Extending my gratitude to @ross_prager@arntfield for letting me come to London and see the great things you’re doing with point of care ultrasound (POCUS).
I truly appreciate your KINDNESS, HUMILITY and willingness to share your wisdom and knowledge.
#pocus#hemodynamics#vexus
Just out of the oven! Acute hemodynamic tests to determine the status of macro-to-microcirculatory coupling in septic shock. More and more validating data. In ANDROMEDA-SHOCK-2 great success in normalizing CRT with various tests (summarized in the text)! The way to personalize!!
Highlights from our episode out today on the new 2026 multi society PE guidelines! Thank you to @American_Heart for reaching out to collaborate and to @DrMarkCreager for coming on the pod.
Fun the full episode on our website, wherever you get your pods, or on YouTube
1/ 🚨NEW: POCUS in Kidney Disease: Cases That Changed Management
🩸If you’ve ever wondered “what should we do next?” in a patient with kidney disease — this episode explores how renal, lung and venous POCUS can help answer that question!!
📝:https://t.co/VrA2K80n70
Our VESPER team, led by Dr. @john_basmaji have recruited the first two patients into our RCT of venous congestion guided resuscitation in septic shock!!
Our goal is to understand how venous congestion can be used to guide decisions surrounding fluids, inotropes, RV support in septic shock.
Focus for VESPER right now is feasibility but we have already recruited two patients in the first week live!
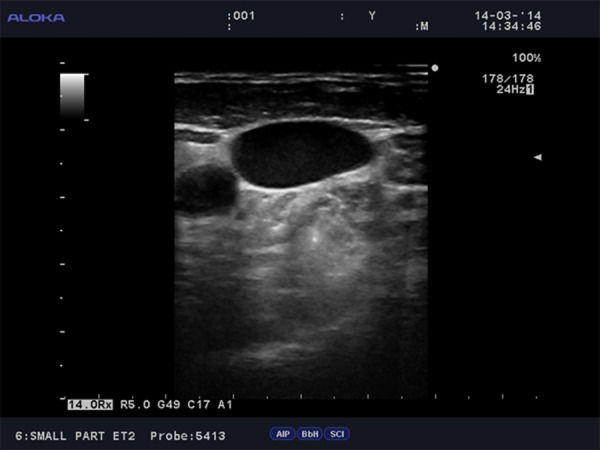
@ross_prager I use POCUS for patients with SSTI, sometimes ruling out an abscess by feeling fluctuation can be challenging. US gives me more confidence.
Clinicians can enhance patient understanding by using numerical data instead of verbal probabilities, consistent denominators, absolute risk comparisons, and clear context for unfamiliar data types.
https://t.co/cdjVDcZfvq
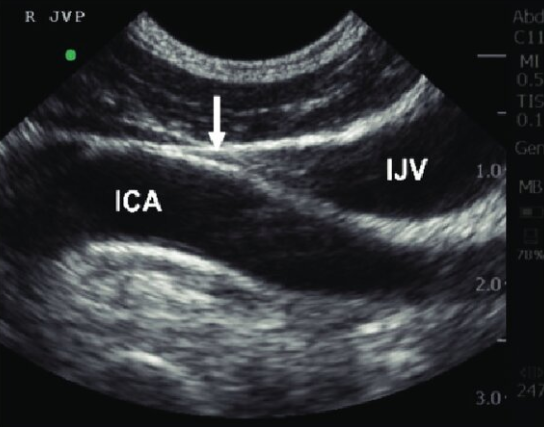
(1/3) What's the worst trend in POCUS for 2025?
Ultrasound to measure the height of the jugular venous pressure.
In fact, this might be the worst trend in POCUS ever👇
Do you have an innovative way to teach or an interest in publishing #MedEd scholarship? 📚🩺
I was honored to join the @ATSMedEd webinar to discuss how to craft and publish "How I Teach" papers for @ATSScholar and other educational journals. Great insights shared with @CardsNYC, Yuri Matusov, and Abi Kumaresan ! Watch the full session here: https://t.co/2l3xot8Mw8
🎥 #MedTwitter #FOAMed #FacultyDevelopment #Scholarship
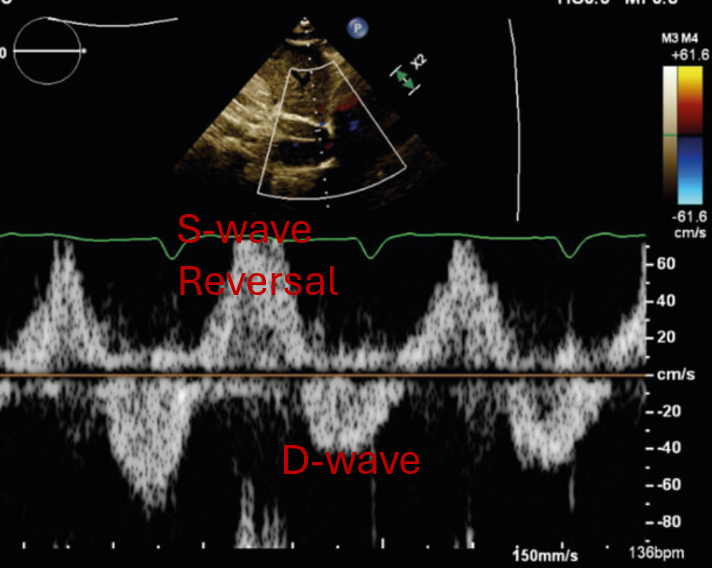
Patient with fevers, dyspnea, and hemoptysis. You place the echo probe and see this 😰
What's the diagnosis?
Here are some tips as an echo-loving ICU doc👇
in thyroid storm, treating sinus tach with a beta-blocker will occasionally cause death
many patients have reduced LVEF & compensatory tachycardia (borderline cardiogenic shock)
beta-blockers push them over the edge
what data supports B-bl in thyroid storm?
why do this?
A few thoughts on pericardial tamponade:
1. Clinical Diagnosis that is NOT binary - exists on a spectrum of symptomatic effusion to hemodynamic collapse.
2. Hypotension is a LATE finding when compensatory mechanisms overwhelmed - be wary of normotensive shock.
3. Congestive injury is present before forward flow is impaired from the PCE --> we have a great case report that is being reviewed of a PCE with severe venous congestion that is improved by pericardiocentesis, when there are no features of tamponade.
4. Echo features suggestive of tamponade include:
- Pericardial effusion (remember, smaller effusions that appear quickly can cause tamponade)
- RV diastolic collapse
- RA systolic collapse
- Dilated IVC
- Excessive MV and TV inflow variation
- Low LVOT VTI (not a classic one, but hugely valuable as a sign of shock early)
- VTI variation (an echo correlate to pulses paradoxus where LVOT VTI is a surrogate for SV which causes the BP variation seen in pulses)
5. Drainage should be done before the patient is in extremis - ultrasound useful to landmark best approach, but most clinicians do not use realtime needle guidance (some do, but most landmark with U/S)
6. Be wary of draining larger chronic effusion to quickly, especially if there is a degree of RV dysfunction. Rapid drainage can decompensate RV failure
7. Regional tamponade (e.g. post cardiac surgery) is a different beast - search chamber by chamber carefully in 2 views (on TEE) to identify chamber collapse. Isolated RA / LA tamponade common and can cause atypical hemodynamic tamponade compared with circumferential PCE
See this example of regional tamponade with RA clot here.
What other pearls am I missing?
1/🚨NEW #BehindTheScenesInterview: What is “Fluid Tolerance” and how can VExUS help guide us?
Don’t forget- strong basic POCUS skills are essential before using VEXUS ‼️
🎥:https://t.co/zQEDdmvRIa
🎥: https://t.co/QgTied20jt
🖥️:https://t.co/vYhM3qu2dh
2025 has been a tough year for me professionally - here are some of the thing's I've learned🧵
Fail fast
Listen to your gut
Do Less = More Focus
Productivity is not impact
If you never give up you never lose
Stay on the steep part of the learning curve
Automated, Delegate, or Deprecate as much as possible
(1/x) For venous congestion, it turns out that the same Doppler pattern can have different prognostic and therapeutic significance depending on the underlying cause.
These have been coined congestive 'endotypes'.
Here's how I think about them👇
1/ 🚨 NEW episode on venous congestion & the VExUS score 💧
Venous congestion is a century-old concept, but modern tools now allow clinicians to detect, quantify, and monitor it ‼️
🖥️: https://t.co/CeJBrZr3qr
📊 Research Summary: Adults with #AFib who drank at least one cup of caffeinated coffee daily after successful cardioversion had a lower risk of recurrence than those who abstained from coffee and caffeine.
#AHA25
https://t.co/CoGRhvpUbZ