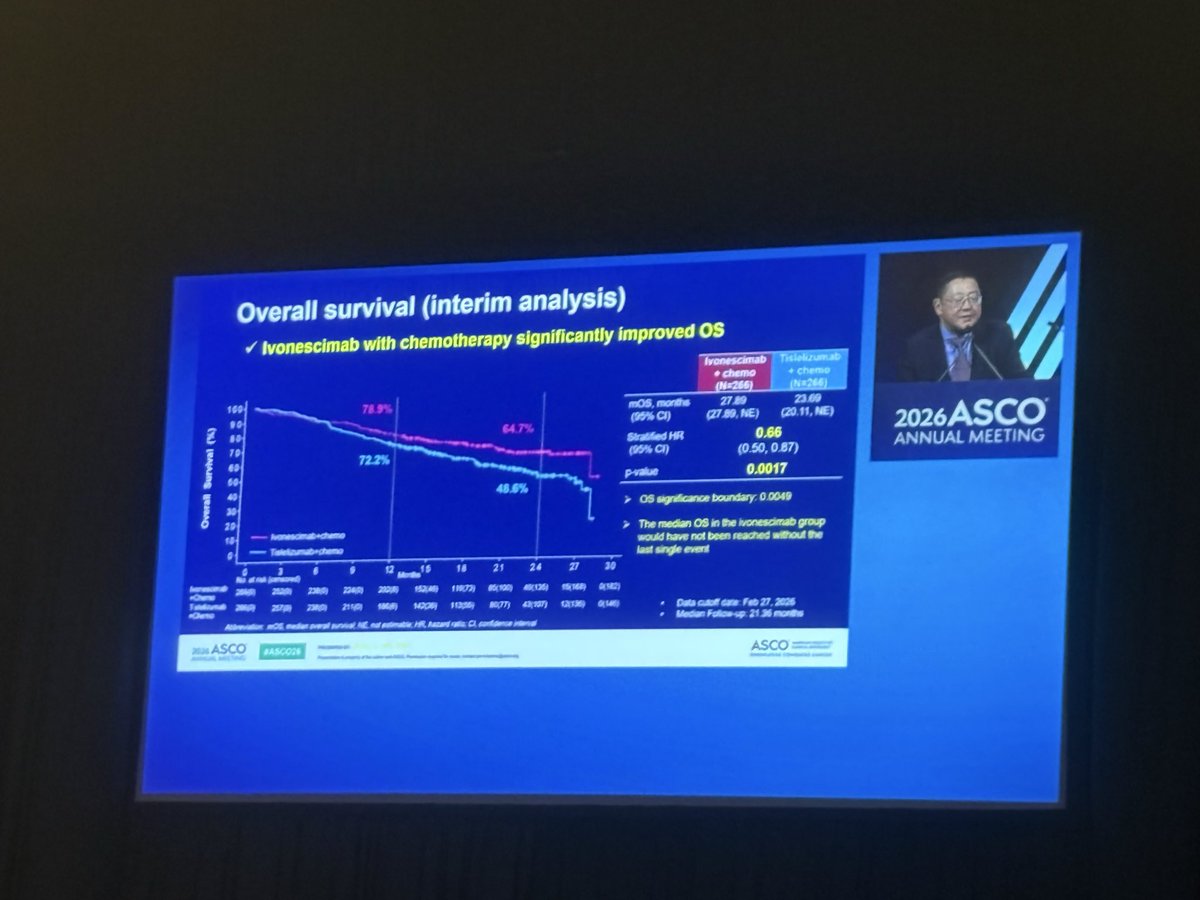
HARMONi-6 shows that ivonescimab + chemo significantly improves OS
Vs tislelizumab + chemo in first-line advanced Sq #NSCLC (HR 0.66).
A positive phase III study with a clinically meaningful OS benefit and simultaneous publication in @TheLancet:
https://t.co/2JR3fy4cL1
Caveat: this was a study conducted entirely in China. How these data will translate globally remains an important question? Let’s see what HARMONI 3 will show
Dr. Zhao PhII study of ZG006 (tri-specific T-cell engager DLL3/CD3) in refractory #NEC (1 prior line) ➡️ ORR 57.3%, median DoR 11.76 mos, median PFS 7.06 mos, median OS NR in 30 mg cohort if DLL3 tumor cell staining >50%, 68.8% G>3 TRAEs, no G5 events in 30 mg
#ASCO26@OncoAlert
Dr. Oh Asian-based PhIII ATTRACTION-6 trial of platinum-chemo +/- nivo/ipi (1 mg/kg Q6W) in #1L HER2- met GC/GEJC (55% CPS<5) ➡️ no sig diff in median OS 15.7 vs 15.8 mos or PFS 8.9 vs 7.7 mos in ITT, 3 mo OS ⬆️ in CPS>5 & ORR 57.9 vs 38.5% in favor of chemoIO
#ASCO26@OncoAlert
NeoINR:
Simultaneous CTLA-4, PD-1, and LAG-3 Blockade Achieves Remarkable Pathologic Responses in Resectable Advanced Melanoma, Setting the Stage for a New Neoadjuvant Immunotherapy Paradigm.
@OncoAlert#ASCO26
#ASCO26
This one is special.
This is the hottest paper of 2026 and potentially in the history of pancreatic cancer.
Let’s dive in.
RASolute 302: Daraxonrasib vs investigator’s choice chemotherapy in previously treated metastatic pancreatic cancer
Abstract LBA5 (soon!)
Presentation: May 31, 2026, 3:21-3:33 PM CDT
For decades, pancreatic cancer has been where good ideas go to die.
We have optimized chemotherapy. We have sequenced chemotherapy. We have celebrated modest gains.
But the central driver of PDAC has always been sitting there in plain sight:
RAS.
More than 90% of pancreatic cancers have oncogenic RAS mutations, and until recently, we had essentially nothing direct to do about it.
Daraxonrasib is an oral RAS(ON) multiselective inhibitor targeting the active GTP-bound state of mutant and wild-type RAS.
And in RASolute 302, it delivered.
Quick hits:
📌 Phase 3 international randomized trial 500 patients with previously treated mPDAC Daraxonrasib vs investigator’s choice chemotherapy
🧬 RAS G12 population
91.8% of patients had RAS G12 mutations
📈 OS in RAS G12 population
13.2 vs 6.6 months
HR 0.40
P<0.001
📈 OS in overall population
13.2 vs 6.7 months
HR 0.40
P<0.001
📊 PFS in RAS G12 population
7.3 vs 3.5 months
HR 0.45
P<0.001
📊 PFS in overall population
7.2 vs 3.6 months
HR 0.49
P<0.001
🔥 12-month OS
Overall population: 53.2% vs 17.3%
⚠️ Toxicity matters, but this was not just more efficacy for more toxicity
Grade ≥3 AEs: 61.8% vs 69.6%
TRAEs leading to discontinuation: 1.2% vs 11.2%
This is the kind of survival curve we almost never get to see in pancreatic cancer.
This validates RAS(ON) inhibition in the most RAS-addicted major cancer. It takes a target we have talked about for decades and turns it into a clinically meaningful survival benefit in a randomized phase 3 trial.
The next questions come fast: 1L combinations, maintenance, perioperative disease, sequencing, resistance, toxicity management, and whether this becomes a new backbone.
RAS is here, and it couldn’t have come sooner.
https://t.co/Y4WJRlRRTk
@TheGutonclab@UGrewalMD@TimothyJBrownMD@OncoAlert@Onco_Nexus@ASCO@NazliDizman@LauraAlderMD@DVAraujoMD@DrBarbiOnc@LauraEsfeller@FunchainMD@YGaritaonaindia@DrSAHaddad@jgong15@iandresmeraz@SakditadMD@RamilaShilpakar@RohitBanwar@lungoncdoc
#ASCO26 Watched On Demand "Elevating the Patient Voice..." Thanks @stage4kelly for being our voice!
Yes, advocates are @ASCO members. We are ready to be involved.Yes, PROs should be included in every trial. Yes, QOL measures should be co-primary end pts. #gyncsm
Published today and presenting tomorrow! 📚➡️🎤
Excited to share our @ASCO Ed Book chapter on the contemporary challenges of EOC care @KimmieNgMD@drtarahenderson#IreneSu
Looking forward to tomorrow’s discussion at #ASCO26
https://t.co/geEMt1uKhR
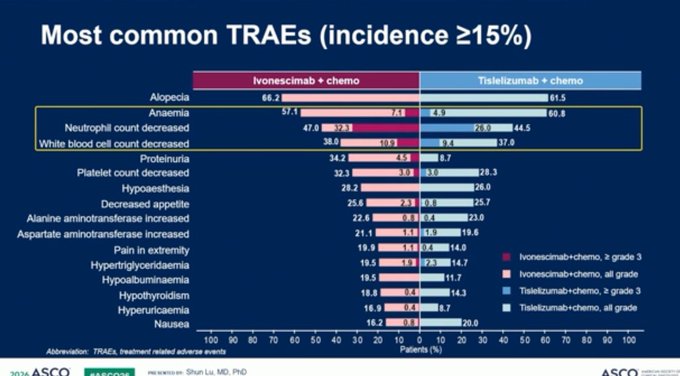
#ASCO26 Safety shows d/c rate of ivonescimab and tislelizumab were low (5%) adn G3+ irAEs 14% in both arms. Main higher grade AEs were hematologic in nature. Global phase III study, HARMONi-3, is underway. Important positive study but global data needed to change US practice.
Novel endocrine therapies are transforming outcomes for our patients — first in the second-line setting, and now with innovative ctDNA based strategies and, most importantly, in the curative setting. A pleasure to join this @gotoPER symposium to review this evolving landscape.