UTSW Neph Class of '26| He/Him/His| Nephrology and Critical Care Fellow| Loves chess, cricket, videogames, social justice reform, anti-racism. Views my own.
@EMNerd_ Note that traditional criteria to start RRT is pH < 7.1 despite failing medical management which I consider an additional flaw in BICAR-ICU2
@EMNerd_ I completely agree with your end evaluation, and I think I can add a bit.
BICAR-ICU2 used pts with pH < 7.2 and used a pH < 7.2 as 1 of 3 criteria fulfilling dialysis initiation.
SODA-BIC enrolled pts with pH < 7.3. This probably suggests they’re not completely comparable.
@AnilMakam Additionally we should ask if pH is associated with improved CV, etc, then why is mortality unchanged? There are noted harms of bicarbonate amp or gtt clinically that are not captured in trials (low ionized calcium -> worse CV; paradoxical intracellular acidosis; fluid load)
@AnilMakam My take on this is a bit different. My take is pH really a good marker for initiation of dialysis in the acute setting? Perhaps these trials expose a flaw in RRT evaluation.
Journal Club spotlight 🌟
Great discussion led by our first-year fellow Dr. Yaseen Jumani on the LIBERATE-D trial, exploring strategies to reduce dialysis burden and rethink how we approach care for patients with acute kidney injury needing dialysis.
Really troubled by this question in a popular surgical critical care study book…
Surgical Critical Care and Emergency Surgery
Topic is early v late dialysis and so much on this topic is know and just disappointing to this question…. The keyed answer was….
@jaykoyner
🩺Shedding light on what makes us stand out.
Think you know UTSW Nephrology? Think again. Explore the Top 10 things you didn’t know about our fellowship.
We’re bringing you a countdown — sharing a different fact every day! 🚀
Starting with
🔟Training Ground for Future Leaders
🧠💥 Think you can crack the case? Join us for The Seldin Challenge!
This special Renal Grand Rounds features a complex case presentation by Dr. Kelley Harris and real-time discussion with guest Dr. Eleanor Lederer. Don't miss it!
📅 Oct. 30 | 🕛 Noon | 📍K5.600 or Zoom
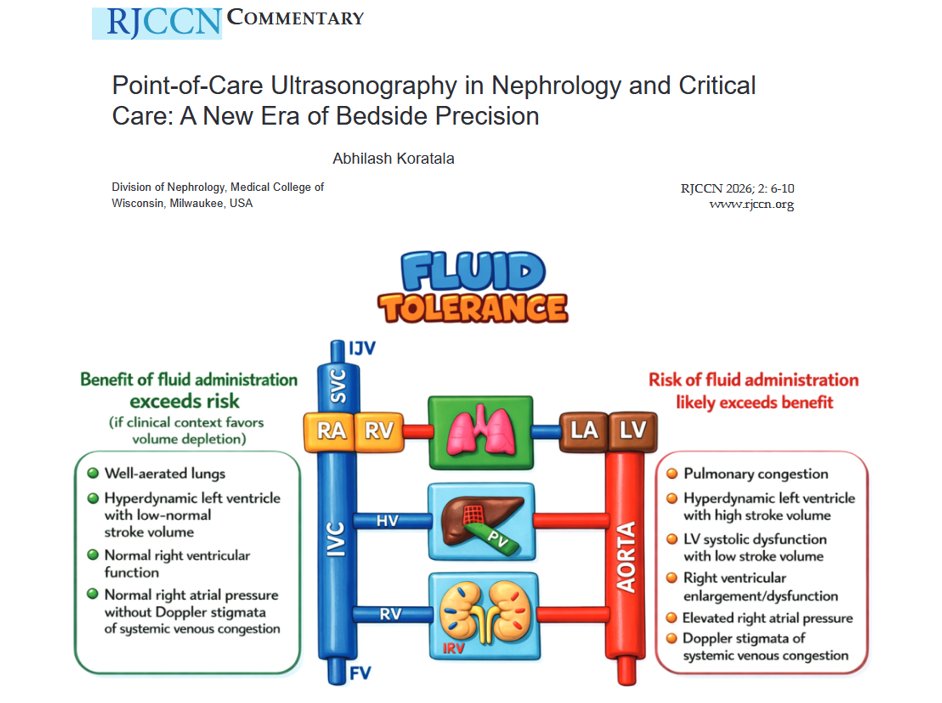
Where does the fluid go?
➡️ Excess crystalloid pools in skin, gut and lungs
➡️ Rapid ~1.3–1.5 L opens a slow-exchange third space that traps fluid
CCR Journal Watch
https://t.co/Sp06oA6IDG
1/
💡 IV fluid is the most over-prescribed drug in hospitals.
Why? Because when faced with certain problems, our reflex is always “give fluids”.
Let’s unpack the cognitive biases behind this — and why they harm patients.
🧵 What is Critical Closing Pressure — and why does it matter for perfusion?
A thread to clear up one of the most misused and misunderstood ideas in circulatory physiology.
👇
Additionally, 3g salt tabs TID is equivalent to 150 mEq of Cl. This is equal to a little less than 1/3 L of 3% NS - I would be curious of the efficacy of this.
We often rec salt tabs with diuresis in HF with hyponatremia - often met with resistance.
Awesome physiology! I wonder if it’s more accurate to state it’s a low effective arterial blood volume state with decreased filtration of chloride than a chloride deficient state as patients with heart failure are usually total body salt up.