The new ERC 2025 recommendations for advanced airway management during CPR
Airway and ventilation
📌During CPR, start with basic airway techniques and progress stepwise according to the skills of the rescuer until effective ventilation is achieved.
📌Give the highest feasible inspired oxygen during CPR.
Start effective ventilation breaths as soon as possible ensuring the rate and tidal volume are appropriate to prevent both inadequate ventilation (hypoventilation) and excessive ventilation (hyperventilation).
📌Deliver effective bag-mask ventilation breaths by optimising mask seal and airway patency and if necessary, use a two-person technique for bag-mask ventilation.
📌Give each inspiratory breath over 1s to achieve a visible chest movement.
📌When using a supraglottic airway (SGA), an i-gel is preferred to a laryngeal tube.
📌Tracheal intubation should only be attempted by rescuers with a high success rate and with the use of continuous waveform capnography. The expert consensus is that a high tracheal intubation success rate is over 95 % within two attempts at intubation.
📌Aim for less than a 5-second interruption in chest compression for tracheal intubation.
📌Use direct or video laryngoscopy for tracheal intubation according to local protocols and rescuer experience. In settings where video laryngoscopy is immediately available, it is preferable to use video laryngoscopy instead of direct laryngoscopy.
📌A sustained ETCO trace on waveform capnography must be used to exclude oesophageal placement of the tracheal tube.
📌Once a tracheal tube or a SGA has been inserted, ventilate the lungs at a rate of 10 min-' and continue chest compressions without pausing during ventilations. With a SGA, if gas leakage results in inadequate ventilation, pause compressions for ventilation using a compression-ventilation ratio of 30:2.
📌If using mechanical ventilation, use a volume-controlled mode during chest compressions set the ventilator to a tidal volume of 6-8 mL kg-' (predicted body weight), or to achieve a visible chest movement, the maximum inspired oxygen, a respiratory rate of 10 min-', an inspiratory time of 1-2 s, a positive end expiratory pressure (PEEP) 0-5 cm H2O, the peak pressure alarm at :0-70 cm H20, and the flow trigger off. Ensure mechanical ventilation is effective and if not, use manual ventilation.
📌If standard airway management strategies (oropharyngeal airway and bag-mask/supraglottic airway/ tracheal tube) fail during cardiac arrest, appropriately trained rescuers should attempt surgical cricothyroidotomy to enable oxygenation and ventilation.
Can emergency thoracotomy save lives in resource-limited hospitals? A Cape Town study shows promising survival outcomes, 24% to hospital discharge! @stemlyns
https://t.co/MszUIeWVwn
OMAGGIO A VITO PROCACCI
LA BIENNALE SIMEU è dedicata al collega barese che ci ha purtroppo prematuramente lasciati.
Vito voleva che si parlasse ai giovani di #Medicina e di #Servizio, parole che per lui iniziavano con la maiuscola.
E #SIMEU farà come voleva lui. 💙
#fieridiMEU
🤝 Exciting news! THOR has signed an MoU with the Italian National Blood Centre to advance trauma care & transfusion research through global collaboration.
Together, we’re committed to protecting donor & patient health worldwide.
#THOR#RDCR#TransfusionMedicine#GlobalHealth
Do you intubate people?
I made this video to guide colleagues on infant intubation but it’s apparent that it contains essential tips for ANYONE using direct laryngoscopy or standard geometry videolaryngoscopy regardless of whether it’s on adults or paeds
After all, adults are just grown up infants, amiright?
https://t.co/RnCb394vLX
E’ uscita la monografia sul trauma toracico che ho curato insieme a Geminiano Bandiera per conto di @SIMEU_EM
Scaricatela qui
https://t.co/EfyP0idAZQ
Grazie a tutti gli autori per il contributo. Un grazie particolare Fabio De Iaco ed Alessandro Riccardo per il supporto
Videolaryngoscopes for advanced complex airways.
Comparison of the Medtronic McGrath VL Xblade and Storz VL Dblade.
They look similar but the intubation experience is different.
Plastic vs metal, different camera position, different lux light, different handle, different weight, different width of blade, different tip.
@airwayGladiator@VirtueOfNothing@jducanto@NaveenEipe #foamed #VL
*⃣IL VALORE SCIENTIFICO DEL PROGRAMMA È IL PUNTO DI FORZA DELLA #BIENNALE#SIMEU, la Prima Giornata Nazionale di #Studi in #Medicina di #Emergenza#Urgenza (Bari, 28-29 maggio)
👉Per info : https://t.co/FEOcnr0NbV
⭐️Early Bird Price fino al 15 aprile. 👉Non perdere l'opportunità!
🚨 SAVE THE DATE! 🚨 The COR CONFERENCE this September will feature the legendary @amalmattu for an unmissable session on Emergency Electrocardiography Interpretation! ⚡🫀
📅 September, 24-26th 2025 📍 https://t.co/7Z61bctRUZ
🔗 Register now: https://t.co/0w9C1AFG98
#COR2025 #ECG #EmergencyMedicine #AmalMattu #CriticalCare #Cardiology #intubatiem
REGISTRATION: [email protected]
Let me know if you’d like any refinements! 🚀
#beyondacls
In the 8th Year our BEYOND ACLS changes skin!
TEE and Arterial Line in Cardiac Arrest in PreHospital, RESUS Hysterotomy, Double Defi, Change Drugs in refractory FV, Check the point of best compression in the MCE, Clinical study of TEE in preHospital and more… BEYOND the protocol!
Follow us for the BIG BEYOND of 2026 #intubatiem #resushysterotomy #TEEcardiacarrest
@GomorraDoc@MEDEST118
COR CONFERENCE 2025
A Must-Attend Event with ECG Guru @amalmattu !
September 24-26, 2025 – Lazise, Lake Garda
If you're passionate about ECG interpretation and want to learn from one of the world’s leading experts in Emergency Electrocardiography, this is the event for you!
COR CONFERENCE is the premier gathering for emergency medicine professionals, offering advanced, hands-on training in an immersive setting. This year, INTUBATI EM, an organization committed to providing top-tier emergency medicine education and bringing the best international expertise to Italy, is proud to bring Dr. Amal Mattu to Italy for the second time.
Why attend?
Direct interaction with Dr. Amal Mattu in an exclusive, small-group format
Advanced insights into ECG interpretation in emergency settings
A unique experience in a breathtaking location
Limited spots available! Don’t miss this opportunity— register now to secure your spot.
For more information and registration:https://t.co/0w9C1AFG98
𝑳𝒆𝒂𝒓𝒏 𝒇𝒓𝒐𝒎 𝒕𝒉𝒆 𝒃𝒆𝒔𝒕 𝒂𝒏𝒅 𝒆𝒍𝒆𝒗𝒂𝒕𝒆 𝒚𝒐𝒖𝒓 𝑬𝑪𝑮 𝒆𝒙𝒑𝒆𝒓𝒕𝒊𝒔𝒆!
Do you use ketamine as part of your routine clinical practice? Richards et al review the diverse effects of ketamine and its benefits in clinical practice. #ketamine#anaesthesia#perioperative#analgesia#surgery
https://t.co/chVbGOh9us
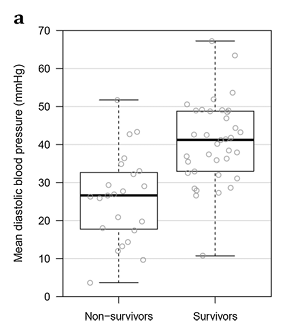
(3/x) #2: Arterial Line monitoring of CPR quality
This is a bit of a double edge sword.
Having arterial pressure monitoring for CPR is fantastic for:
1. Monitoring for ROSC --> reduce pulse check duration
2. Monitoring CPR quality --> diastolic BP (DBP) less than 30mmHg may be less correlated with ROSC
3. Theoretically can be used to titrate vasoactive medications
4. Distinguish between PEA and pseudoPEA
Out of these, number 1 and 4 are the most useful for me. Manually checking for pulses in cardiac arrest is notoriously inaccurate (even among skilled providers).
The problem? Placing arterial lines in cardiac arrest is hard (even for experienced clinicians!). Here are some tips:
1. Best operator available
2. Make sure you are going for common femoral (people sometimes go too low in cardiac arrest)
3. Have someone stabilize the pelvis manually (this reduces motion of the legs) ****
4. Ultrasound guided is a must (you will likely be venous blind because the vein is huge and artery is small in cardiac arrest)
Biggest error is becoming task focused on the access. Placing an arterial line is great when there are lots of skilled hands around, but when I'm a solo code team leader don't have the bandwidth to do myself.
PMID: 27107688 (animals although human data for this too)