Vena de Marshall. 🫀⚡️
🔶️La vena de Marshall es un remanente de la vena cardinal izquierda embrionaria que discurre entre la orejuela izquierda y las venas pulmonares izquierdas.
🔶️Lo importante es lo que contiene:
⚡ Fascículo de Marshall (tejido muscular arritmogénico).
⚡ Plexos autonómicos simpáticos y parasimpáticos.
⚡ Conexiones epicárdicas protegidas por grasa.
🔶️Por ello participa en los 3 pilares para generar FA:
🔸️Trigger: genera extrasístoles que inician FA.
🔸️Sustrato: favorece circuitos de reentrada y gaps epicárdicos.
🔸️Modulación autonómica: la estimulación de sus plexos puede inducir FA.
🔶️ La vena de Marshall no es un simple vestigio embrionario; es una estructura neuro-muscular capaz de iniciar, mantener y perpetuar la FA. Por eso se ha convertido en un objetivo terapéutico clave en la ablación moderna de la FA persistente (la infusión con etanol surge como nueva opción). 🫀⚡
📄🆓️⤵️ State-Of-The-Art Review 2026 @JACCJournals 💯👌🏻
https://t.co/wRtVPFbmZ6
https://t.co/qWJKrnsDI0
Right Atrium-to-Left Ventricle Access Guided by Computed Tomography Merged with 3D Mapping for VT Ablation in a Patient with Mechanical Aortic and Mitral Valves
@veramasloo@evgeny_lyan@CKuehl2015
https://t.co/8W1TxoTbyY
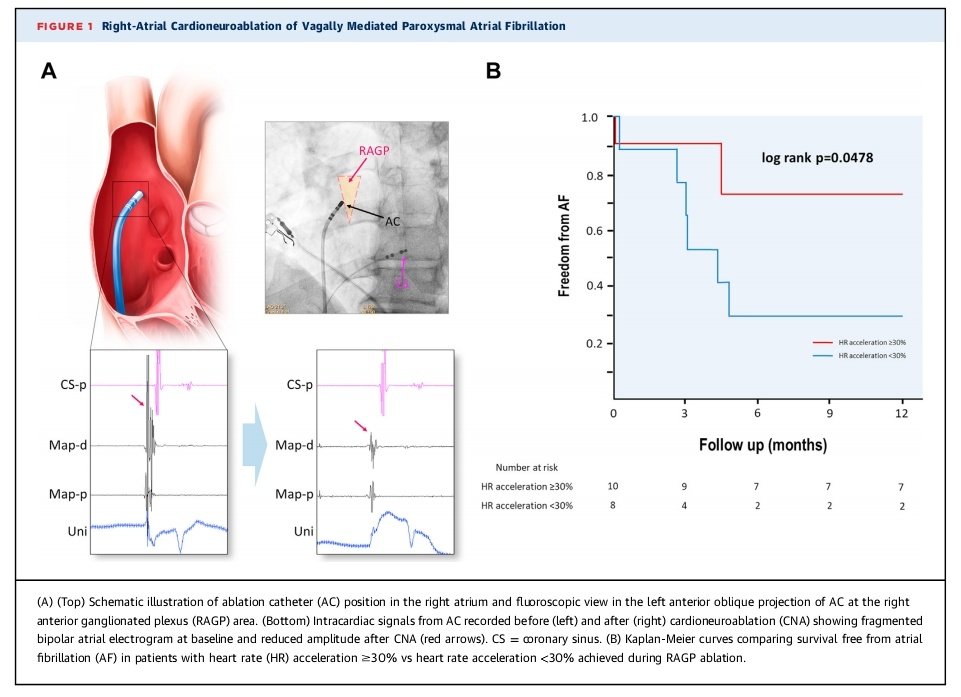
Some patients with vagally mediated AF can benefit most from cardioneuroablative effect and may not need full PVI
Some of them may not even require any ablation in the left atrium
Check out our @JACCJournals paper using shareable link (before it expires) https://t.co/YCLRdvs9HR
See my comment in the subthread.
In patients with RBBB, narrowing of the S-wave in lead I with an S/QRS ratio<0.56 is associated with increased need for PPM, even after adjusting for QRSd.
https://t.co/N3KqeqMhvx
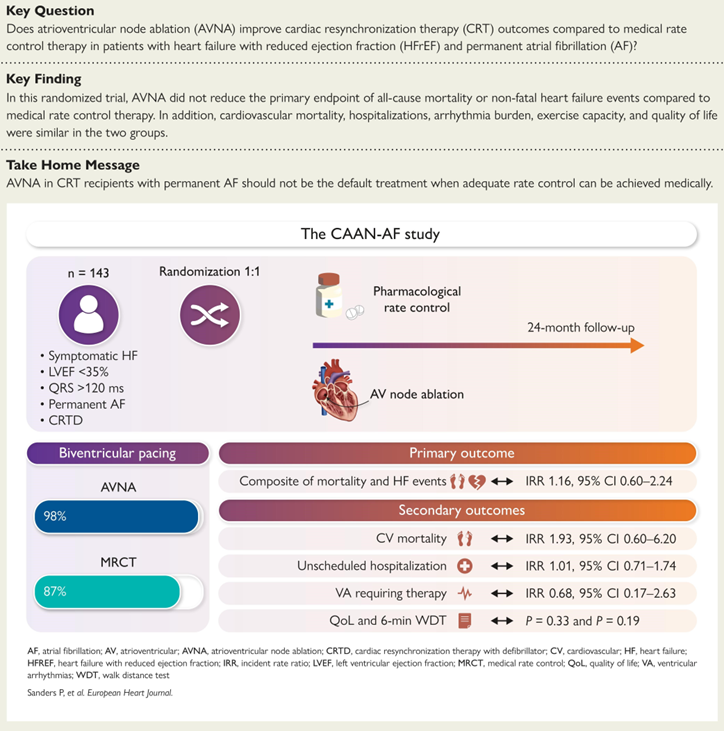
CAAN-AF Trial #CHRD@adelaide87018
Our previous meta-analysis of observational studies suggested CRT patients with AF had a significant 58% reduction in all-cause mortality with AV node ablation - https://t.co/rLbkUhqZLX
We designed the CAAN AF Trial supported by the @nhmrc and critical industry partners - in order of support @bostonsci@AbbottNews@Medtronic@MicroPort - Methodology paper - https://t.co/kZrLVV9G9q
CAAN AF Trial: https://t.co/bMIaH2CPHV
RCT showing no benefit in the routine use of AV node ablation
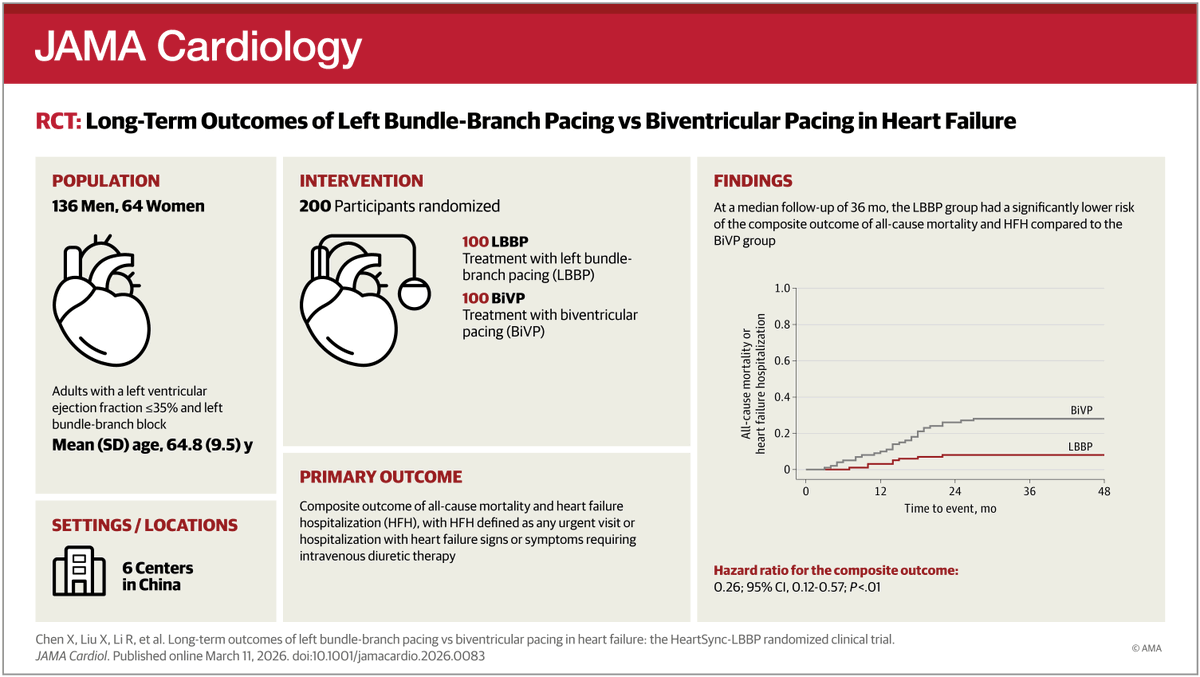
In patients with #HeartFailure and #LBBB, conduction system pacing (#CSP) was inferior to biventricular pacing (#BiVP) for a composite of death, heart failure events, and LVEF change at 12 months.
https://t.co/a3Tlkre65B
Three years ago, I was asked to speak @westernAFib on whether PFA will obviate the need for epicardial therapies. As a field, we need to collectively understand when and how often PFA is transmural and durable.
Congrats to @Innovate_JJ and team on publishing our observations with simultaneous epi mapping.
Epicardial Validation of Transmural Posterior Wall Isolation During Endocardial Pulsed Field Ablation https://t.co/a3L82cnMHy
A randomized controlled trial of pulsed field ablation vs antiarrhythmic therapy as a first-line treatment for persistent atrial fibrillation: The AVANT GUARD trial rationale and design
@ClevelandClinic@ohiohealth@UCLAHealth@MassGeneralNews#EPeeps
https://t.co/rOF6eZeRHn
Efficacy and safety of direct oral anticoagulants for intermediate stroke risk in patients with atrial fibrillation (SINGLE-AF): Study design and protocol
#EPeeps
https://t.co/iQqBD2HYaS
pECGreview: Using “Not-to-Miss” ECG diagnoses to assess competency of trainees and faculty in ECG interpretation via a weekly online ECG education program, by @Peds_ECG_Guy and colleagues
@HopkinsMedicine@JohnsHopkins#EPeeps
https://t.co/Rbvoq4J9jq
Pulsed-field vs radiofrequency ablation for posterior wall isolation in persistent atrial fibrillation: A propensity-matched outcome analysis
#EPeeps
https://t.co/irAlY1lwfR
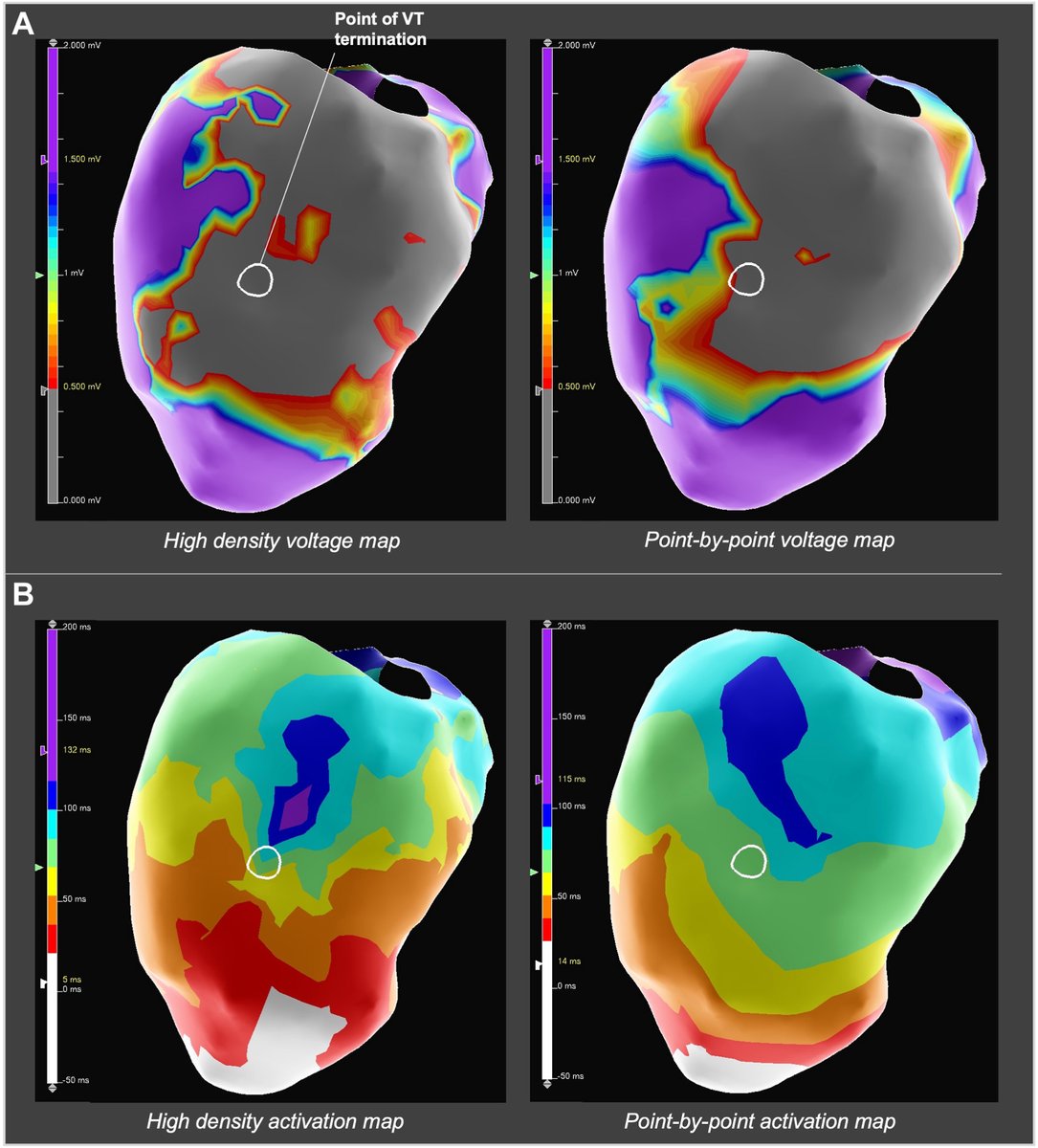
High-density vs point-by-point mapping in ventricular tachycardia ablation: A comparative analysis of substrate characterization, by @adrian_petzl and colleagues
@PennMedicine@AbbottNews@MedUnivSC#EPeeps
https://t.co/tOgo2VIKSQ
🔎 Webinar Spotlight: Imaging in PFA
In this clip, Prof Josef Kautzner explains why fluoroscopy alone is insufficient in pulsed field ablation. A 2D view misses the third dimension, particularly along the ridge between the appendage and left veins, where reconnection often occurs.
Catheter position may look acceptable on fluoro, yet lack posterior wall contact or ridge alignment. Signals and intracardiac echo reveal what fluoroscopy cannot.
This part of the New Horizons In Atrial Fibrillation series, where experts discuss optimizing imagery strategy in PFA.
This video is supported by Boston Scientfic.
#Electrophysiology #PFA #PulmonaryVeinIsolation #ArrhythmiaAcademy