@aribindi I don’t know if I’d call that shenanigans or inclusion criteria. the Minneapolis team also uses lactate (we don’t) to decide on initiation. Getting access and keeping train moving while awaiting more data seems fine to me.
New study: eCPR programs don't harm cardiac arrest patients who don't receive eCPR — and with hands-on training + MCDs on ALS units, survival AND neuro outcomes actually improve. A rising tide lifts all boats. 🫀
Full text: https://t.co/o2Xzq2pi7z
@aribindi Well aware of European model built on longstanding robust prehospital physician response to OHCA; not sure it would be as same/as easy here. ECPR program in San Diego produces similar neuro intact survival:
Paris: 29%, https://t.co/0y13gIJ4mo
SD: 25%, https://t.co/zC0MWKzkUU
@aribindi But also expensive to pay physicians to be on call 24/7 to respond to a small subset of OHCA cases for eCPR. Overall, resource intensive but we need to look at cost and impact on system, not just individuals treated w eCPR (where we’ve all seen individuals who can benefit).
@aribindi think it depends. Some high performing EMS systems can identify patients who are very likely to be eCPR candidates and only transport those. in other systems where there are already prehospital physician teams responding to calls, prehospital ePCR may make sense.
@aribindi Whether to do eCPR in prehospital environment vs transporting to hospital
is highly system dependent. not all EMS systems can/should be configured to deliver prehospital (or in-hospital, for that matter) eCPR.
@aribindi Did you read article? Not about transporting non-eCPR patients. Most OHCA pts aren’t eligible for eCPR. But systems must be reconfigured to facilitate rapid transport of the few that are. this study asked whether such a system was associated with outcomes in non-eCPR pts.
@TheYZA13@RafaelOliveLeit@aclong111 Arbitrary time cutoff is not the way to prognosticate, IMO. this is why we do multimodal testing. For those who are truly indeterminate, shared decision making about goals and values re: duration of continue support and uncertainty is my approach.
@RafaelOliveLeit@aclong111 unfortunately, we’ve known for over 10 years that a third of patients who awaken do so after 3 days. The approach you outline above, if I’m understanding correctly, would inaccurately categorize those patients as “bad prognosis”.
https://t.co/a7QOAseJX5
https://t.co/g2KzD0Vbit
Out-of-hospital cardiac arrest can look devastating early.
The neurologic exam may be poor. The CT may show edema. Families understandably want answers immediately.
But one of the most important principles in post-arrest care is avoiding premature neuroprognostication.
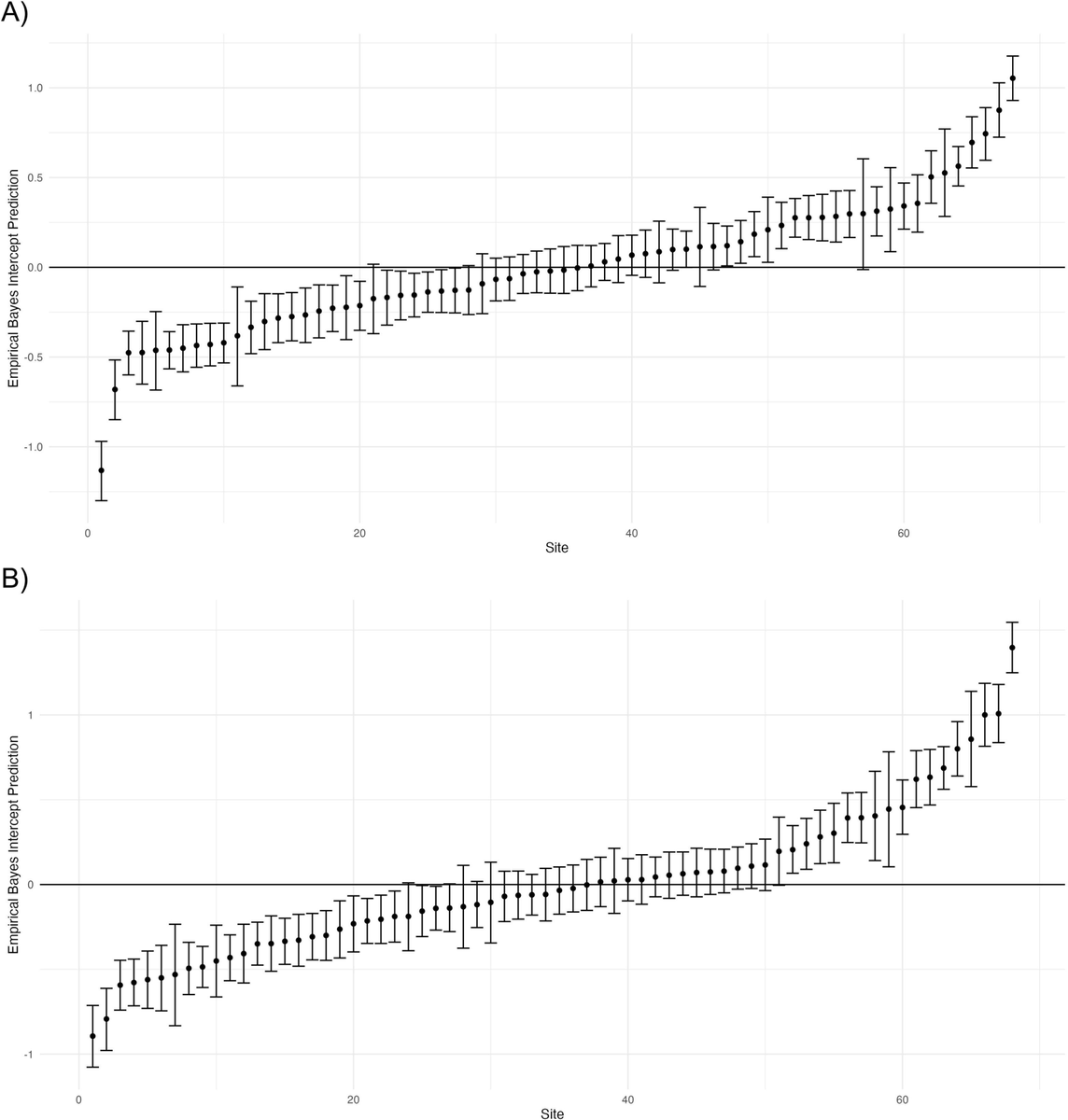
Between-hospital variability in outcomes after cardiac arrest in a large clinical trial network. See unadjusted (A) and adjusted (B) survival to discharge from #ICECAP sites. Variability likely worse out of clinical trial sites. @ResusJournal https://t.co/ih4BXgbzS7
In adults with moderate to severe #ARDS, inhaled sevoflurane sedation produced fewer ventilator-free days and lower 90-day survival than intravenous propofol, raising safety concerns including acute kidney injury.
🎥 Watch the video and read the full article: https://t.co/Tm8iW1psPm
1/ There is a lot about my job in pulmonary and critical care medicine that I find deeply meaningful. But one thing really weighs on me these days, and it is this. 🧵
📊 Research Summary: Restrictive vs liberal wrist-strap restraint strategies in ICU patients receiving mechanical ventilation produced similar outcomes for delirium, coma, self-extubation, and mortality.
🔗 https://t.co/41unfiJIDU
#ISICEM26#ICUCommunity
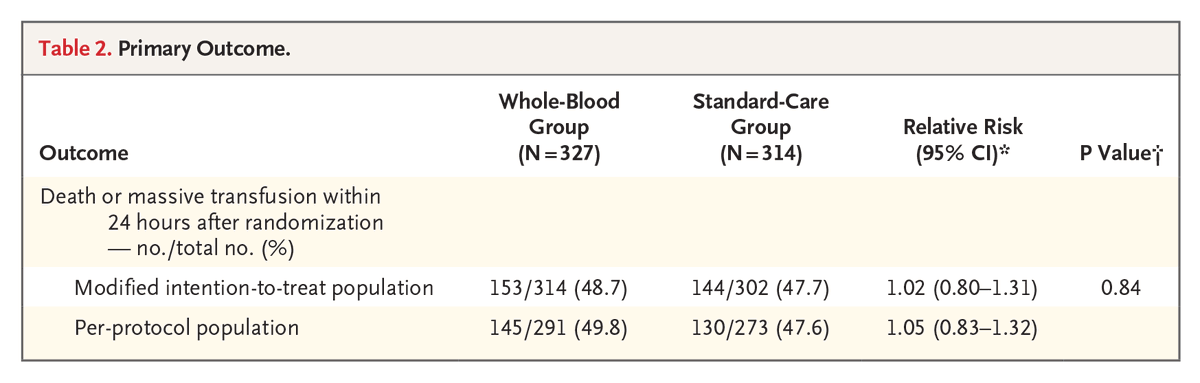
Presented at #ISICEM:
Among patients with traumatic hemorrhage, prehospital whole-blood transfusion was not superior to standard transfusion with red-cell and plasma components in reducing the risk of death or massive transfusion. Full phase 3 SWiFT trial results: https://t.co/67l1bSI81L
@ISICEM