Computational design of monomeric Fc variants with distinct pH-responsive FcRn-binding profiles
1.This study introduces computationally engineered monomeric Fc (mFc) variants with dramatically enhanced FcRn-binding affinity at acidic pH and minimal binding at neutral pH — a key requirement for extending serum half-life while avoiding lysosomal degradation.
2.The standout variant, IgG1_mFc4, binds FcRn with 30.7 nM affinity at pH 6.0 and a much weaker 6,549 nM at pH 7.4, demonstrating strong pH responsiveness with a 213-fold difference in binding — outperforming even some dimeric Fc designs.
3.The monomeric Fc variants are created by rationally disrupting Fc dimerization via substitutions like S354R and Y407R and remodeling the α2 helix for structural stability — validated via crystallography.
4.To enhance FcRn interaction, the authors introduced a designed loop near His310, a key pH-sensing residue. The best design, IgG1_mFc3, achieved 88 nM affinity at pH 6.0 while maintaining weak binding at pH 7.4 (39,150 nM).
5.Further improvements were made by targeting the His435 microenvironment with M428L and N434H substitutions. The final variant, IgG1_mFc5, reached 7.5 nM binding at pH 6.0 and 1,056 nM at pH 7.4 — ideal for efficient FcRn recycling.
6.Additional tuning using T256Y, T307L, and V308I substitutions modulated pH sensitivity by altering conformational dynamics. IgG1_mFc6 showed 44 nM affinity at pH 6.0 and 11,000 nM at pH 7.4.
7.Fc fusions, including Trastuzumab Fab or human growth hormone (hGH), did not significantly alter FcRn-binding properties, indicating design robustness and compatibility with therapeutic payloads.
8.Thermal stability of the variants remained high (Tm > 58 °C), and immunogenicity assays confirmed negligible cytokine induction, supporting their therapeutic potential.
9.The designed loop sequence serves as a versatile tuning module: minor changes in its residues yielded mFc variants with widely different FcRn affinities, opening paths for application-specific optimization.
10.Substitutions were successfully transferred into IgG4 Fc, yielding IgG4_mFc variants with FcRn-binding profiles similar to their IgG1 counterparts, suggesting broad adaptability.
11.Introducing the same FcRn-enhancing substitutions into native dimeric Fc also produced variants with stronger pH-selective FcRn binding, offering a complementary route to extend antibody half-life.
12.Compared with existing monomeric Fc variants like MFc4, the new designs showed much greater pH selectivity (up to 445-fold), higher solubility, and easier manufacturability — overcoming previous limitations.
13.Overall, this study establishes a robust design platform for monomeric Fc variants with customizable pH-responsive FcRn-binding profiles, opening new possibilities for long-acting biologics and Fc-fusion therapeutics.
📜Paper: https://t.co/sLZbfjeuUS
#ProteinEngineering #AntibodyDesign #FcRn #Biologics #ComputationalBiology #FcFusion #Pharmacokinetics
🚨 BREAKING: A drug that removes the antibodies causing paralysis - in WEEKS.
Myasthenia Gravis is a rare disease where your immune system cuts the signal between your brain and your muscles. Including the muscles that breathe.
A new class of drugs is rapidly removing the exact antibodies that cause paralysis in Myasthenia Gravis — often within weeks.
This is the FcRn revolution. 🧵
Discovery of a 14-protein biomarker that predicts lung cancer 5.6 years before it is diagnosed, even in non-smokers, and an anti-inflammatory medicine that prevents its progression. And, challenging dogma, the proteins are not coming from cancerous cells!
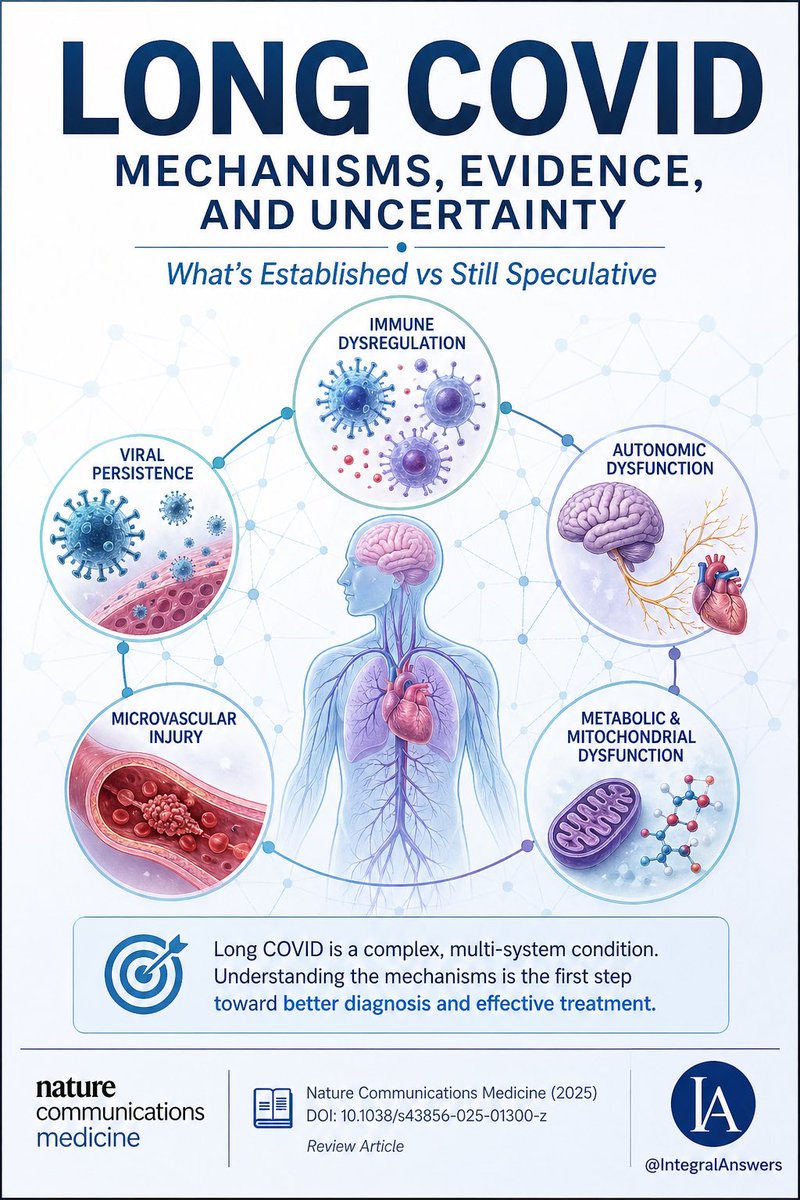
1/ Long COVID is one of the most complex post-infectious syndromes ever studied.
A new review in Nature Communications Medicine attempts to unify the biology.
Here’s what’s established, what’s emerging, and what’s still speculative. 🧵
Orexin neurons help stabilize wakefulness through orexin receptor-2 (OX2R) signaling.
When the orexin system is disrupted, sleep and wake states can become fragmented.
#OrexinSeries#SLEEP2026
Prof. Klaus Wirth proposes that a substantial subset of Long COVID—the group that clinically resembles ME/CFS—is driven by a vicious cycle involving vascular dysfunction, impaired sodium handling, calcium overload, and ultimately mitochondrial injury.
In his model, exertion does more than temporarily deplete energy reserves. Instead, exercise may trigger abnormal sodium accumulation within muscle cells. Excess sodium then promotes calcium influx, including into mitochondria. Calcium overload is a well-established mechanism of mitochondrial injury in other diseases, and Wirth argues that repeated episodes may progressively impair cellular energy production.
This hypothesis attempts to unify several observations reported in Long COVID and ME/CFS research: orthostatic intolerance, impaired cerebral blood flow, elevated lactate during exercise, post-exertional malaise (PEM), cognitive dysfunction, autonomic abnormalities, and exercise intolerance.
Importantly, this remains a hypothesis—not a proven mechanism—but it offers a biologically plausible framework linking many seemingly disconnected findings.
$VRDN - bought full stake yesterday in low $17s. Very bullish on June 30th PDUFA data given data & w both Velig (less freq IVs) and Elig (1st self-admin sub-cu form to file Q127), they're poised to be major players in underserved TED market. Eur part deal in 2H26 possible bonus.
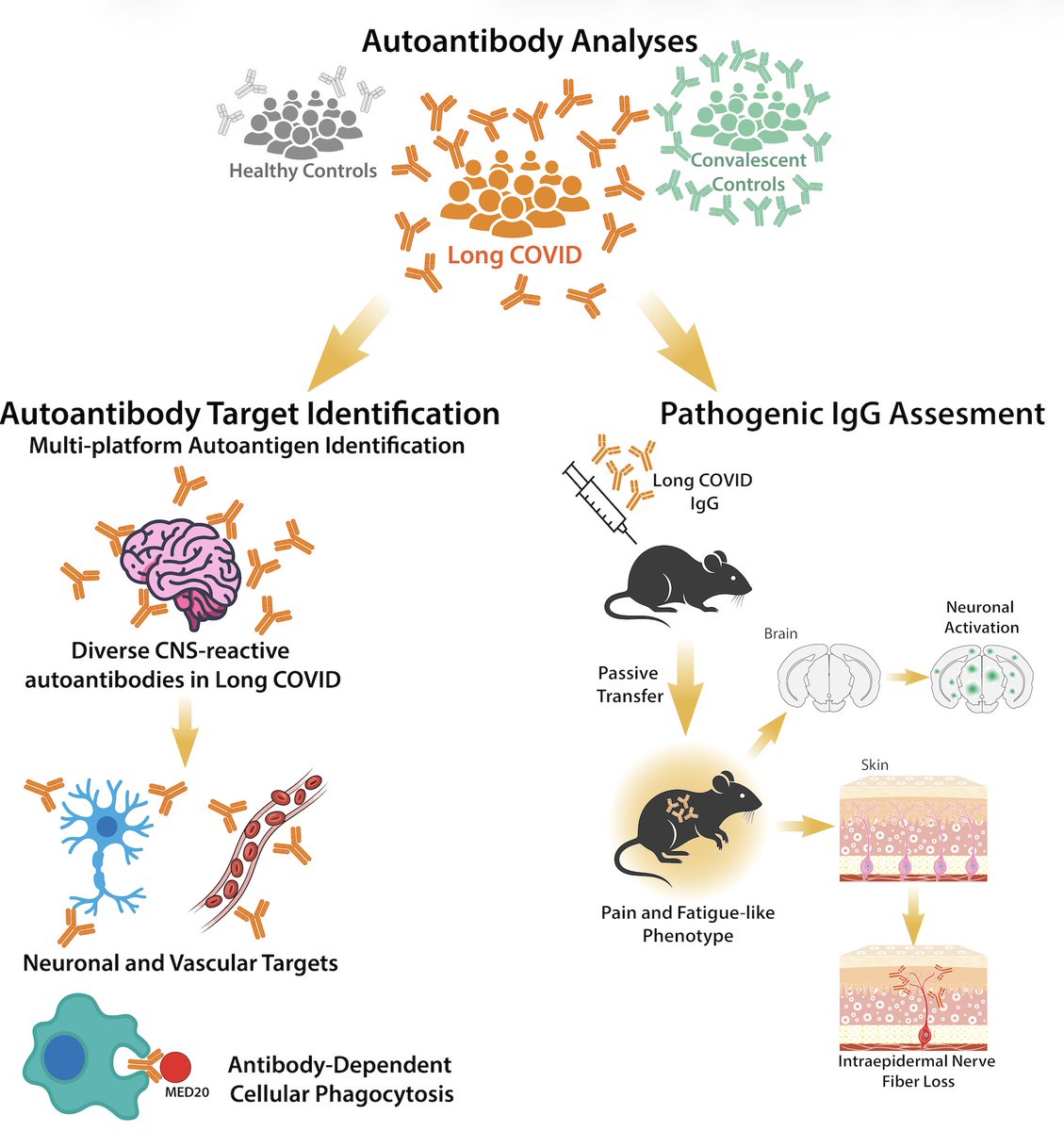
Excited to share our study by @keylas3 et al. on pathological autoantibodies in people with Long COVID. We asked whether IgG in patients with Long COVID bind to human tissues/antigens and cause pathologies when transferred into mice. With @PutrinoLab
https://t.co/tcowCufWyf
With SLEEP 2026 just around the corner, we’re sharing an educational series on the orexin system—what it does, why it matters, and how targeting this pathway may result in benefits extending beyond wakefulness.
Follow along.
#OrexinSeries#SLEEP2026
There is an assumption with vitamin D that more is better, or that one dose works for everyone. Neither is true.
The dose-response for vitamin D is curvilinear, and your starting level changes everything.
Heaney et al. (2003) gave healthy men in Nebraska 1,000, 5,500, or 11,000 IU of cholecalciferol daily through winter. Achieved serum levels at steady state were approximately 30, 60, and 84 ng/mL. Ten times the dose did not produce ten times the level. It produced about 2.8 times the level.
The body actively regulates 25(OH)D. As serum rises, hepatic hydroxylation, binding protein saturation, and catabolic clearance all increase. The curve flattens because the body is not passively accumulating vitamin D. It is throttling how much stays in circulation.
There is a second layer.
Garland et al. (2011, Anticancer Res) plotted the first derivative of that dose-response curve at different starting baselines in 3,667 adults.
At baseline 10 ng/mL, +1,000 IU/day raises serum 25(OH)D by ~11 ng/mL.
- At 30 ng/mL, ~8 ng/mL.
- At 50 ng/mL, ~5 ng/mL.
- Above 90 ng/mL, the response is nearly flat at ~1.6 ng/mL per 1,000 IU.
The same pill does dramatically different things depending on where you start.
Body composition shifts the curve further. Drincic et al. (2013) showed that in obese adults, the same 1,000, 5,000, and 10,000 IU doses produced smaller serum increments than Heaney saw in healthy-weight men. Vitamin D is fat-soluble and gets sequestered in adipose tissue. The Endocrine Society guideline acknowledges this and notes obese individuals may need two to three times the standard dose to achieve the same serum level.
The guideline landscape has shifted on what "enough" means. The IOM defines 20 ng/mL as adequate and recommends 600 to 800 IU/day. The Endocrine Society's 2011 guideline set 30 ng/mL as sufficiency. Their 2024 update walked that back. They no longer endorse specific 25(OH)D thresholds for deficiency or sufficiency, and recommend against routine 25(OH)D testing in healthy adults under 75. The evidence did not support drawing precise lines at 30 ng/mL the way the field assumed for over a decade.
If you are at 12 ng/mL, a moderate dose moves you a lot. If you are at 45 ng/mL on 5,000 IU/day, you are paying for a dose that barely moves the needle from where you already are.
The dose that works is the one matched to your starting level, your body composition, and your individual physiology. Knowing your 25(OH)D level is the input that lets you choose the dose. Without it, you are guessing.
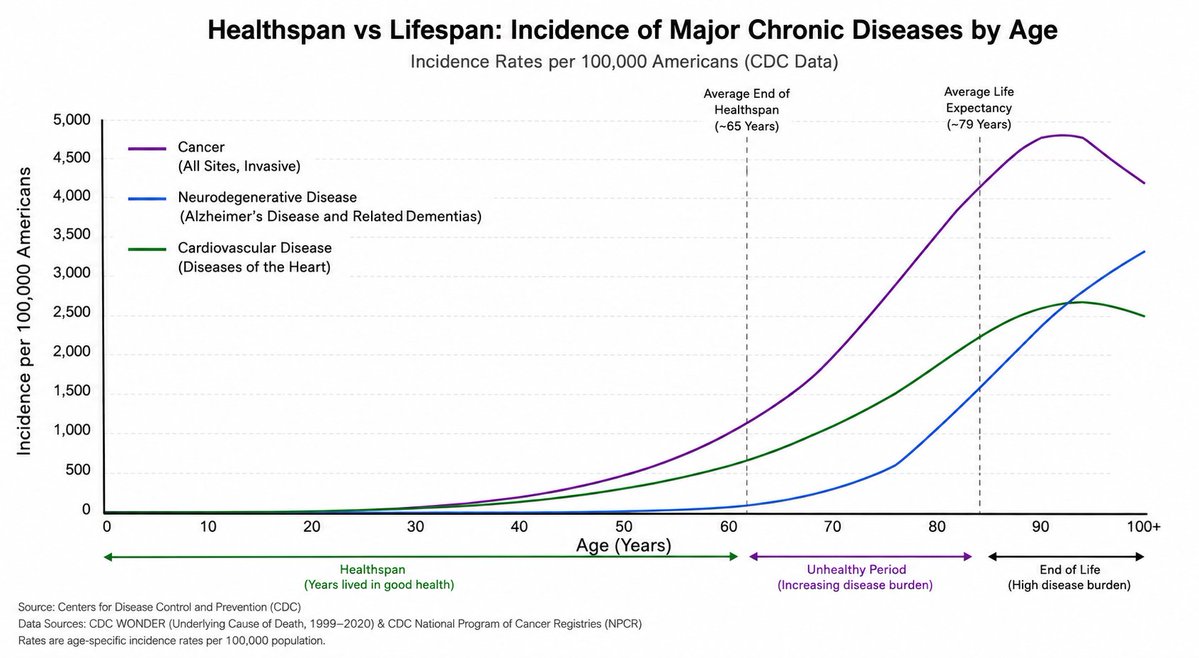
Why is there such obsession with extending lifespan when the bigger issue is that average healthspan is 65 years and there are no data (except in super-centenarians) that longer lifespan = longer healthspan (known as compression of morbidity)?
I want to give a massive shout out to Disney. Once a year when I have Make A Wish requests they let us use their parks to give the kids the greatest days of their lives. We recreate our videos in the park and Disney goes so above and beyond to make the kids happy. Very grateful🙏🏻
Big innovations that were discovered by mistake!
Nice summary by @Zlatimeyer
Can add coronary angiography by Mason Sones to the list, and many others in medicine.
Gift link https://t.co/SevqPwYdmR
📢 We’ve announced a $56 million Series C financing to support the advancement of STC‑15, our first‑in‑class, oral small‑molecule METTL3 inhibitor. The first patient has now been dosed in a Phase 2 monotherapy trial in selected sarcoma indications. https://t.co/xC77sWmabt
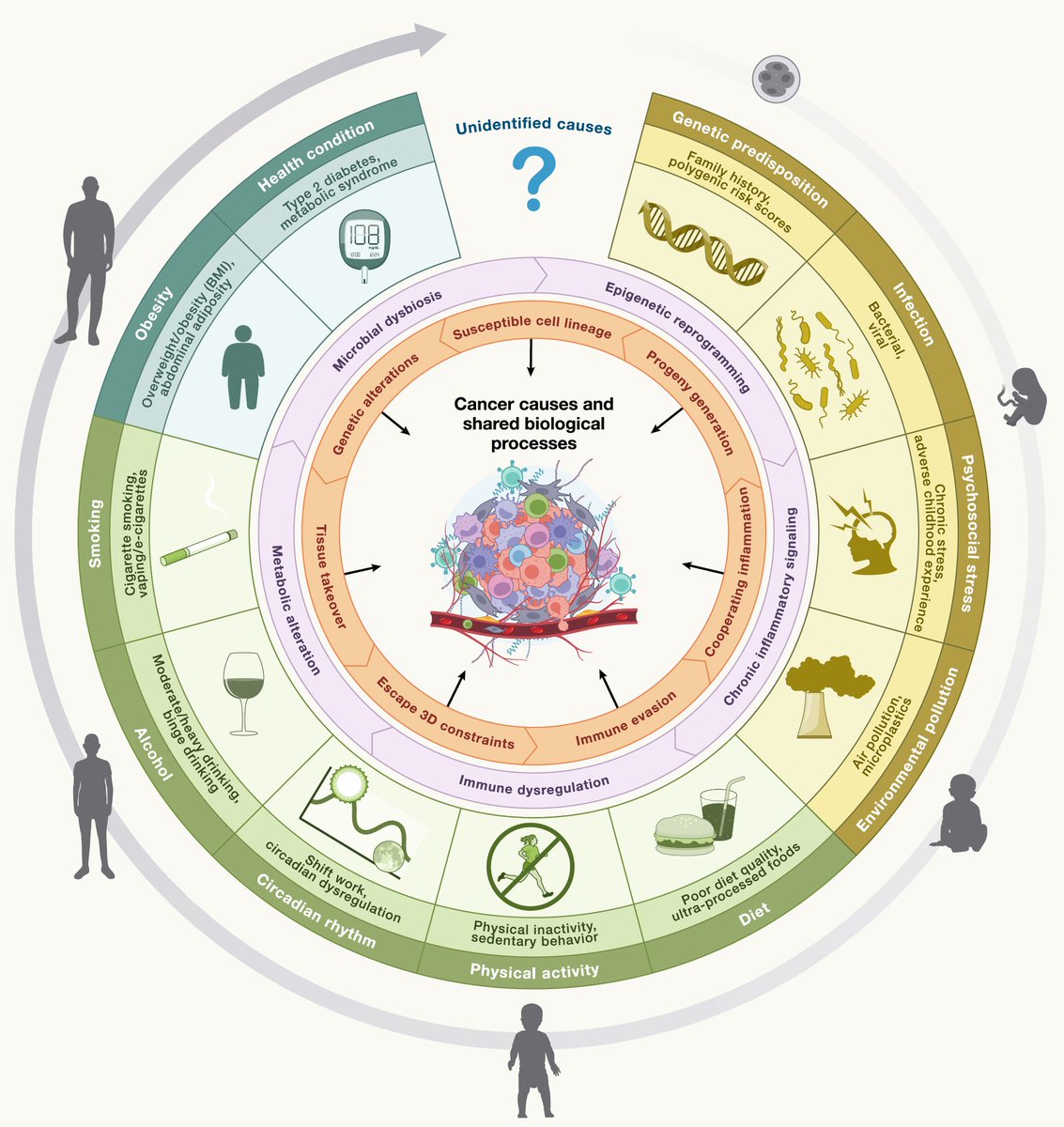
We should be prioritizing prevention of cancer instead of the major focus on detection and treatment. A new @CellCellPress perspective
https://t.co/Gkso3gGPOI