BSc in Sports Rehabilitation & Athletic Therapy. Interned at Stanford University, California. MSc in Physiotherapy in Kings, London. Private practice physio
Keith Evans is sprinting at maximal speed, then has to absorb 3–6 times his bodyweight in braking forces just to give himself a chance of making this play. Deceleration is a skill.
'A silent disability’
At the time of writing, it’s about 8 months since I ‘walked’ out of the Cleveland Clinic into bright sunshine, on crutches, fearful and unable to stand upright
I’ve recently accepted that I have a mild form of PTSD after my 6 weeks as an in-patient – an abstract clinical nightmare world, heavily medicated – an environment in which I’ve spent 20 years of my career, patrolling with confidence and empathetic dissociation
Then suddenly I find myself on the other side of the fence, in a sterile cubicle and bed - separated from my family and close friends, battling suicidal levels of pain due to disciitis and radiculitis – all the while bacteria feasting on my vertebrae, lying on the floor of the toilet crying and begging for help, the patient in the bed opposite swearing at the staff to assist me - banging my head against the radiator
And yet there is no effective help to be offered
“You aren’t due your next Oromorph for another 2 hours”
“Would you like to try an ice pack?”
I still find it hugely triggering to return to the hospital for yet more interval imaging – hoping that my staph aureus devoured L4/5 segment is finally nearing natural bony fusion
Whilst in the MRI machine again today, I passed the tedious hour by doing rough mental calculations -
In the last 12 months:
1000 hours lying in a hospital bed slipping in and out of false sleep, picking up where I left off in familiar nightmares
20 hours of MRIs, CTs, biopsies and X-rays – fighting desperately to keep still, despite my legs being 'on fire' – rolling off the machine bed like an invalid
42 hours of intravenous antibiotics via my PICC line (I can still see the small scar from this, a tiny medical tattoo lest I ever forget the journey passed)
I went into hospital at 105kg – I left at 83kg
As the patient, you don’t recognise the changes as they are insidious – the mirror deceives you – but to others its stark. It’s been upsetting to hear friends confide that they found it harrowing seeing me after my discharge
“You looked 60 years old mate”
“I didn’t recognise you – I called my sister after I saw you to talk about it and cried over the phone”
“I didn’t know what to say”
And then, function improves, but at a glacial pace – when I first returned to work at limited hours, I had to stop several times walking up Threadneedle Street to the clinic from Bank tube, sat embarrassed on the pavement, waiting for the heaviness in my pelvis and legs to subside
“You alright mate?”
Now I can undertake low level exercise. I have days when I appear ‘normal’ to colleagues. The bilateral foot drop is subtle and, with focus, I can tame it. But I still trip if I’m not paying attention. It is variably wearing and upsetting.
And, so, it seems to those around me that I have recovered. But I haven’t – not fully. Physically nor mentally.
I still have daily pain and it can be exhausting. They can’t see my feet that feel ice cold, ache, swell - insensate. They don’t belong to me.
I’m an inch shorter than this time last year. My posture has changed - I feel & fight it constantly – slouching is my constant aesthetic nemesis.
I can't look at myself in the mirror. I can’t lie flat on my back because of the kyphotic deformity. Simple things. I can’t have a bath.
I used to play off 5 in golf, I was a sub 12 second 100m sprinter - now my daughters have to help me put my socks on in the morning
Once you’ve left hospital, the battle isn’t over – there is the task of arduous self-directed withdrawal from the heavy-duty opioid and benzodiazepine medication, which never seemed to do anything anyway
Hello ‘Trainspotting’
Now I just take ibuprofen occasionally
The mornings are the worst – waking up to the familiar rat gnawing on my shins. I kick and lash out at it to get it off, half asleep, imagining it to be under the duvet, but it’s not there
I’ve worked out that the longer I stay in bed, the worse my symptoms are into the day – so I flop inelegantly out of bed onto the floor at 5am, stare at the ceiling for 10 minutes and try and find some peace listening to the birds outside, cursing my lot
I have a silent disability
On the Tube I cast my eye over the posters that remind commuters that not all ‘disabilities are visible’ – a rueful smile
And wrestling with the uncertainty:
Is this as good as I’m going to get?
Will I be like this for the rest of my life?
Do I have any other options and at what further cost?
If it’s a struggle now, how will I cope in 20 years time?
How will I support my family?
And in darker moments - what did I do to deserve this?
It sounds bleak – and it is – but there are some positives to grasp hold of:
A different perspective on life – prioritise health, family, friends, interests…. not work
A different level of empathy – I can truly acknowledge a patient’s suffering based my own lived experience – this has made me a more rounded, compassionate doctor
I can share tested, real world management strategies
All the clothes that were too small for me that I insisted on keeping, much to my wife’s irritation, now fit me again – a whole new wardrobe at no cost!
I’ll admit I’ve had some tearful conversations with patients when trying to discuss this and share my experiences – but despite my reticence, the feedback has universally been that they felt closer and more trusting of me having seen I’m a ‘human being’, not a clinical robot.
And so we push on. What other choice do I have?
Riding a wave of support from closer friends and family.
I will get there.
@DrJN_SportsMed@marklaslett_NZ Thanks for sharing James. I hear you on the silent disability. Keep showing up consistently and things will improve eventually.
The Endurance Performance Pyramid.
Start with a strong base of consistently, recovery and fuelling and then progress up the pyramid by building volume then adding intensity and S&C.
Consult a Running Coach for a plan to achieve your goals 🥇
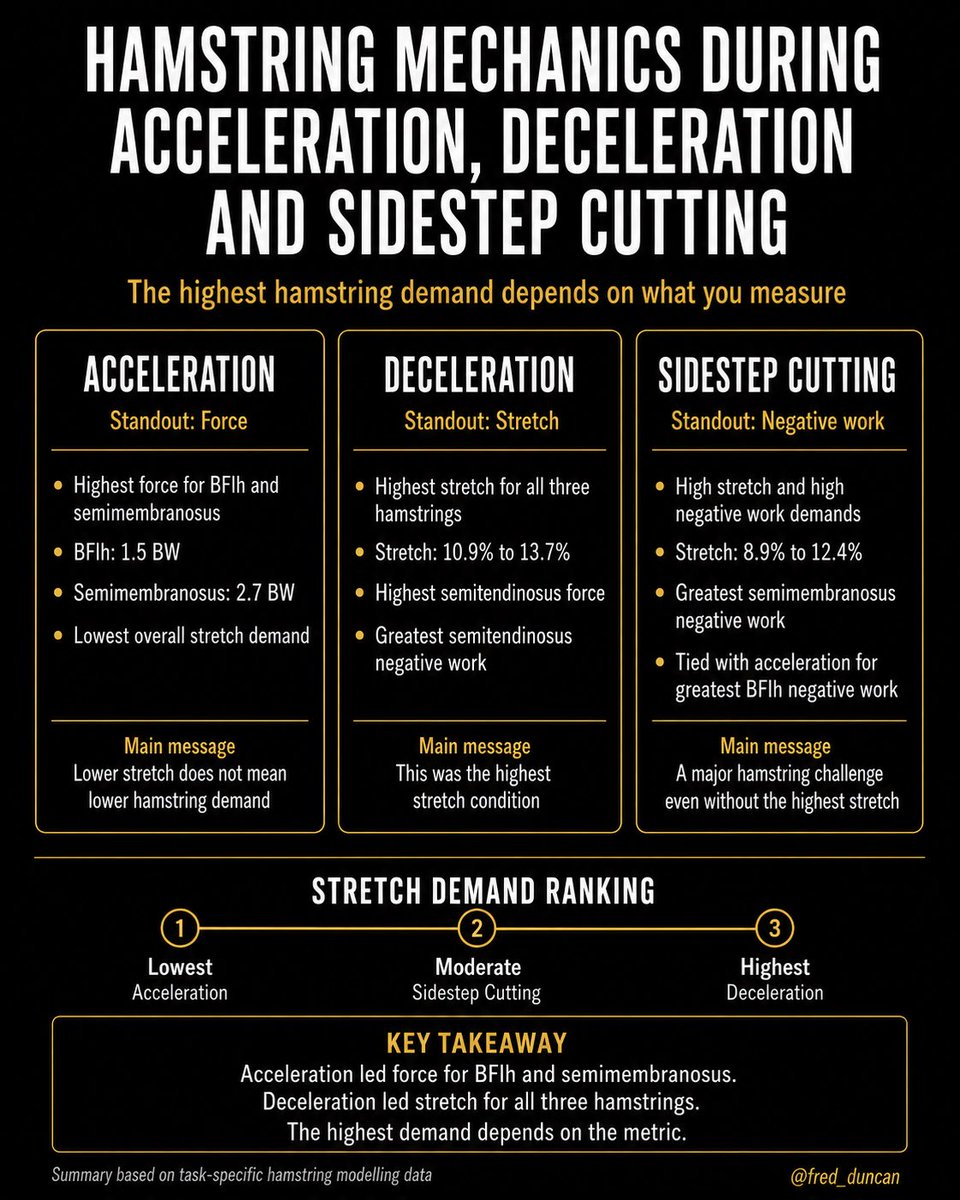
Acceleration, deceleration and cutting all involve the hamstrings, but they don’t challenge them in the same way
This is why we need to understand the mechanical demands of specific movements and skills so we can prepare athletes for what they are going to face.
These are
When athletes can handle higher speeds and control them, it shows up everywhere
Because braking capacity isn’t just a quality, it’s a separator
Total time can look the same, but how it’s produced isn’t: entry velocity + decel = performance
Overview:
-Basketball demands high braking capacity in multiple directions, especially in defensive shuffling
-Total time alone misses how movement is produced, with deceleration possibly being a key driver
-This study tested whether linear braking ability differentiates lateral movement performance
Methods:
-124 NCAA Division I basketball players (Guards and Bigs) from 10 Power 4 programs
-Two tests: 10m ADA Test and m5-0–5 lateral shuffle test (both directions)
-Athletes were split into high vs low deceleration groups based on ADA results, then compared in shuffle performance
Results:
-Athletes with higher linear deceleration performed better in the lateral shuffle, with faster total time & higher deceleration
-Differences were meaningful across both Guards and Bigs, with moderate to large effect sizes
-Better performance was driven by a combination of higher entry velocity and greater braking
Discussion:
-Braking capacity is a key driver of multidirectional performance, better decelerators move better across tasks
-It separates athletes who can handle higher speeds and forces in multiple planes
-Treat deceleration as a KPI: profile it, train it, and expect it to transfer
🧠 Researchers: Adam Petway, @DHMov , @Dr_DanielCohen , @OlaAthletic1080
🚨 Just Published 🚨
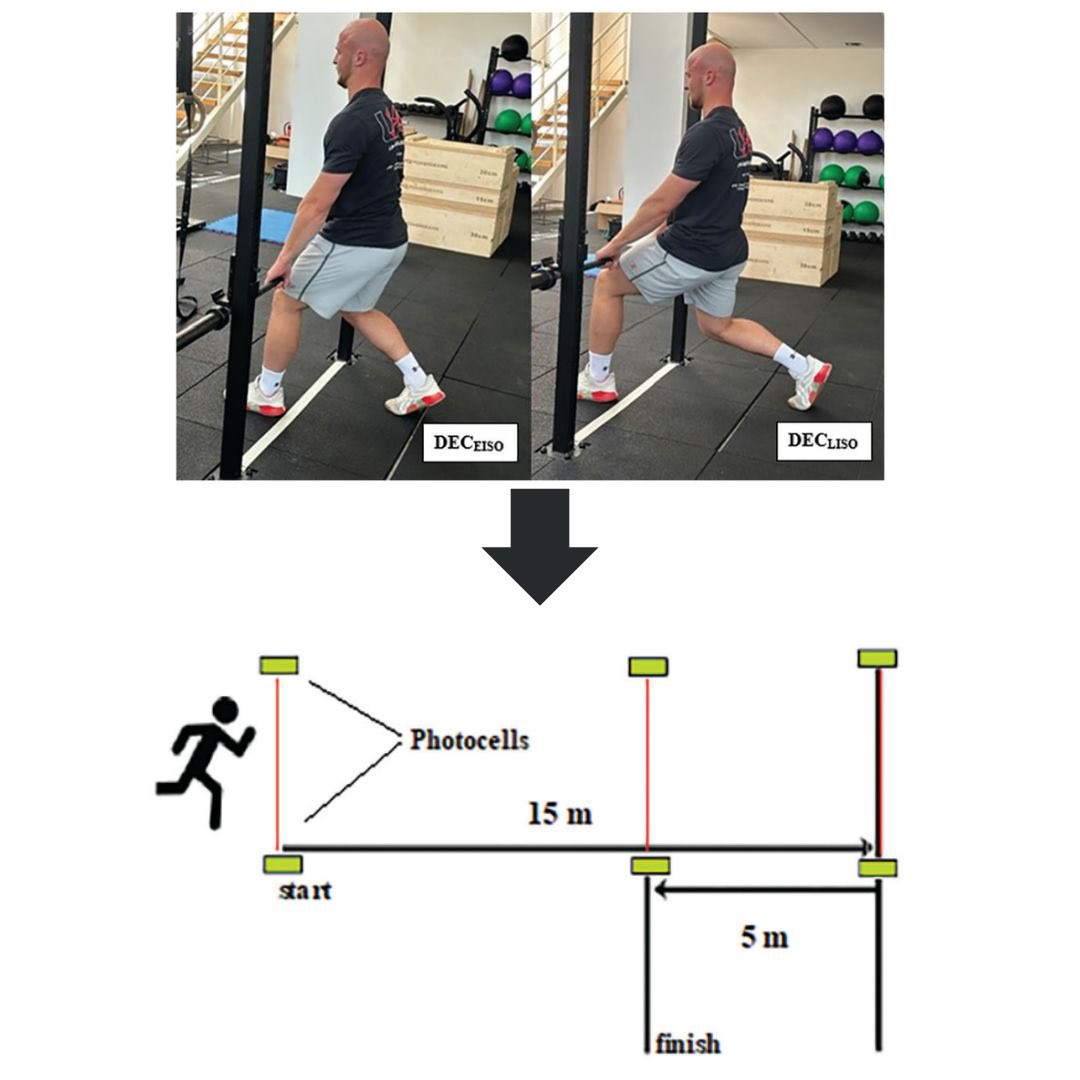
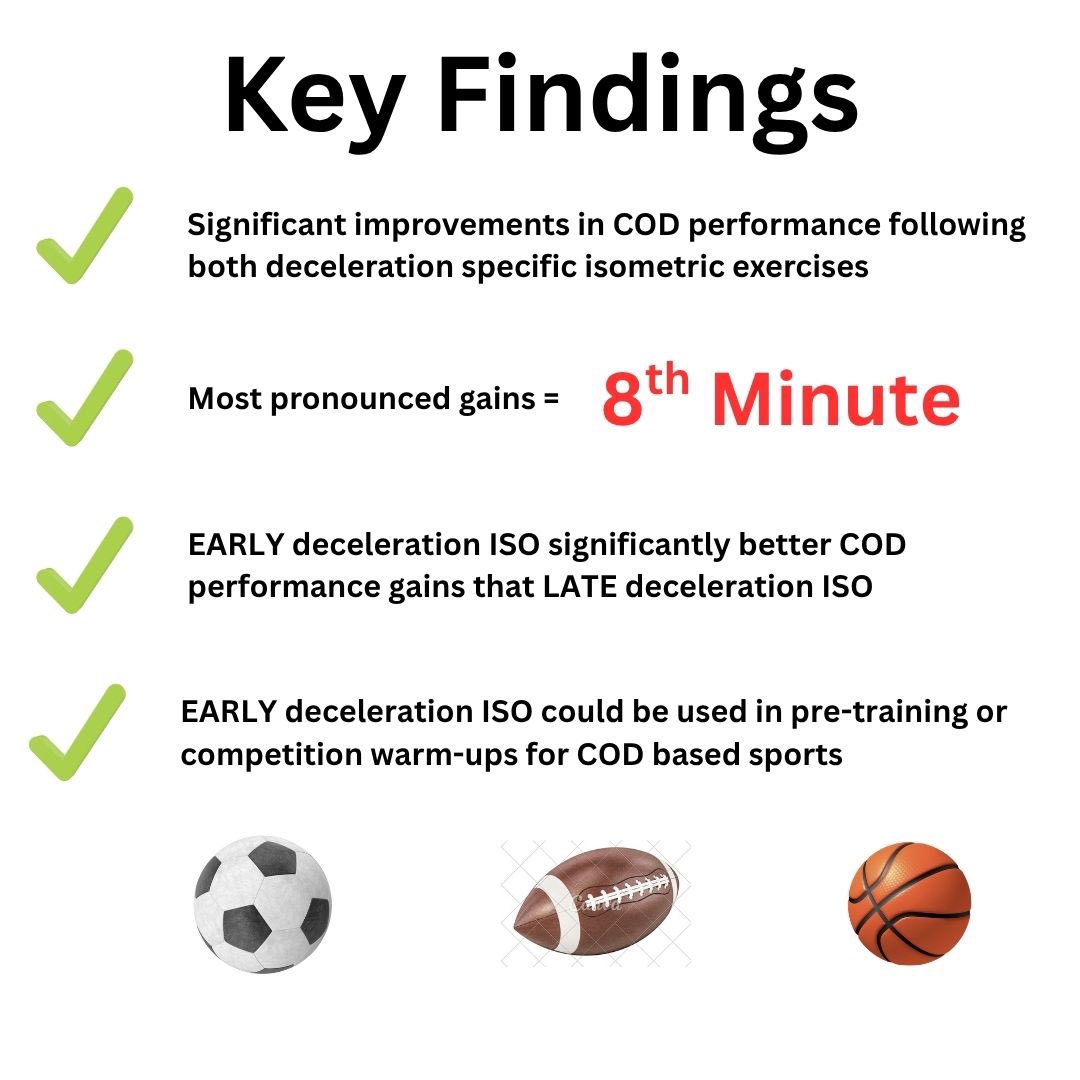
DECELERATION specific isometric exercises acutely enhance change of direction performance in academy ⚽️ players
✔️ 8th min most pronounced gains & with early DEC-ISO position
✔️ Application to pre-training or competition warm-ups for COD sports 🏈⚽️ 🏀👇
🌽 Husker Power… the MASTERY of strength & conditioning
Boyd Epley is often thought of as the “godfather of strength & conditioning.”
His program at Nebraska 4 decades ago changed the game & we can STILL learn from it
Here, he details some of his speed development tools
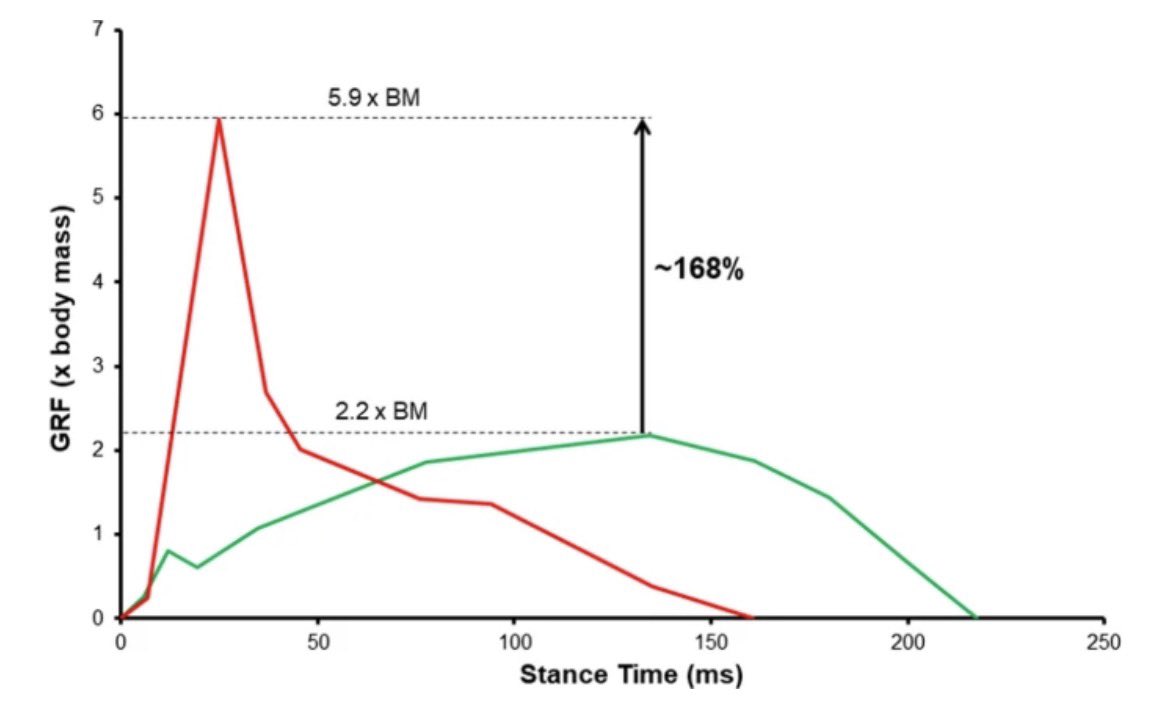
🚨 Biomechanical & neuromuscular performance requirements of horizontal deceleration…
📌 High Impact Forces ⚡️
(2.7 x ⬆️ than acceleration)
📌 Braking for Rapid COD 🔑
📌 High Eccentric Muscle Forces 🟰 Risk of Damage
📌 Braking Kinematics 🦵
🔐 https://t.co/mn37gFCRXa
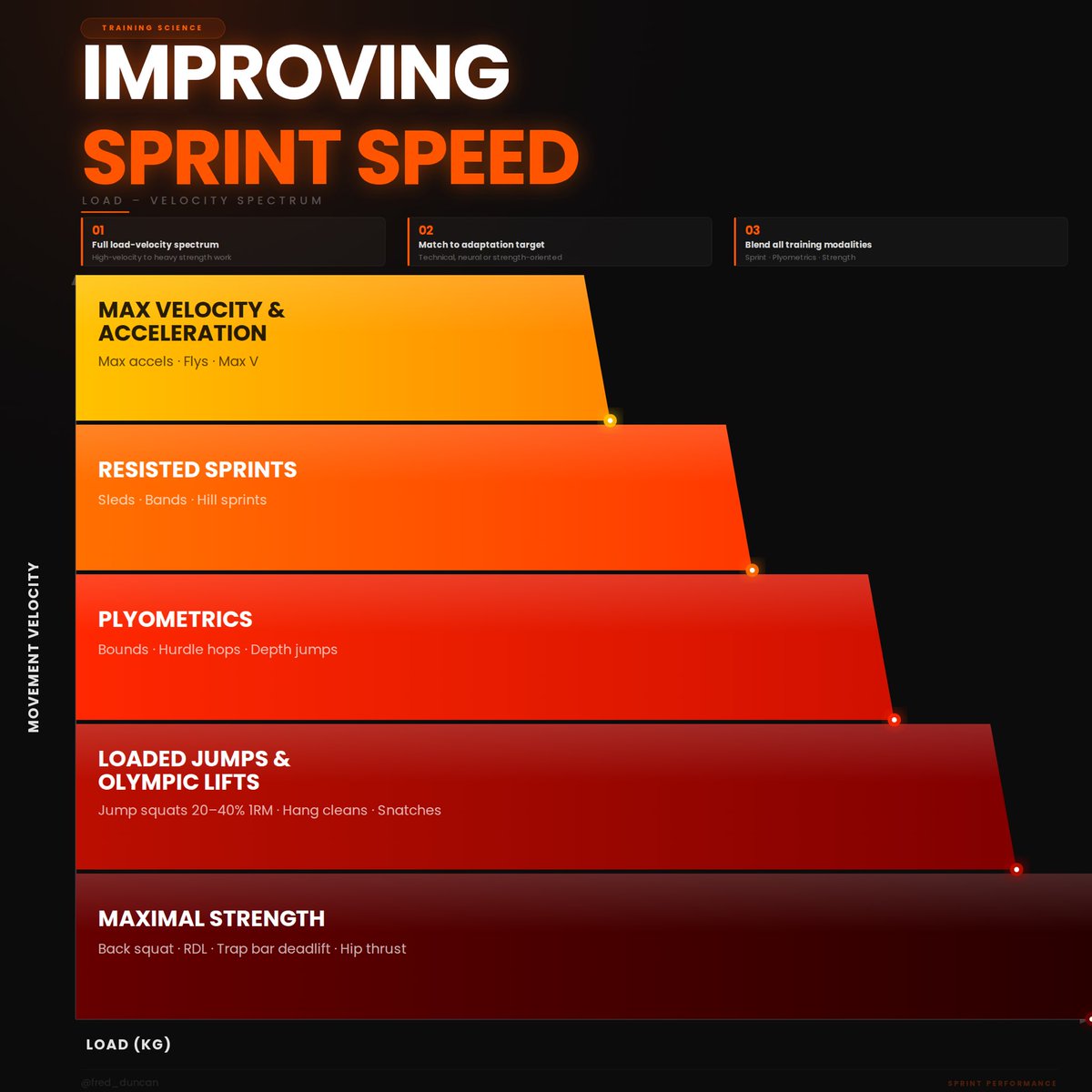
Speed isn’t built in one lane…
You need exposure across the entire load–velocity spectrum, from true max velocity work to heavy strength, each serving a different adaptation.
Most programs overemphasize one end and ignore the rest.
Inside Speed Kills, I break down
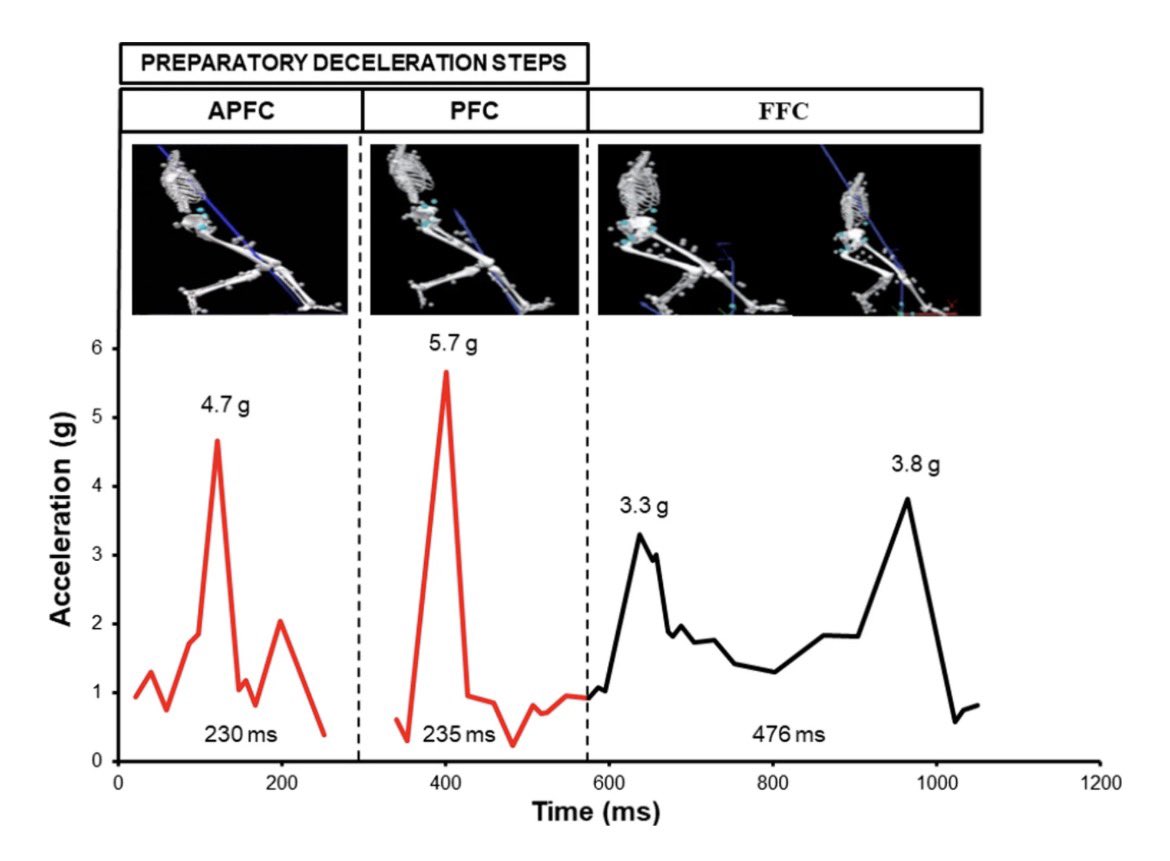
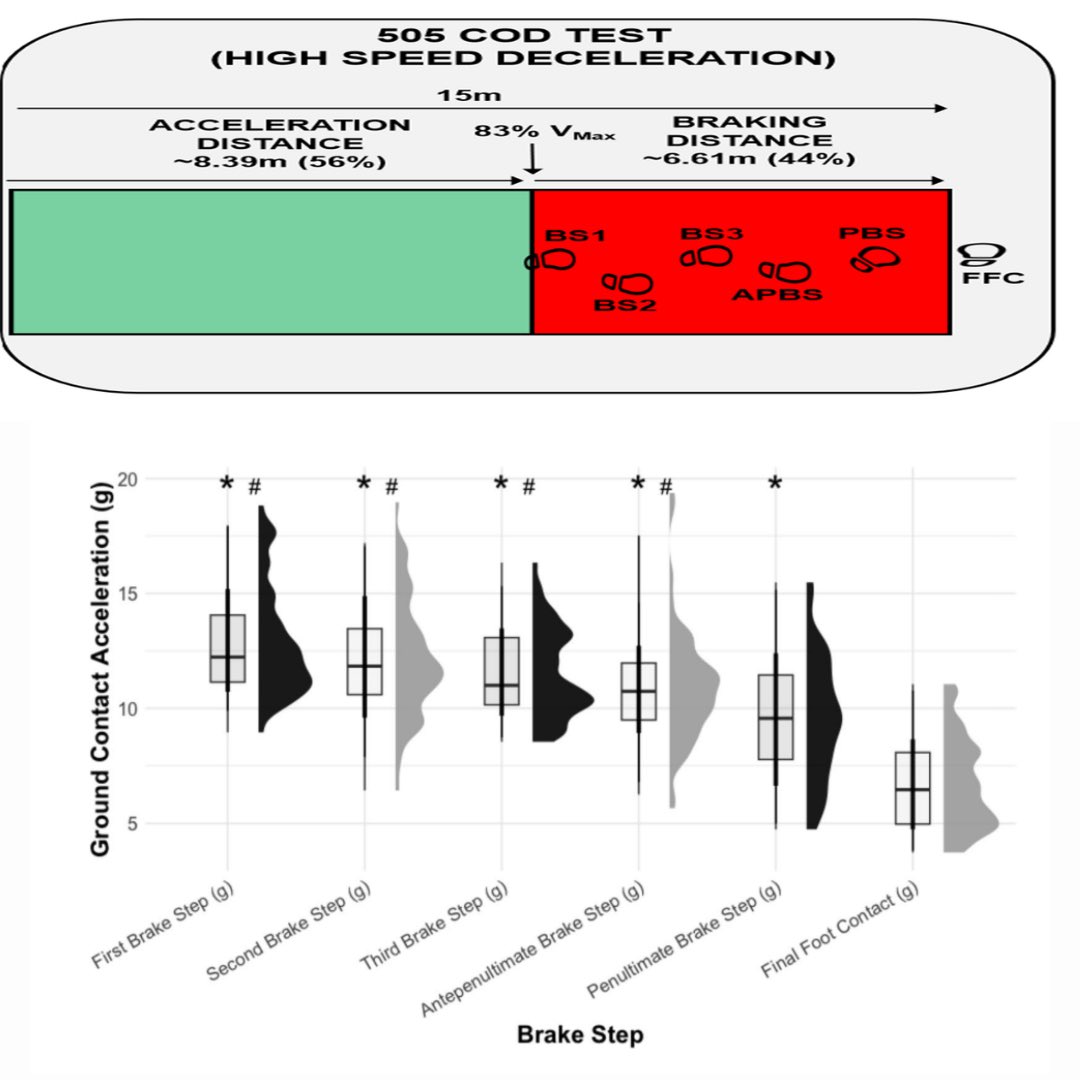
🚨 BRAKING step forces in a 505 change of direction test (high speed deceleration)
Here we show data on ALL braking steps…
🔎 Brake Step 1
🔎 Brake Step 2
🔎 Brake Step 3
🔎 APBS
🔎 PBS
🔎 FFC
Forces highest in early braking steps!!
Read here: https://t.co/lz2feXjvPs
82 nóim
@DingleGAA 0-23
@StBrigidsRos 1-19
Mikey Geaney leis an iarracht agus Geaney leis an scór chun an chluiche a bhuacaint!😱🤯🤝
After a titanic battle, Dingle are All Ireland Club Champions after extra time!!
BEO/LIVETG4 AR @TG4TV 📺
#GAABEO
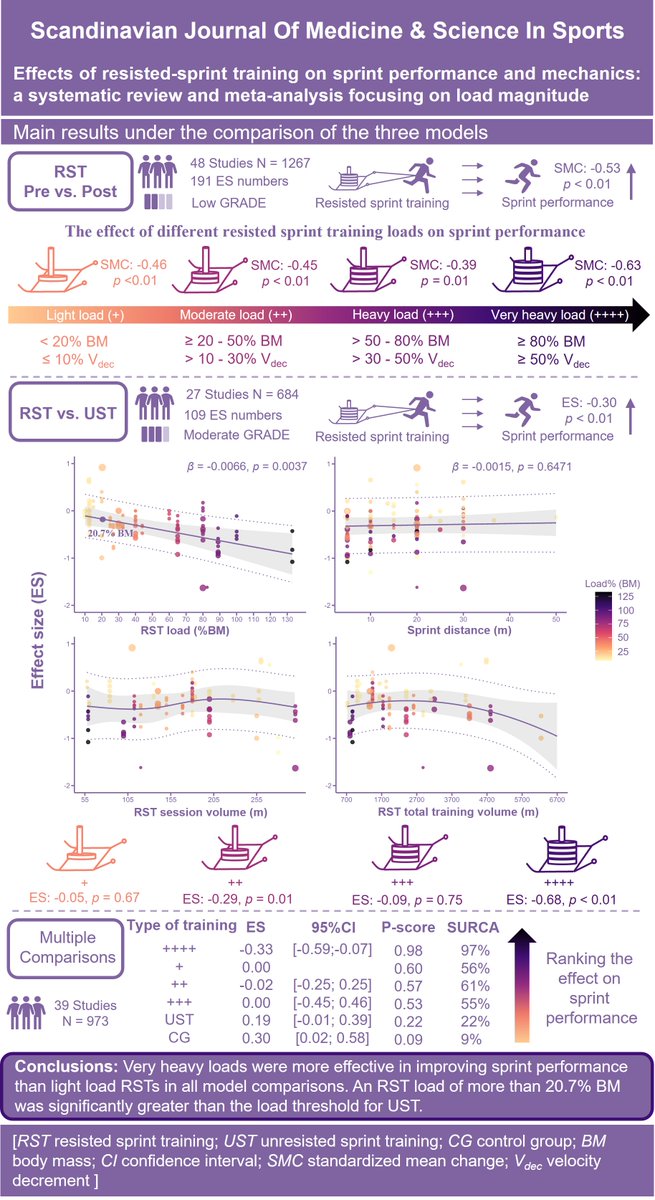
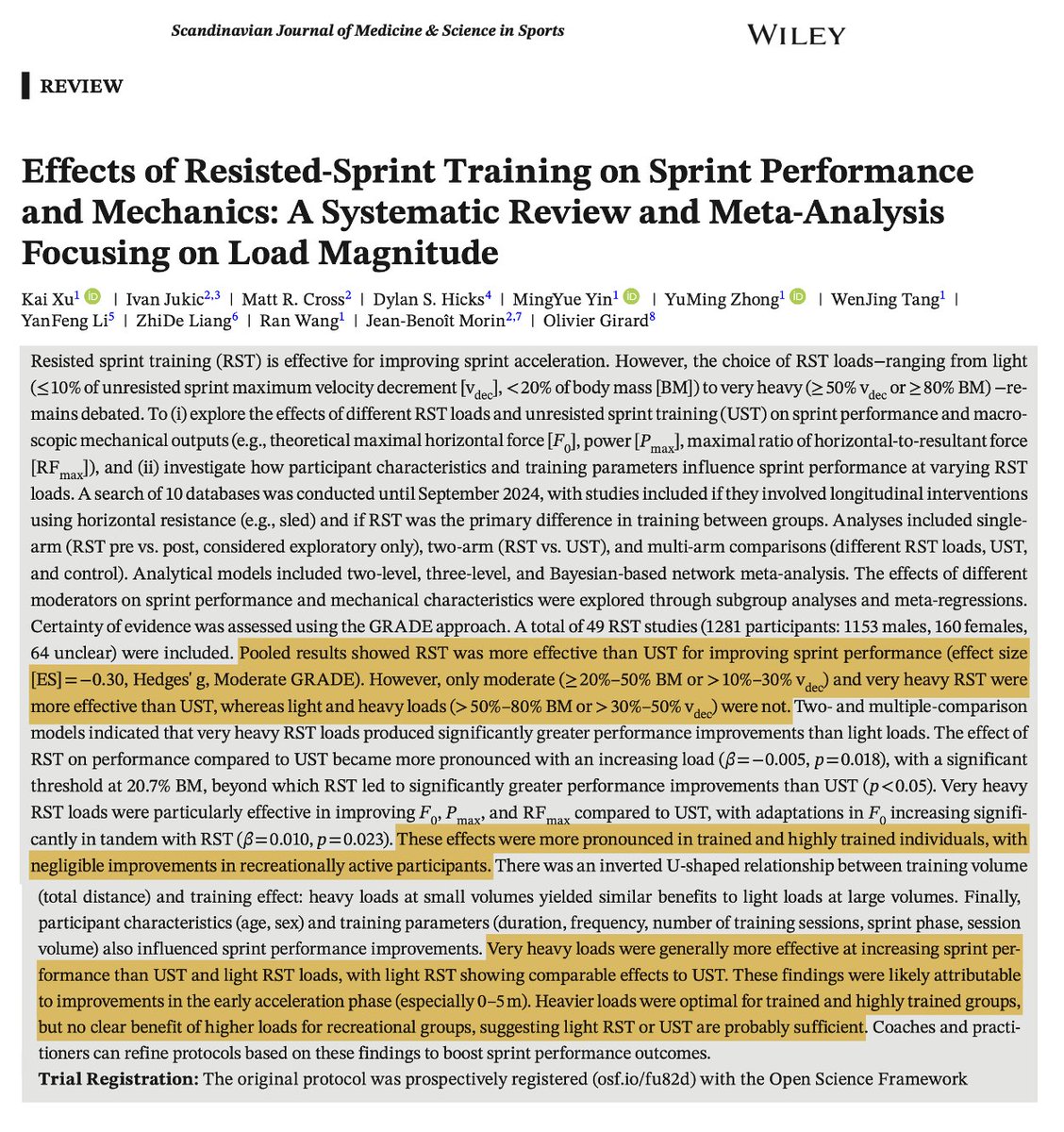
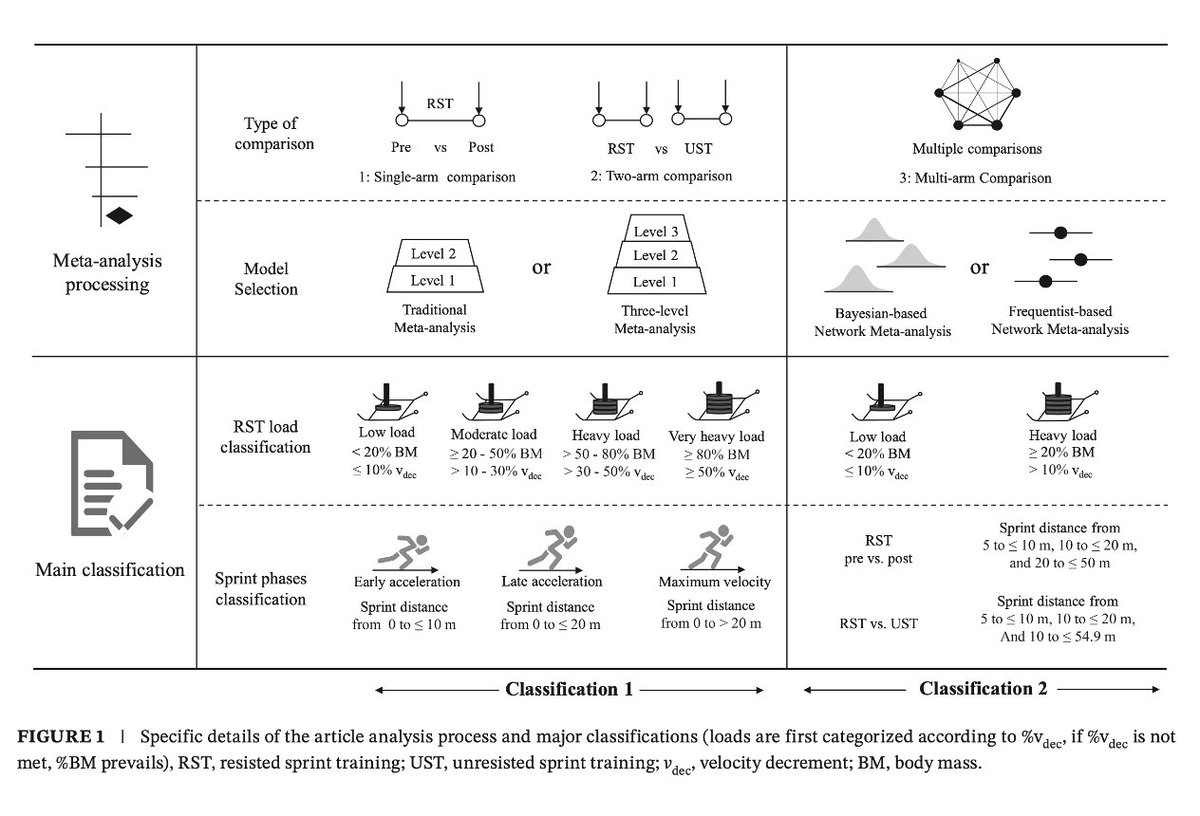
🚨NEW PAPER🚨
Resisted sprint training🏃♀️, FINALLY (was about time) a detailed meta addressing LOAD as a key variable: as for 🏋️♀️, "resistance training" means nothing without this nuance💡
Great team🤝work by @Xukai382031
From now on, a reference paper✅
https://t.co/f38UMbVu7h
Hamstring injuries in multi-directional speed sports...not all SPRINT related❗️
⚽️ 31 % Braking Stopping
🏉 18% Decelerating
🔎 Trunk & hip flexion with knee extension
🟰High eccentric strain
Braking movements with high eccentric force could be tools in hamstring injury ⬇️
Paul Geaney’s leadership today was a template for every player.
In the swell of the Bars’ surge, he stood up and asked for the ball.
Took his goal with certainty, took his knocks without pause.
Patched up, back on, and never once hid from the moment.
A leader in the truest sense, present, persistent, unshakeable.