🆕🔥EMPHASIS RCT
A multicentre, double-blind, RCT
N:1724
Minocycline therapy initiated within 72 h of acute ischaemic stroke provided a significant functional outcome benefit compared with placebo at 90 days, without safety concerns #IDXposts
https://t.co/tPHJp4tHKW
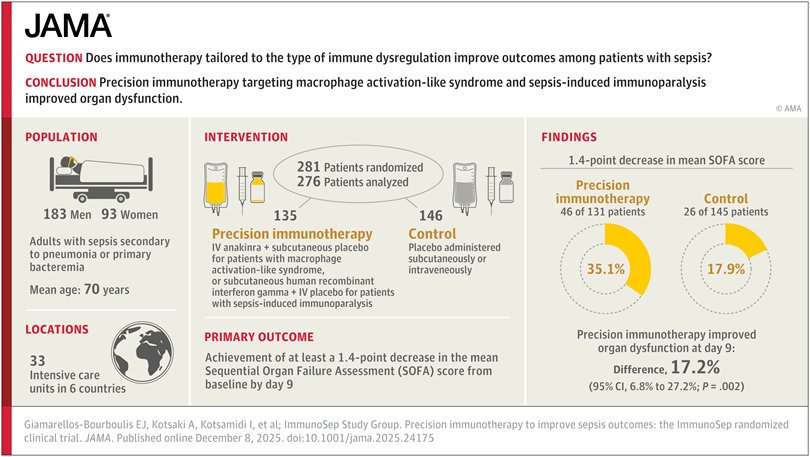
🆕⚡🧬🧩 The Sepsis Puzzle: Precision Immunotherapy Finds a Missing Piece | ImmunoSep RCT | JAMA, 2025
🚀 What they did
• 🧪 RCT (double-blind, double-dummy, placebo-controlled) across 🌍 6 countries
• 👥 276 adults with Sepsis-3 + immune dysregulation
• 🔍 Stratified by immune phenotype:
• 🔥 MALS (ferritin >4420) → 💉 IV anakinra
• 💤 Immunoparalysis (low HLA-DR) → 💉 IFN-γ
• 🏥 Standard care ➕ precision immunotherapy vs standard care ➕ placebo
• 🎯 Primary endpoint: SOFA ↓ ≥1.4 points by day 9
🔥 Key findings
• 📉 Organ dysfunction improved by day 9: 35.1% vs 17.9% (+17.2% over placebo)
• ⚰️ 28-day mortality: ❌ no significant difference
• ⚠️ AEs common:
• 🩸 More anemia with anakinra
• 💉 More bleeding with IFN-γ
• 🧬 Matching therapy to immunotype = driver of benefit
⚠️ Limitations
• ⏳ Benefit measured only to day 9
• ❌ No mortality signal
• 🧫 Requires ferritin & HLA-DR → not widely available
• 💉 High AE burden
💡 Takeaway
Precision immunotherapy (anakinra for MALS, IFN-γ for immunoparalysis) delivers an early organ-function boost, but without a mortality benefit and with notable safety risks.
A promising step toward personalized sepsis care—not practice-changing yet. #IDXposts
https://t.co/wMSNPeHgqa
🆕⚡💊 A SNAP Moment — Flucloxacillin Variability Raises a Wake-Up Call to Shift Toward Safer MSSA Options(FLUTE study) |JAC 2025
🚀 What they did
🔬 Retrospective study of 203 hospitalized patients receiving flucloxacillin.
🧪 Measured unbound flucloxacillin ≥48h after starting therapy and compared levels with PK/PD targets (4–10× MIC).
🩺 Assessed links between high unbound levels and nephrotoxicity 🧨 & neurotoxicity ⚡.
👀 Identified patient groups who may benefit most from TDM.
🔥 Key findings
🎯 Only 33% reached target levels.
🟦 35% were too low → underdosing.
🟥 32% were too high → toxicity risk.
⚠️ Toxicity thresholds:
🚨 Nephrotoxicity ≥10 mg/L (66.7% affected).
⚡ Neurotoxicity ≥21 mg/L (46.2% affected).
🧓💧 Most high-level patients had eGFR <50 mL/min, showing classic accumulation.
⚠️ Limitations
🏥 Single center.
📚 Retrospective design.
🔍 Timing of level collection not fully standardized.
💡 Takeaway
Renal impairment + high daily flucloxacillin doses = strong candidates for TDM to prevent AKI and neurotoxicity. With only one-third of patients achieving target levels, this SNAP moment highlights growing evidence pushing us toward safer MSSA options (cefazolin, cephalexin, cefadroxil) where appropriate.
#IDXposts #IEWiki
https://t.co/uPrQKCDfig
🆕⚡🦠 Aztreonam-Avibactam — The Undisputed Hero 🏆 Tackling MBLs Like a Pro| AAC/2025
🐯 Tigecycline — “The Tiger,” still strong and reliable but not in BSI.
🐴 Cefiderocol — Once the Trojan Horse, but not the soldier we hoped for
🎯 Cefepime-Taniborbactam — Targets MBLs, yet resistance strikes with tricky combos (NDM-9, IMP-8, CTX-M-15, porin changes…)
🚀 What they did
🔬 Tested aztreonam-avibactam, cefiderocol, cefepime-taniborbactam, tigecycline, and colistin against 490 genetically characterized MBL-producing Enterobacterales from 27 countries (2019–2022).
🧬 Characterized MBL types: NDM-1 (307), NDM-5 (68), VIM-1 (53), and 14 other genes/combinations (62).
🌍 Looked at susceptibility patterns and resistance mechanisms, including other β-lactamases, porin changes, and efflux pump disruptions.
🔥 Key findings
✅ Aztreonam-avibactam: 100% susceptible (MIC50/90 0.12/0.5 mg/L) — unstoppable hero!
🐯 Tigecycline: 94.1% susceptible — reliable as ever.
🐴 Cefiderocol: 66.7–90.8% susceptible — the Trojan Horse isn’t always victorious.
🎯 Cefepime-Taniborbactam: 36.7–55.5% susceptible — resistance hits tricky combos (NDM-9, IMP-8, CTX-M-15, porin changes…).
⚠️ Colistin: 76.6% susceptible — last-resort back-up.
⚠️ Limitations
🏥 Single study with 490 isolates; global trends may vary.
🔍 Some rare MBL types may respond differently.
💡 Takeaway
Aztreonam-avibactam reigns supreme against MBLs — the undisputed hero in a sea of tricky resistance. Other options like tigecycline remain solid, but cefiderocol and cefepime-taniborbactam show variable activity depending on resistance combos. This highlights the urgent need for tailored therapy guided by resistance mechanisms. #IDXposts
https://t.co/yA24PvUDWW
🚨 Francia confirma 2 casos importados de MERS-CoV en viajeros que regresaban del Oriente Medio.
🔗 Noticia: https://t.co/oe2hk3D9iZ
⸻
🦠 ¿Qué es el MERS-CoV?
• Coronavirus zoonótico identificado en 2012 en Arabia Saudí.
• Hospedador primario: dromedarios 🐪.
• Transmisión entre personas: limitada, pero posible en entornos sanitarios y contactos estrechos.
• Letalidad estimada: ~35%.
• Cuadro clínico: fiebre, tos, dificultad respiratoria; puede causar neumonía grave y fallo multiorgánico.
⸻
🇫🇷 Sobre los casos en Francia
• Ambos viajaban en el mismo grupo turístico.
• Detectados tras aparición de síntomas; ya están hospitalizados y aislados.
• Estado clínico: estable.
• Activado el rastreo de contactos y vigilancia de viajeros procedentes de la región.
⸻
🔍 Puntos clave para la salud pública
• El riesgo global es bajo, pero no inexistente.
• Importancia de la detección precoz en viajeros con síntomas respiratorios tras volver de países del Golfo.
• Medidas básicas recomendadas:
– higiene de manos,
– usar mascarilla si hay síntomas,
– consultar ante fiebre + tos + antecedente de viaje reciente.
• Para profesionales: mantener sospecha clínica y aplicar precauciones de contacto y gotas / aerosol según procedimientos.
⸻
🌍 Seguimos monitorizando la situación desde GEPI-SEIMC.
La vigilancia internacional y la comunicación transparente son fundamentales para anticipar riesgos emergentes.
Guías #PrEP👉🏻screening ITS 3-6 meses pero datos sobre esto #escasos.En @Lancetmicrobe en 🇧🇪solo test a SINTOMATICOS
1️⃣Incidencia #Ngonorrhoeae y #Ctrachomatis disminuyó🧫📉
2️⃣No aumento infecciones sintomáticas❌
3️⃣Dismimuyó uso de antimicrobianos📉💊
🔗🆓https://t.co/58SiIOPje5
🆕🔥 🫁🧯 Steroids Save Lives — Low-Dose Corticosteroids Cut Short-Term Mortality in Severe Pneumonia & ARDS, Annals of Internal Medicine, 2025
🚀 What they did
🔎 Systematic review + meta-analysis (20 RCTs( 15 severe pneumonia), 3459 adults) across severe non-COVID pneumonia & ARDS
📚 Compared systemic corticosteroids vs placebo/usual care
💊 Focused on low-dose (<3 mg/kg/day prednisone-equivalent), ≤15 days, started within 7 days
🧪 Outcomes: short-term mortality, shock, hospital-acquired infections, secondary pneumonia, bloodstream/catheter infections
🔥 Key findings
💀 Short-term mortality ↓
• Severe pneumonia: RR 0.73 (95% CI 0.57–0.93)
• ARDS: RR 0.77 (95% CI 0.61–0.99)
🫀 Secondary shock ↓ in severe pneumonia
• RR 0.49 (95% CI 0.26–0.92)
🛡️ No increased risk of hospital-acquired infections
• Severe pneumonia: RR 0.99
• ARDS: RR 0.97
🦠 Little to no difference in secondary pneumonia across both groups
🩸 Evidence for catheter-related & bloodstream infections = very uncertain
⏳ Long-term mortality = very uncertain
⚠️ Limitations
📉 Heterogeneous pneumonia severity definitions across trials
🧪 Variable reporting of infection-related complications
🌍 Mixture of ARDS & pneumonia studies may limit subgroup precision
💡 Takeaway
👉 Low-dose, short-course systemic steroids probably reduce short-term mortality in both severe pneumonia and ARDS — without increasing hospital-acquired infections.
🔄 Supports early, controlled steroid use in selected critically ill adults.
🛡️ Benefit strongest for mortality & shock reduction; infection risks appear minimal at low doses. #IDXposts
https://t.co/ppaRy7lapP
🆕⚡🦀A New Twist — Once Again, Ceftazidime Avibactam Turbocharges Ampicillin Sulbactam Against CRAB | JAC-AMR 2025
🚀 What they did
🧪 In-vitro study of 184 CRAB isolates from 9 Peruvian hospitals (2018–2023).
🧬 Confirmed via blaOXA-51 PCR, MALDI-TOF, and 16S rRNA where needed.
💊 Tested ampicillin/sulbactam (SAM) + ceftazidime/avibactam (CZA) synergy using dual-disc diffusion (20 mm → 10 mm).
🧲 Screened for MBL using EDTA synergy; confirmed blaNDM by PCR.
📊 Compared synergy across susceptible / intermediate / resistant CRAB categories.
🔎 Stats via Fisher’s exact test.
🔥 Key findings
🧱 87.5% of isolates were AMP/SUL-resistant.
💥 97.3% overall synergy with SAM + CZA (97.2% in non-susceptible).
🧬 MBL (blaNDM) in 1.6% — poor/absent synergy (expected: avibactam doesn’t inhibit MBLs).
⚙️ One NDM isolate showed synergy at 10 mm → likely low MBL expression + serine β-lactamase inhibition.
🚫 Three non-NDM isolates lacked synergy → likely porin loss, efflux, or OXA-variants not inhibited by avibactam.
⚠️ Limitations
🔬 No MIC confirmation (no avibactam powder).
🧭 Possible MALDI-TOF misidentification in a minority.
🌍 All isolates were carbapenem-resistant → limits generalizability.
📦 Non-parallel isolate recovery → no evolutionary analysis.
💡 Takeaway
👉 Sulbactam/avibactam shows potent in-vitro synergy with CZA against CRAB, restoring activity even in resistant isolates.
🛡️ Especially useful in regions with CRAB prevalence >80% where options are scarce.
⛔ Limited activity against NDM producers — inherent class limitation.
📈 Supports future stewardship pathways for XDR CRAB, while clinical trials are urgently needed.
Could this become a salvage option for SAM non-susceptible CRAB isolates? #IDXposts
https://t.co/IUaUsTNAtw
Infections don’t follow the tidy stories we tell ourselves.
They follow biology, behavior, chance, and sometimes undercooked chicken.
A few common myths in ID worth exploring in more detail. (Link in next tweet 👇)