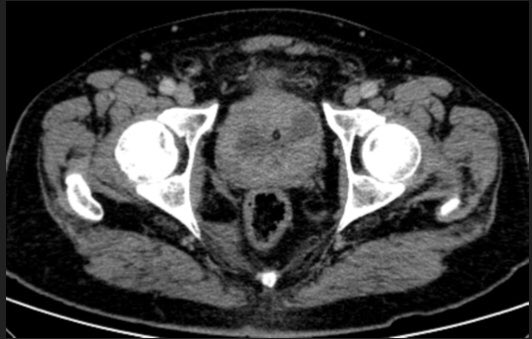
@ErickMRemer@SocietyAbdRad@adrenaldfp There are typical adenomas (homogeneous and <10 UH, probably still safe <20UH).
There are clear "take me out" lesions, large and heterogeneous.
And there are "i don't know" lesions, which unfortunately, there's little to improve with other imaging (CT washout / MRI / PET).
@Felipegaliza not sure we are ready, but definitely the way to think of a P5: am I confident enough to skip biopsy? If the answer is yes, that's a P5, otherwise, is P4.
@coronilRMD@lkayat@wroclawski_uro we are at the beginning of this journey, learning from @SchuchAlice , @lkayat and many others.
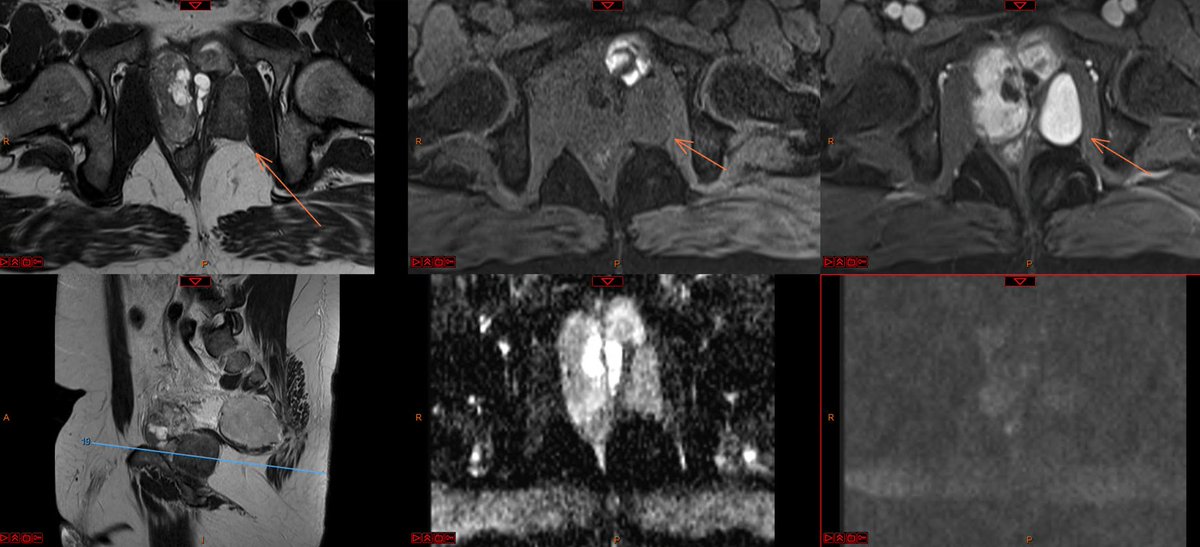
Urethra is retrograde filled with lidocaine (10-15ml). High resolution T2WI are performed, as well as delayed post contrast sequences. finally, dynamic voiding is acquired
@swoo_rad @epi_rad @SAR_ProstateDFP@radiolobt@Purysko@midrisdoc every time I try to argue this, i get a disapproval from senior colleagues: "if you want to do different from what is stated on the document, than create your own system".
But think about it: weren't we using bosniak on MRI before the updated version?
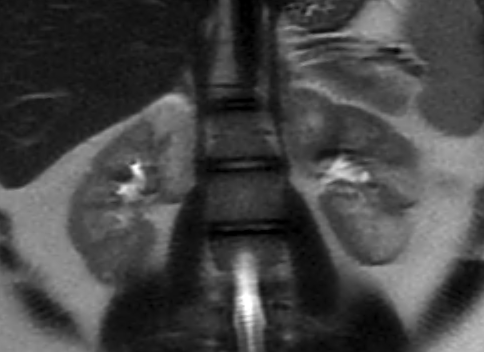
Young patient with right scrotal pain w/o trauma. US shows anechogenic lesion with no Doppler. 2 MRIs 2 months apart show the evolution of a testicular segmentary infarction to a scar. Knowing this pathology could avoid an unnecessary orchiectomy. #radiology#urology