And today @JAMA_current Mazdutide, also a GLP-1 and glucagon dual receptor agonist with similar body weight loss as Survodutide https://t.co/BLLVmXgUp8
The tide is coming in. High tide of the X-tides, that is in the new GLP-1 family of peptide drugs. Today @NEJM survodutide, a GLP-1 and glucagon dual receptor agonist (no GIP, like tirzepatide) drug that achieved ~16% body weight loss at 2 different doses cf placebo
https://t.co/lHCy7iLUCn
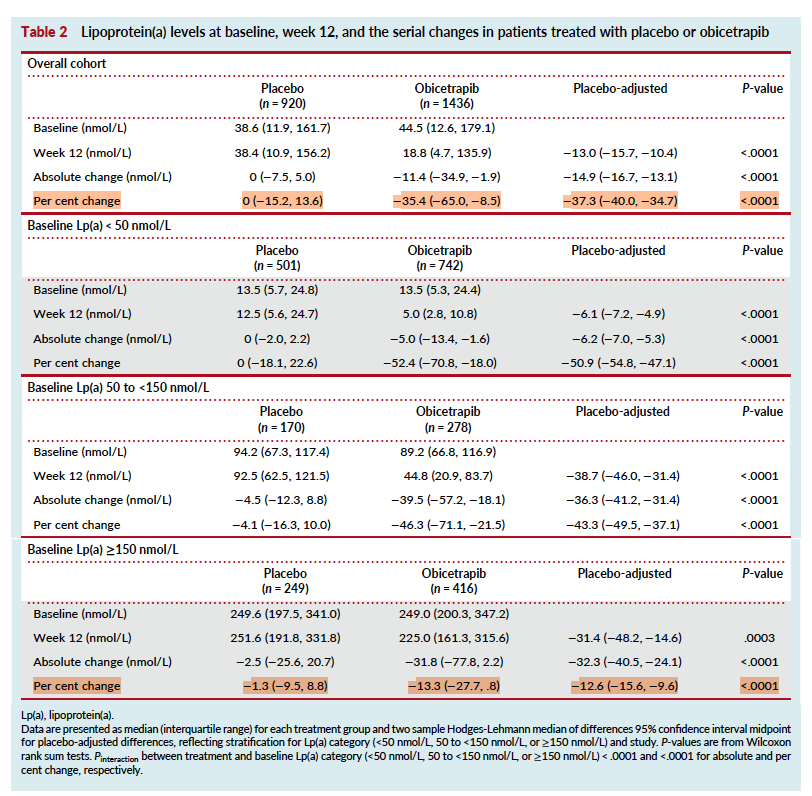
Interesting obicetrapib/Lp(a) signal: like PCSK9i, the % reduction appears smaller at higher baseline Lp(a). But the absolute reduction is fairly similar once Lp(a) is elevated (~32–36 nmol/L), suggesting a possible “ceiling” in absolute lowering. Mechanism remains unclear. This would be a good nidus for an NIH R01 grant @Philip_Gordts It will also be interesting to see what absolute reduction on Lp(a) may be associated with benefit in Lp(a) HORIZON. https://t.co/l330tDYJGJ
Our indie game:
- handcrafted pixel art, made one tiny detail at a time 💜
- cosy farming, fishing, cooking, and crafting 🧑🌾
- build your home wall by wall 🏗️
- customise your character & shape relationships with NPCs 🫶
- rebuild a village shaped by the Frostfalls 🌠
- meet villagers with stories of their own 👪
- uncover the mystery of the Second Moon 🌕
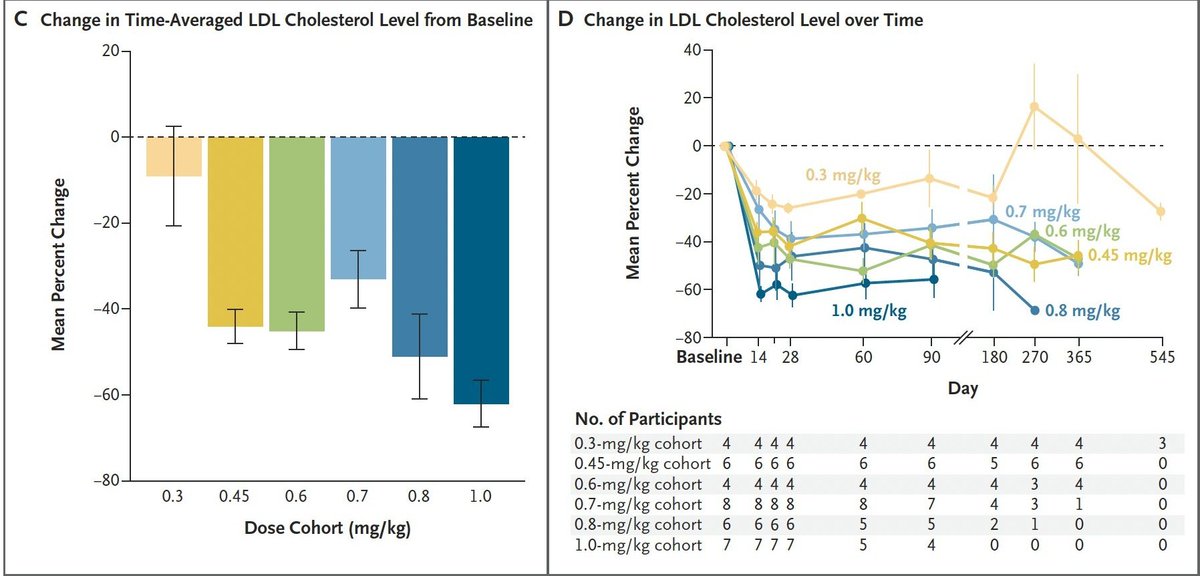
Stellar data from first-ever epigenome editing clinical trial by @tunetx_news [$COI: I own equity as a co-founder]. Invented at Sangamo by yours truly and colleagues in 2001, reduced to clinical practice 2026.
"It's been a long time coming | but now it's here" (Springsteen).
My latest article is about how the longevity movement should not be about wellness tips and tricks and lifestyle improvements, but rather, true, biotech-enabled life extension and life improvement.
We should be able to live exciting lives, without restriction. Forever.
Why ApoB Deserve More Clinical Attention
• New study followed 378 very young ACS survivors (≤40 years) for a median of 8 years
• Every 10 mg/dL increase in ApoB increased MACE risk by 8.2%
• ApoB ≥130 mg/dL was associated with a 2.5× higher risk of recurrent events
• ApoB outperformed LDL-C and non-HDL-C in predicting future cardiovascular events
@DrNadolsky@DrKarlNadolsky@NutritionMadeS3@drmatthewnagra@MichaelAlbertMD@maciejbanach
People whose genes give them a lifelong dose of statins tend to have
- Lower risk of vascular and unspecified dementia
- Lower risk of heart disease
- No difference in the risk of Alzheimer's
In other words, they're better off!
What about one-and-done Lp(a)-targeting?
CRISPR Therapeutics have human data on this: >70% Lp(a)-lowering, by targeting the LPA gene
Editas' data (below) are from monkeys: a whopping >90% Lp(a) reduction – via an unusual mechanism, LDLR upregulation!
Lilly (Verve) and Scribe also have pre-clinical programs
By the way, Lilly's is not the only one-and-done cholesterol-lowering therapy in development
To name a few others:
1. CRISPR Therapeutics (ANGPTL3 CRISPR)
2. YolTech (PCSK9 base editing)
3. Scribe (PCSK9 epigenetic silencing)
4. Editas (LDLR CRISPR upregulation)
5. Epigenic (PCSK9 epigenetic silencing)
Eli Lilly has done it.
They've gone and made what seems to be a powerful, permanent gene therapy for LDL cholesterol.
That means they'll be able to effectively prevent most heart disease with a single infusion!
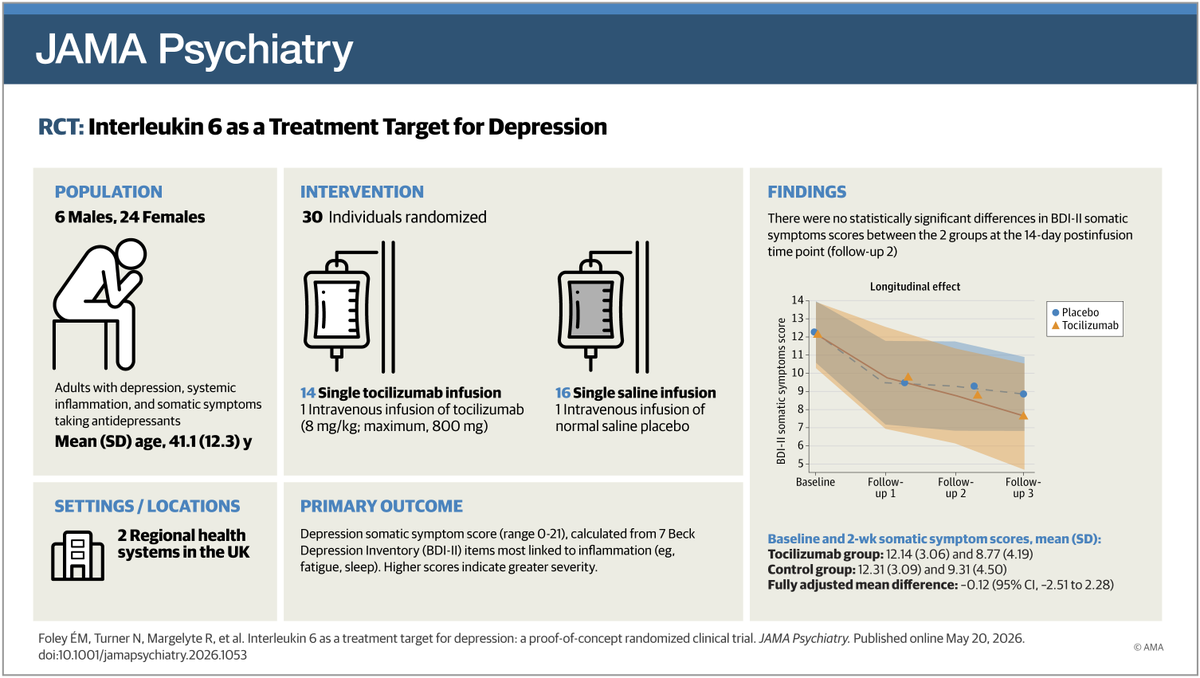
🚨 A new RCT just tested an IL-6 monoclonal antibody for difficult-to-treat depression.
It’s the first direct test of IL-6 receptor blockade in psych.
Remember: the new DSM is considering an inflammatory subtype of depression.
But did it actually work? 🧵
reminder
BIG BREAKTHROUGH: Scientists have discovered a protein called SHP (NR0B2) that could potentially slow or even stop osteoarthritis instead of just treating the pain.
The researchers found that SHP blocks a major inflammatory pathway known as IKKβ/NF-κB, which normally triggers cartilage destroying enzymes like MMP-13 and ADAMTS5.
In patients with osteoarthritis, SHP levels were found to be much lower in damaged cartilage.
And when scientists removed the protein in mice, the joints deteriorated faster, with more inflammation and severe cartilage damage.
The team then used AAV-based gene therapy to restore SHP inside knee joints, significantly reducing cartilage degeneration and slowing osteoarthritis progression in animal models.
Current osteoarthritis treatments mostly focus on reducing pain after the damage is already done.
But this approach targets the actual biological mechanism driving the disease itself.
🚨 5000 milligram-years of LDL exposure is the threshold where cardiovascular risk stops being theoretical and starts being structural.
Your arteries remember every year of high cholesterol.
The damage accumulates long before your first symptom appears.
And no, a "normal" cholesterol reading at age 45 does not erase 25 years of silent injury.
I am a cardiologist.
I have seen patients with LDL of 130 mg/dL for 40 years walk into my office thinking they are fine.
They are not fine. Their cumulative exposure tells a completely different story.
🔬 Here is what the science actually says.
Milligram-years are calculated by multiplying your average LDL level by the number of years you carried it.
LDL of 100 mg/dL for 50 years equals 5000 milligram-years.
LDL of 160 mg/dL for 31 years also equals 5000 milligram-years.
The math is unforgiving either way.
💓 At 5000 milligram-years, atherosclerotic plaque is not forming. It has already formed.
The question is no longer whether you have plaque. The question is how much, and whether it is stable or vulnerable.
Mendelian randomization studies show that lifelong LDL exposure drives cardiovascular risk in a dose-dependent, time-dependent relationship that late intervention cannot fully reverse.
✅ JUPITER (rosuvastatin): major cardiovascular events reduced 44% in patients with elevated CRP and LDL under 130 mg/dL. The benefit came from early, aggressive lowering.
✅ FOURIER (evolocumab): cardiovascular death, heart attack, and stroke reduced 15% on top of statin therapy. The patients who benefited most were those with the longest prior exposure histories.
✅ ORION-1 (inclisiran): LDL lowered 51% with twice-yearly dosing. Designed precisely for patients who need sustained, long-term reduction to stop cumulative damage from compounding.
🔬 Why cumulative exposure matters more than a single reading:
Endothelial injury begins at LDL levels above 70 mg/dL
Oxidized LDL penetrates arterial walls and triggers inflammatory cascades
Foam cell formation and fibrous cap development happen silently over decades
A coronary calcium score of zero at age 40 does not mean you have escaped. It means the clock is still running.
⚠️ The patients I worry about most are not the ones with LDL of 200 mg/dL at age 60.
They are the ones with LDL of 115 mg/dL since age 25 who never started treatment because no single number ever crossed a guideline threshold.
🩺 A patient who starts statin therapy at age 35 with LDL of 130 mg/dL and reduces it to 65 mg/dL cuts their lifetime milligram-year burden nearly in half by age 65.
A patient who waits until age 55 to start treatment has already accumulated 3575 milligram-years of irreversible arterial exposure.
That is the difference between prevention and damage control.
❌ Supplements will not reduce your milligram-year burden.
❌ Eating clean after decades of high LDL will not remodel calcified plaque.
❌ Feeling healthy is not a biomarker.
The tools with the strongest data are unsexy, free, and require your participation.
Know your LDL. Know your age. Do the math.
❤️ Bottom line:
Cardiovascular risk is not a snapshot. It is a cumulative calculation.
5000 milligram-years is not a scare tactic. It is a structural threshold supported by genetics research, imaging data, and outcomes trials enrolling hundreds of thousands of patients.
Get your LDL tested now regardless of your age.
Calculate your exposure. Multiply your average LDL by your years of adult life.
If you are approaching or past 5000 milligram-years, talk to your cardiologist about aggressive reduction targets, not guideline minimums.
Start early. The arteries you protect in your 30s and 40s are the ones that keep you out of my cath lab in your 60s.
What is your LDL, and how long have you been carrying it?
#Cardiology #HeartDisease #HeartHealth #CardiovascularHealth #LDLCholesterol #ApoB #Atherosclerosis #StatinTherapy #PreventiveCardiology #MetabolicHealth






























![UrnovFyodor's tweet photo. Stellar data from first-ever epigenome editing clinical trial by @tunetx_news [$COI: I own equity as a co-founder]. Invented at Sangamo by yours truly and colleagues in 2001, reduced to clinical practice 2026.
"It's been a long time coming | but now it's here" (Springsteen). https://t.co/Nm7Y0dnvIC](https://pbs.twimg.com/media/HJqiiDOacAArETa.jpg)