When a large employer pays so little that their full time employees qualify for Medicaid , (or any public assistance ) we the taxpayers are effectively subsidizing that big company. That’s wrong
This is a good start. PBMs should not be able to offer Formularies at all. They should be required to provide all claims data to employers and manufacturers. Among other things
Thesw alone could cut pharmacy pricing in half for the most widely prescribed brand drugs
@TakeMeSerial@AndrewYang The first step is becoming isolated in a lot of cases, which is something Reeves does document i.e., the hikikomori in Japan. After isolation and purposelessness more aberrant behavior is likely to appear. Evidence for social media and aggression https://t.co/EUuGP41cMs
@TakeMeSerial@AndrewYang There’s actually a lot of evidence that social media and smartphones are toxic for children and adolescents. Read Anxious Generation by Jonathan Haidt. This is not something political.
For the doctors out there: It’s time we talk about how unfair the business of medicine has become for providers. If you’ve tried to negotiate fair pay with insurance—whether it worked or not—I want to hear your story. Tag me or share it in the comments. We can’t fix what we don’t talk about.
For far too long, big drug middlemen called PBMs have inflated drug prices. Not anymore. Arkansas is leading the way protecting our seniors, veterans, and everyone else who relies on their local pharmacy to stay healthy
https://t.co/Hn2WbO4k0D This is an important story because it debunks one of the favorite PCMA talking points.
The State of Ohio fired Optum and CVS as the Medicaid PBMs and started a state-run PBM.
They were able to save $140 million and increase the payments to pharmacies by 1200%.
They now have a system in which 99% of pharmacies are available to Medicaid patients, and the pharmacies are thriving.
This proves that we DON'T need the large PBMs, and we need PBM reform now at the federal level.
Another insurance denial. Another patient put at risk.
We did everything right. My PA saw a patient with signs of a Deep Venous Thrombosis (a dangerous blood clot). We ordered an ultrasound, confirmed the diagnosis, and prescribed the medication to help prevent dangerous complications. But her insurance denied the medication.
Why? They wanted “more clinicals.” Despite an in-person examination. Despite appropriate documentation. Despite the ultrasound result showing a blood clot. She was sent home from the pharmacy without the treatment she needed.
If I failed to prescribe the medication, I would be held accountable for putting this patient at risk. When will we admit that insurance companies are practicing medicine? When will we hold companies and individuals accountable for delays in care?
I am going to continue to share these denials with you so you can see what it is like to be a doctor in 2025. We have to fix this—for patients, for providers, for all of us. If you have a story, please share it with me. Let’s change this.
Takeaways from #ACC2025. Late breaking trials - take home points
@ACCinTouch
1. WARRIOR Trial : Intensive medical therapy did not significantly impact the rate of serious cardiovascular events at five years in women with suspected ischemia with nonobstructive coronary arteries (INOCA).
Had our second annual Fellow Research Retreat!
Congrats to our winners this year:
🥇Nick King
🥈Alex Dang
🥉Martin Chacon (@MartinChacn)
Looking forward to next year's retreat!
The Cost Conundrum was an article written in 2007 in the New Yorker by famed surgeon and author, Atul Gawande that sought to explain the high cost of American medical care.
It was inspired by data from a health policy researcher from Dartmouth named Eliot Fisher. Fisher’s group had mapped Medicare spending of every county in the U.S.
McAllen, Texas had the distinction of having the second highest per capita Medicare spending in the country, and it was this town Gawande traveled to, to write his article.
Gawande, an academic surgeon from one of the elite medical centers in America wrote with some distaste of a two filled with strip malls with small independent private practices dotting the landscape that were making handsome profits by billing fee for service Medicare to the max.
Gawande provided a stark contrast to this low value, profit driven care by traveling to a high value, low cost county — the Mayo Clinic.
A visit to a surgeon’s clinic at the Mayo Clinic told the story of an hour long discussion with a patient followed by a cardiologist materializing within 15minutes from another floor to help ready a patient for surgery the next day.
How did they do this?
Gawande’s words :
“..decades ago Mayo recognized that the first thing it needed to do was eliminate the financial barriers. It pooled all the money the doctors and the hospital system received and began paying everyone a salary, so that the doctors’ goal in patient care couldn’t be increasing their income. Mayo promoted leaders who focused first on what was best for patients, and then on how to make this financially possible.
No one there actually intends to do fewer expensive scans and procedures than is done elsewhere in the country. The aim is to raise quality and to help doctors and other staff members work as a team. But, almost by happenstance, the result has been lower costs.”
The answer to the health care cost problem lay in this elegant article. The plan as initially forwarded by Eliot Fisher from Dartmouth and now gracing the pages of the New Yorker was to create “Accountable Care Organizations” in the image of the Mayo Clinic.
Convert McAllen, Tx to Rochester, MN and the nations problems would be solved.
As a young medical trainee reading his article, I was sold.
But I never stopped to think of how Mayo was operating in this manner. How could a surgeon at Mayo afford to spend a whole hour with a patient? How exactly does a cardiologist have time to run down in the middle of the day to discuss a complicated patient? If the cardiologist doesn’t bill the consultation, how is the cardiologist being paid?
1/x
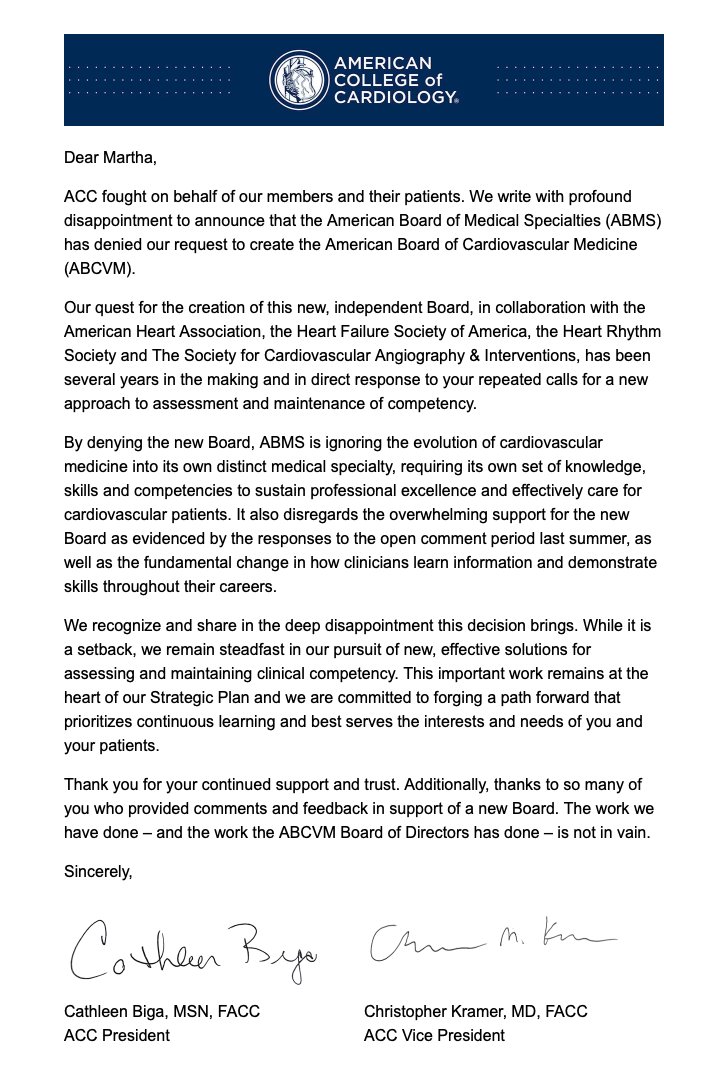
This is such sad news.
I think we all wanted @ACCinTouch to take over our certification in #cardiology & not leave to the ABMS.
Cardiology is often a Department, not within a Division of Medicine. We need to separate to make this happen.
😢😢😢 #CardioTwitter
@independentMDs When more than half your time is spent in front of a computer clicking, writing notes (bills), and putting orders it is understandable. EMRs are taking the thrill away from medicine. You can see it on every annual medscape survey.
Dear Hospital Admins: Requiring board-certified intensivists to have ACLS is redundant. Requiring them to also spend time and money on BLS is ridiculous.
Sincerely,
Someone who probably leads codes far more often than the BLS teachers
. @BillAckman@elonmusk@doge if you want more, on the healthcare side too, I got trillions worth.
The arbs in this industry are insane. For instance, here is an example of how insurance companies with Pharmacy Plans for traditional Medicare game their plans to push people to Medicare Advantage
In their traditional Medicare Pharmacy Drug Plans, they use co-insurance. Which means the patient pays a percentage, usually around 20% of the retail price that they effectively set themselves. So a $600 drug like Elliquis costs them $120 each month
They don't use co-insurance for their Medicare Advantage plans where they profit about $1747 per year per patient.
So one has $120 monthly costs. The other has maybe a $25 co-pay.
So they are pricing to push people to their most profitable plans and extract more money in Medicare PDP plans
The bad part, beyond the money out of pocket that should be far less, is that CMS approves all of these plans and did nothing to help reduce the out of pocket for those with PDPs. They are stuffing money onto the pockets of the plan owners
Want to know one of the biggest problems in healthcare? Deductibles.
Deductibles are defined by the plans the insurance companies design. Then they are approved to be offered by the feds or employers. Then we the people decide what deductible we want when we choose our plans.
Often we choose higher deductibles because we are healthy or because we can only afford the lowest premium plan.
When we got get care and can't pay our deductible for whatever reason, you know who takes all the credit risk and losses?
Doctors, hospitals and caregivers
They have ZERO to do with designing, selling or choosing the plans.
But when you can't pay, they are the ones that become the bill collectors we hate. The ones that put millions into default and bankruptcy,
DESPITE HAVING NO SAY in the plans and deductibles we all choose.
That is one fucked up system that needs to be redesigned.
Next time I'll tell you how insurance companies decide not to pay what they contractually owe to the hospitals and use delay tactics like denials, they know they will approve , just to earn interest on premiums.
And the hospitals aren't innocent. But I'll let them off the hook for now because they have to take anyone that walks in the doors
@BillAckman@elonmusk@DOGE@RobertKennedyJr@DrOz
I asked Grok: Why is EHR dysfunctional?
This affects every citizen in America.
"EHRs (Electronic Health Records) being dysfunctional boils down to a few key culprits that keep them from working as smoothly as they should. It’s less about outright failure and more about systems that limp along, frustrating everyone involved.
Start with design. Many EHRs were built with administrators and insurers in mind—think coding for reimbursement or meeting regulatory checkboxes—rather than the doctors and nurses actually using them. The result? Interfaces that feel like a maze. Clinicians waste time wrestling with dropdowns, pop-ups, and endless scrolling instead of focusing on patients. Research, like a 2023 study from Annals of Internal Medicine, found docs spend about 35% of their day on EHR tasks, often on stuff that doesn’t directly help care.
Next, they don’t talk to each other. Interoperability is a buzzword, but in reality, different EHR platforms—like Epic or Cerner—hoard data like jealous dragons. A patient’s history might be split across systems that don’t sync, forcing providers to hunt down faxes or PDFs. The tech exists to fix this, but vendors and hospitals drag their feet—why share when you can lock in customers?
Cost adds to the dysfunction. These systems demand hefty upfront investments and constant maintenance. Smaller clinics get crushed under the weight—sometimes spending $50,000 to $100,000 just to get started, per a 2024 Health IT Analytics piece. And for that price, you’d expect perfection, not sluggish software or downtime during updates.
Human error amplifies it. Training’s often rushed or skimped on, so staff fumble through features they don’t understand. Meanwhile, patients feel the disconnect—doctors glued to screens instead of listening. Worse, bad design can hide critical info, leading to mistakes like wrong meds or missed allergies. Exact stats on this are murky because companies shield error reports, but anecdotal cases pop up too often.
It’s not useless—EHRs have streamlined some things, like e-prescriptions—but the dysfunction comes from a system prioritizing compliance over care, profit over integration, and hype over usability. What’s your angle on this—dealing with it firsthand?