Published today, Defining Cardiovascular Endpoints in Oncology Trials: Challenges and Opportunities A Scientific Statement from the American Heart Association.
This figure provides a flexible, nonprescriptive framework for evaluating cardiovascular (CV) safety across early- and late-phase oncology trials.
This framework balances patient safety, trial feasibility, and cost, while ensuring standardization where supported by evidence.
✍🏼 @AnaBaracCardio@avirupguha@MarcBonaca@anita_deswal@LalehAmiri@DrRaulCordoba@DrAlexAdjei
Vitamin B3 nicotinamide has dual cardiac effects: low doses protect, high or chronic doses cause arrhythmia. @hu_liangyu@DeliZhang2 https://t.co/JqnmDgNvuB
ICYMI in #JACCHF: A prespecified subanalysis of the FINEARTS-HF trial evaluating the efficacy and safety of finerenone in patients with mildly reduced and preserved EF via a kidney function-based dosing strategy https://t.co/xkafxqb7E8
#HFmrEF#HFpEF#LVEF
This statement outlines a standardized framework for CV endpoints, including clear definitions, adjudication, baseline testing, surveillance, and the use of biomarkers and patient-reported outcomes.
Its broader aim is to make oncology trials more consistent, clinically relevant, and regulator-ready, while strengthening collaboration between oncology and cardiology to better assess net clinical benefit.
✍🏼 @AnaBaracCardio@avirupguha@MarcBonaca@anita_deswal@LalehAmiri@DrRaulCordoba@DrAlexAdjei
Fisiología Cardíaca & Bucle Presión-Volumen. 🫀💥
🔷️El bucle PV ventricular describe los cambios temporales en el volumen de la cavidad (eje x) y la presión (eje y) que ocurren a lo largo del ciclo cardíaco. 📈🔣
🔷️Un ciclo cardíaco normal en un bucle PV está típicamente delimitado por 4 bordes: 1) llenado ventricular en la parte inferior; 2) contracción isovolumétrica en el lado derecho; 3) eyección ventricular en la parte superior; 4) relajación isovolumétrica en el lado izquierdo. 🤔🔎
🔷️El área encerrada entre el ESPVR (relación PV telesistólica), el EDPVR (relación PV telediastólica) y la línea de relajación isovolumétrica junto con el área del bucle PV se conoce como Área de Presión-Volumen (PVA), que se aproximan a la energía mecánica total producida por el VI (el PVA tiene correlación altamente lineal con el MVO²). 📉❤️🔥
🔷️Los cambios en la precarga y la poscarga provocarán un desplazamiento diagonal de bucle PV hacia la izquierda o la derecha, hacia arriba o abajo. Entonces, el análisis del bucle PV proporciona una herramienta para comprender mejor las alteraciones hemodinámicas subyacentes y permite adaptar una terapia adecuada. ✍️🏻🧐
📄🆓️⤵️
https://t.co/WsQAEQ1gFK
https://t.co/y2Q98H03sa
📢Nueva evidencia en Nature Metabolism: cada +5 kg/m² de IMC se asocia a mayor riesgo de algunos tipos de cáncer, especialmente endometrio (+58%) y adenocarcinoma esofágico (+47%)⚖️
Eso sí: para la mayoría de cánceres, la asociación parece modesta o nula
https://t.co/Cic3x2jCDd
There are 19 types of cancer associated with obesity. But only a limited number have a very strong association. Two excellent review papers today @NatMetabolism
https://t.co/y1M5b9dtQd
https://t.co/YOlQ3PtRSC
Now online: the latest issue of EuroIntervention, including:
- ESC Clinical Consensus Statement on DAPT after ACS,
- Door-to-unload time in STEMI-CS,
- M-TEER and left atrial pressure,
- Temporal trends in mitral intervention,
- Transcatheter papillary muscle banding,
and more.
🔗https://t.co/Zpd59xzSLB
@BenediktKoell@DanielKalbacher@BenediktSchrage
#cardiotwitter #interventionalcardiology #cardioEd
🫀📊 **Diastolic dysfunction: are we finally making it simpler?**
Assessing left ventricular diastolic function remains one of the most challenging areas in echocardiography. Multiple variables, load dependence, age-related changes, and often discordant findings make interpretation difficult even for experienced imagers.
A new review proposes a **simplified, tier-based approach** aligned with the 2025 ASE recommendations, aiming to improve the clinical applicability of diastolic function assessment.
🔑 **Key concepts**
✅ Diastolic dysfunction should not be viewed as a single measurement but as a combination of:
• Impaired LV relaxation
• Increased myocardial stiffness
• Elevated filling pressures.
📈 The 2025 approach starts with what may be the most clinically useful marker:
👉 **e′ velocity**, reflecting myocardial relaxation.
Additional markers such as:
• E/e′ ratio
• Left atrial size and function
• Left ventricular hypertrophy
• Left atrial reservoir strain (LARS)
are then integrated in a stepwise fashion.
💡 One of the major advances is the introduction of a **tiered framework** for estimating filling pressures, reducing the number of "indeterminate" studies that frequently complicated the 2016 algorithm.
🏃 In patients with unexplained exertional dyspnoea, the paper reinforces the value of **diastolic stress echocardiography**, recognising that elevated filling pressures often become apparent only during exercise.
🤖 Perhaps the most exciting perspective is the role of artificial intelligence.
The authors propose that diastolic dysfunction may be better understood as a **latent phenotype**, integrating dozens of clinical and imaging variables rather than relying on a few Doppler measurements alone.
Machine-learning models have already demonstrated:
✅ Improved estimation of filling pressures
✅ Better prognostic stratification
✅ Identification of high-risk phenogroups that traditional algorithms may miss.
🎯 **Take-home message**
Diastolic dysfunction is not a binary diagnosis.
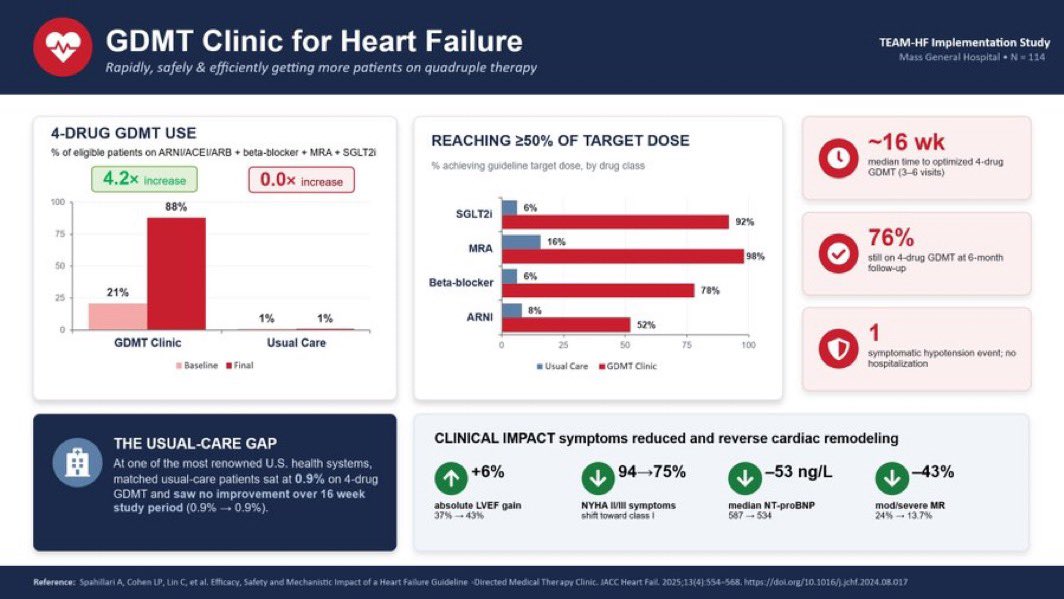
The GDMT Clinic model is a game-changer for #HeartFailure management.
In the TEAM-HF Implementation Study (MGH, N=114):
✅ 4-drug GDMT use: 21% → 88% (+4.2×)
✅ SGLT2i at target dose: 6% → 92%
✅ MRA at target dose: 16% → 98%
⏱️ Achieved in just ~16 weeks
🏃♀️ ¿Y si el ejercicio fuera algo más que control metabólico en la DM1?
Nueva revisión en @DiabetesCareADA sobre inmunomodulación inducida por ejercicio en diabetes tipo 1:
🔬 En modelos preclínicos, el entrenamiento aeróbico y el HIIT reducen la insulitis (~50% en ratón NOD), protegen la célula β del daño por citoquinas e inducen exerquinas antiinflamatorias
👶 En humanos: mayor actividad física → menor progresión de la autoinmunidad en niños con autoanticuerpos, luna de miel más larga y patrón citoquinas antiinflamatorias (↑IL-10, ↓TNF-α).
https://t.co/7X53gM2WNA
Supplementation with #Menaquinone7 for 2 years modestly slowed progression of #CoronaryArteryCalcification in patients with coronary artery disease, with no major adverse effects.
https://t.co/HsBLIlRO0W
🚨 Can serial CMR redefine risk stratification in HCM?
A new study suggests that it may not be the amount of fibrosis alone that matters—but how quickly fibrosis progresses over time.
Researchers followed 313 patients with hypertrophic cardiomyopathy (HCM) who underwent two CMR scans approximately 4 years apart, assessing changes in late gadolinium enhancement (LGE), a marker of myocardial fibrosis.
🔍 Key findings
📈 Myocardial fibrosis increased substantially over time:
Median LGE mass increased from 2.9 g to 8.3 g
LGE prevalence rose from 72% to 91%
Extensive fibrosis (LGE ≥15%) doubled from 7% to 15% of patients.
⚠️ Nearly 70% of patients without LGE at baseline developed fibrosis on follow-up CMR.
💡 The most important finding was the rate of fibrosis progression:
ΔLGE >1.5 g/year independently predicted adverse clinical outcomes
Patients with rapid fibrosis progression had more than a twofold increased risk of death, transplant, HF hospitalization, stroke, or aborted sudden cardiac death
Adding ΔLGE/year to conventional risk models significantly improved risk prediction and reclassification.
❤️ For hard endpoints (death, transplant, aborted SCD), a fibrosis progression rate of >3.75 g/year identified particularly high-risk patients.
🎯 Clinical implications
Current guidelines already recommend repeat CMR every 3–5 years in HCM. This study provides strong support for that recommendation and suggests that:
✅ Serial CMR should be viewed as a dynamic monitoring tool rather than a one-time assessment
✅ Fibrosis progression may identify high-risk patients who appear low-risk according to conventional risk scores
✅ Imaging intervals could potentially be personalised based on fibrosis progression rates.
📚 One particularly striking observation: patients considered "low risk" by traditional ESC or AHA/ACC criteria but showing rapid LGE progression often had worse outcomes than some patients classified as high risk with stable fibrosis.
🧬 The future of HCM risk stratification may therefore move beyond a static fibrosis threshold toward a dynamic assessment of myocardial fibrosis progression.
Ejercicio & prueba de esfuerzo en el Sx de Brugada. 🏃♂️🫀⚡️
🔹 El momento clave no es el ejercicio, sino la recuperación. Solo ~1% de los pacientes desarrolla patrón tipo 1 durante el esfuerzo, mientras que hasta 25.5% lo manifiesta en la fase de recuperación, cuando ocurre el rebote vagal tras el retiro del estímulo simpático. 🤔🏃♂️⏱️
🔹 La recuperación temprana (primeros 2-3 minutos) es la ventana más importante. Es aquí donde pueden aparecer el patrón tipo 1 de Brugada, elevación del ST/J-point, extrasístoles ventriculares, TV o FV en pacientes de alto riesgo. 🧐⚠️⚡️
🔹 Se asociaron con mayor riesgo de eventos arrítmicos: Aumento del ST durante la recuperación, extrasístoles ventriculares entre 1.5 y 3 minutos de recuperación, recuperación rápida de la FC (marcador de hiperactividad vagal), prolongación de la pendiente ascendente de la onda S en ejercicio máximo. 👨⚕️📝
📄🆓️⤵️ State-Of-The-Art Review 2026 @JACCJournals 👌🏻💯
https://t.co/pKL8FJz2HZ
https://t.co/4PnV0aMMfn
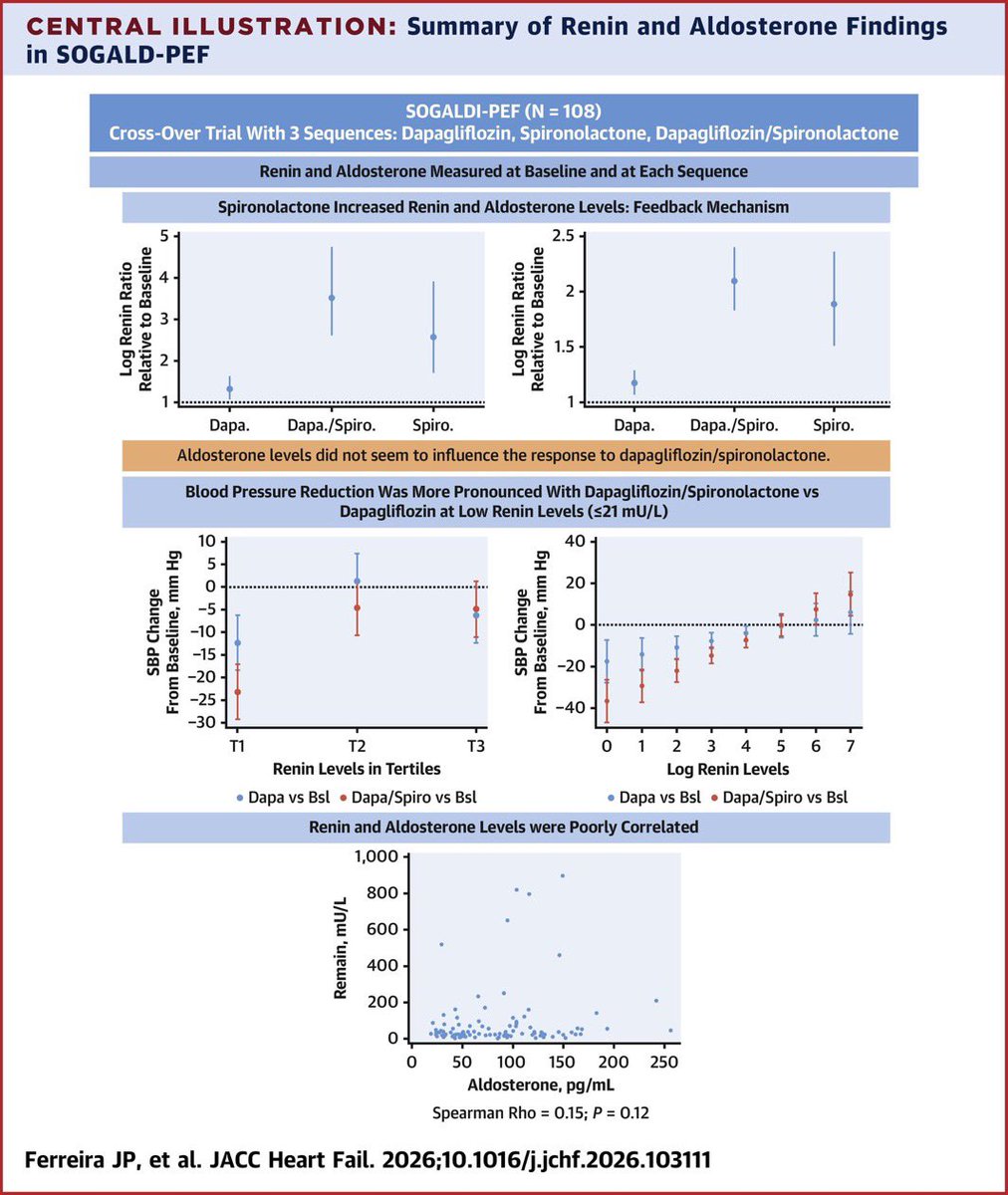
In HFpEF, measure renin before choosing between SGLT2i alone vs SGLT2i + spironolactone combination. Low renin patients benefit most from combo.
Spironolactone activates RAAS feedback loop
Low renin better response to the combination
Renin and aldosterone are poorly correlated
Prospective multicentre single-arm study of an interatrial shunt in heart failure with reduced ejection fraction (SUSTAIN-HF): 1-year clinical and haemodynamic outcomes https://t.co/Eq9o1f1BAM
#Consenso de la Sociedad Interamericana de Cardiología sobre la prevención cardiovascular en el paciente con diabetes mellitus tipo 2 en América Latina y el Caribe.
Un llamado para una estratificación de riesgo más temprana, protección cardiorrenal agresiva y acceso equitativo a terapias basadas en evidencia.
https://t.co/KyNa031T4z
👉Vía: Dra. @MaximaMendez15
New RCT data on nudge letters for CKD management
Patient-facing nudge letters had minimal impact on RASi/SGLT2i prescribing in CKD patients — but did significantly increase GP visits (absolute difference +1.39%, 95% CI 0.17–2.61).
#Nephrology#CKD
Patients w/ low plasma renin levels had a more pronounced BP reduction w/ spironolactone/dapagliflozin vs dapagliflozin alone, along w/ improved CV structure & function. Aldosterone levels exhibited no predictive value in treatment response. https://t.co/U1jK7MQYvd #JACCHF#HFpEF