Abdo/Cancer Imaging & Deputy Lead for Faculty Development @Imagingtoronto, Vice Chair EDI @UofTMedIm & Asst. Prof @UofT, 🇮🇳President 🏅.Proud husband.🐇Pa
Just remember every time you hear an ad for "whole-body MRI" it's based on a pack of lies and against the clear recommendations of Canada's credible radiologists.
https://t.co/FzJ7vZRb9q
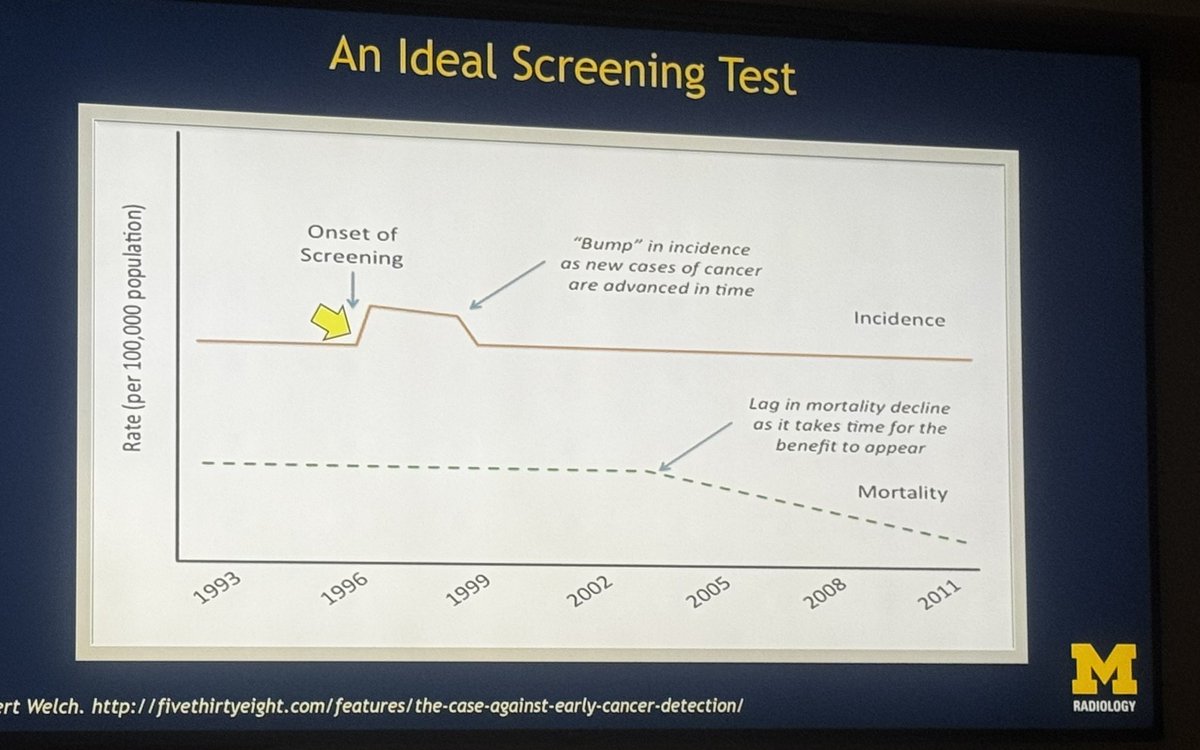
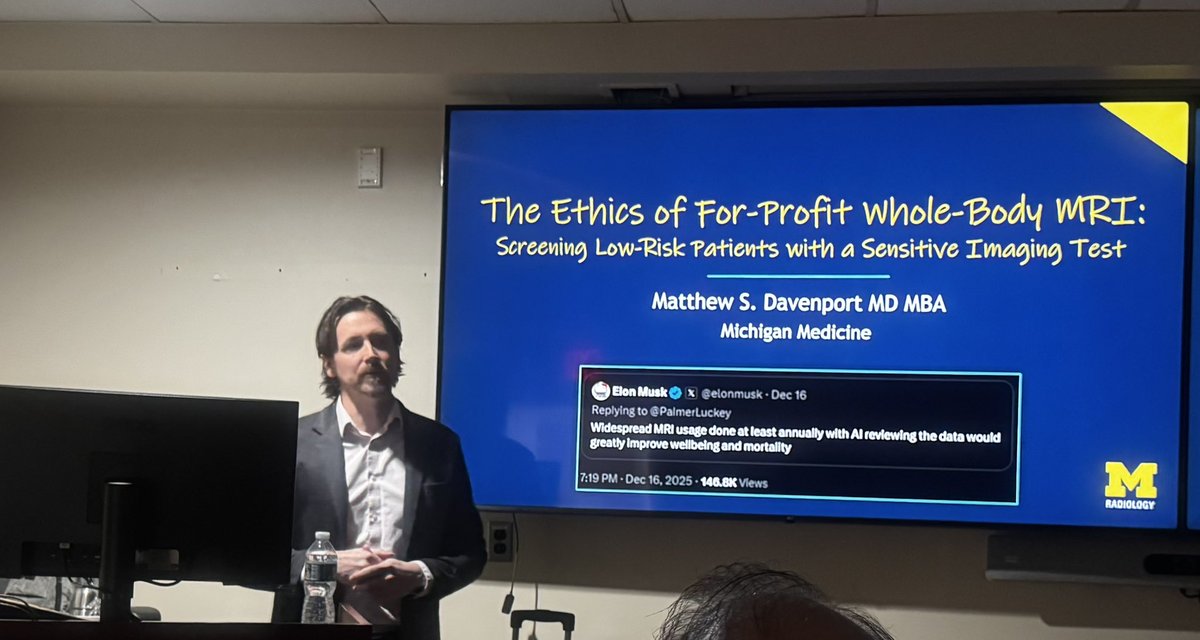
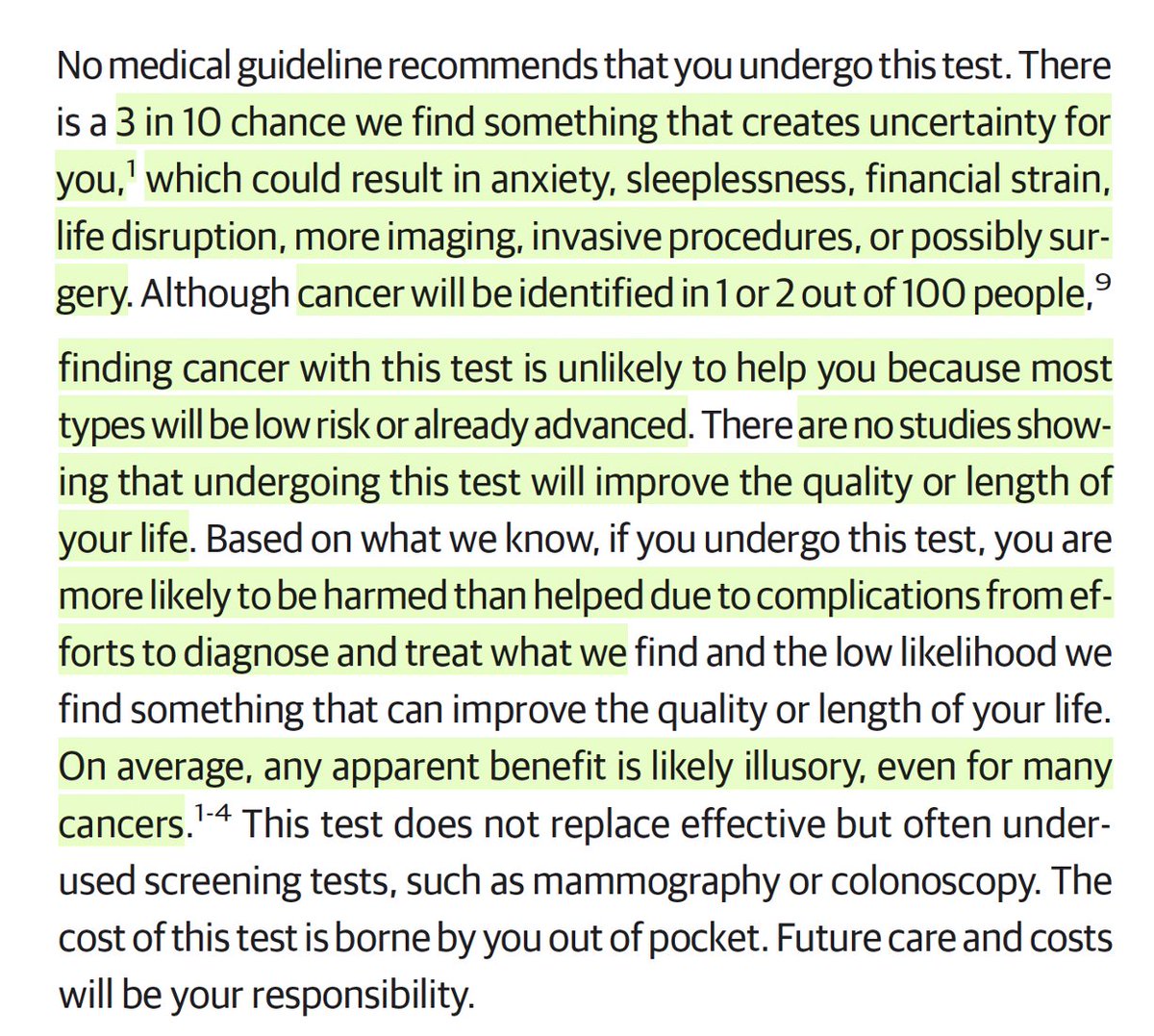
At @JAMA_current today, 2 radiologists publish what should be the consent form for a total body MRI in healthy people
Note: "no major medical society recommends whole-body MRI screening in the general population because it is unproven, and the harms likely outweigh the benefits."
https://t.co/TRSkxDwb6K
AI cuts MRI scan time from 23 to 9 minutes at Amsterdam cancer center.
“We are already seeing that we can perform 18 more examinations in a week than before[...] We can also take more time for each patient, and staff can take breaks more often.”
This week, the "AI replacing doctors" debate is back. The CEO of America's largest public hospital system says he's ready to replace radiologists with AI. The Stanford-Harvard NOHARM study shows top models outperforming generalists. The discourse is moving fast.
I run AI at @UHN, the largest hospital in Canada. Here's what I actually see.
We've developed AI models across imaging, pathology, and clinical decision support. In controlled conditions, the accuracy numbers are real. In some narrow tasks, models genuinely outperform. That's not hype. But the operational reality of running these systems inside a large hospital teaches you things benchmarks never will.
The errors that hurt patients aren't the confident wrong answers. They're the quiet omissions, i.e., the thing the model didn't flag
because it wasn't in the training distribution. NOHARM found 76.6% of AI errors were omissions. We see this too. And in a hospital, a missed finding doesn't just affect one case. It propagates: the downstream physician trusts the AI read, the patient waits, the window closes.
The accountability structure also doesn't exist yet. When an AI-assisted diagnosis leads to harm, who is responsible: the physician, the hospital, the vendor? In Canada, we don't have a clear answer. No hospital system deploying AI at scale does. That's not a regulatory delay. That's a fundamental gap in the infrastructure for AI-in-medicine.
What I'm genuinely optimistic about: AI is already changing how our radiologists work. Not replacing them, but changing the shape of the job. Routine reads get faster. Their time shifts toward complex cases, clinical correlation, cases where the AI flags uncertainty. That's the right direction.
But "ready to replace radiologists" skips 10 hard years of work on deployment infrastructure, liability frameworks, clinician training, and failure mode monitoring that nobody wants to talk about because it's less exciting than accuracy benchmarks.
The capability question is nearly answered. The deployment question has barely been asked.
CEO story:
https://t.co/4O4Z4tAtpp
NOHARM paper:
https://t.co/Q23ClUl01a
I am highlighting an important editorial recently published in Cancer Imaging “the official journal of @ICIS_News written by my friend Hersh Chandarana
This editorial discusses important barriers to MRI access in cancer imaging, including increasing demand, workforce shortages, and infrastructure costs, and highlights technology-driven solutions that may help expand equitable access to high-quality imaging.
You can read at
https://t.co/RRqCRI3mP6
New @AJR_Radiology Accepted Manuscript:
"Personalized Rule-Based Proofreading for Speech Recognition Errors in Radiology Reports: Development Using Artificial Intelligence Coding Assistance"
By Dr Araki @BrighamRad
https://t.co/zunyocCIv1
Update on Management of Incidental Findings Seen on Imaging Studies of the Abdomen and Pelvis
An excellent review from @UCDRadiology@GhanehF@MTCorwin
https://t.co/R2CDuL1al2
Same-Day Multidisciplinary Clinics for Patients With Newly Diagnosed Adult Solid Tumor Cancer: A Systematic Review | JCO Oncology Practice https://t.co/QYB55RUA7e
ImmunoScape is pioneering innovative cancer therapies, and its upcoming clinical trials targeting pancreatic, ovarian, and mesothelioma cancers are highly encouraging. As an investor in @ImmunoScape, I hope to play a small role in helping accelerate their development. #ImmunoScapePartner
Good to see our health care workers and hospitals get the recognition they deserve.
As we protect Canada’s world-class health care system, we’re also determined to make it better — by building new facilities and ensuring our health professionals have the support they need.
💬 Viewpoint: Medical education should shift from pattern recognition to critical thinking and pathophysiological reasoning to reduce diagnostic errors and adapt to #AI advancements. #MedEd
https://t.co/yyhCG5IclQ
Science has turned into a gossip rag, publishing sensationalized takes and personal drama instead of ideas. It has taken extreme political positions, abandoned merit, and filled its editorial boards, reviewers, authors, and research topics with ideology over substance. Ghostwriting is the least of its problems.
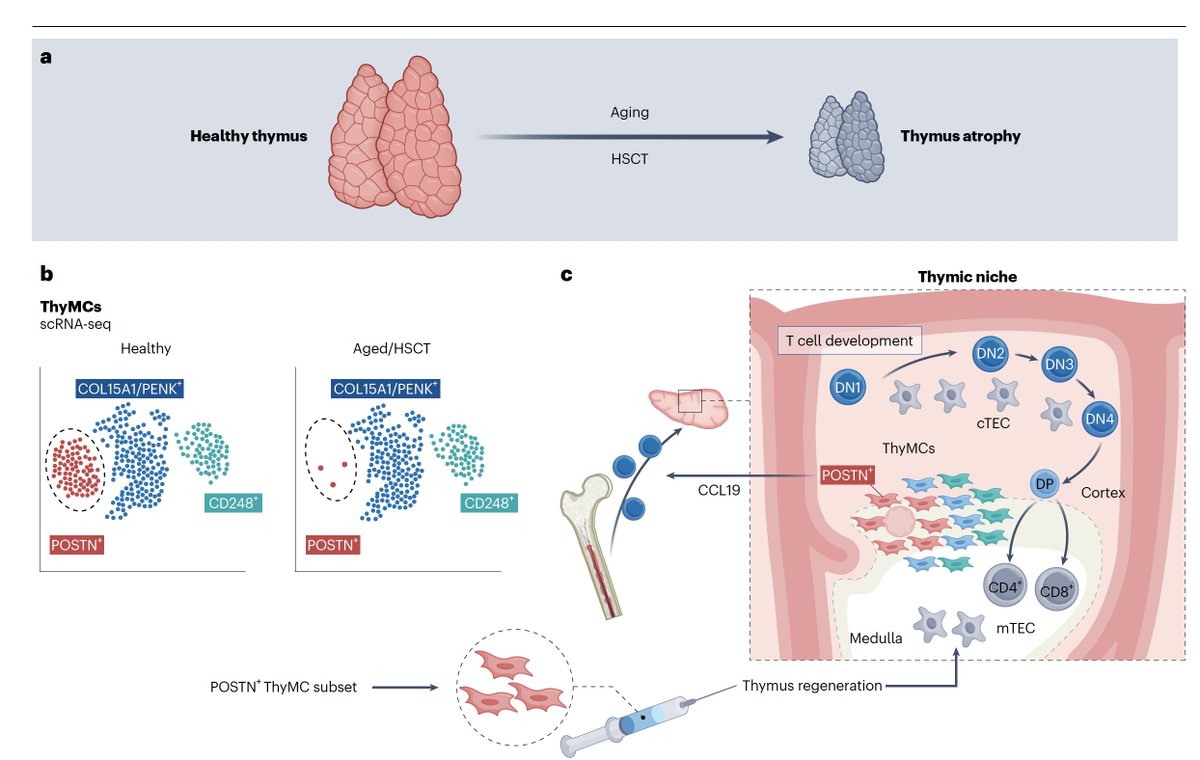
Discovery of a way to regenerate the thymus gland through mesenchymal cells, with implications for enhancing the T cell immune response in multiple medical conditions and with aging
https://t.co/fR0UlPfFgB
https://t.co/DhEU4yhkeR
Why fundamental research is fundamental to progress, seeding major breakthroughs
Editorial @Nature this week
And 7 basic science discoveries that changed the world
https://t.co/0YrKabc7ff
https://t.co/SM11QSJhWz
📌Inaccurate lymph node clinical staging in early and intermediate-risk rectal cancer
@EORTC
🚨19.5% understaged and 62.4% overstaged
✅Seems no survival effect
➡️At least a destressing data when MRI shows 1-3 small lymph nodes that we can not decide whether pathologic or not
👉https://t.co/wp4feb9BVc
#cancer #oncology #MedX #rectal @OncoAlert@realbowtiedoc@GIMedOnc
Hi Everyone. A message from an Editor-in-Chief.
The mission @acsJACS is “Exceptional Science for the practicing surgeon in the House of Surgery”.
For those submitting articles to JACS, we’ve now put in place a structured format for those articles that are rejected.
Headings after the rejection notice include:
▪️JACS Editorial Review
▫️Summary Guidance for Authors
▪️Alternative Options - journals that may be a better fit for the submission
Please remember: The most common reason for rejection is non-alignment with the journal mission. There are a lot of great medical/surgical journals in the marketplace.
Presubmission inquiries can be sent via email:
[email protected]
A few slides from our @RASACS talk during #ACSCC25 @AmCollSurgeons below.
Thanks! 🙏🏾
Let’s take a look at a timelapse of how I create surgical illustration articles.
Some suggest I could be more efficient by modifying a master template—but I always start from scratch, paying respect to the unique anatomy of every case.










































![trajektoriePL's tweet photo. AI cuts MRI scan time from 23 to 9 minutes at Amsterdam cancer center.
“We are already seeing that we can perform 18 more examinations in a week than before[...] We can also take more time for each patient, and staff can take breaks more often.” https://t.co/XixanEgvaR](https://pbs.twimg.com/media/HFKD6gtbcAAnpI0.jpg)