KRUK/IC clinical research fellow, nephrology and GIM dr, proud dad, spectacular husband. None of this is clinical advice. Views often inspired by clever people
This describes our experience managing #haemodialysis patients with #COVIDー19@ImperialNHS community dialysis unit incl risk factors for deterioration and (zero) staff infections
https://t.co/lF58RDe0Qy
@HotKidneyAction@NephJC Read correctly. I think you're right; it prob contributed. We were trying to compare the two regimens, not identical treatment durations. Interesting that even a long (ish) course of treatment with Tac was well tolerated #NephJC
@carlo_alfieri@NephJC Doses were similar but because multicentre, indvidual agents and doses used varied and statistical comparison difficult. We didn't insist on maximal RAASI. Clinically, we don't max RAASI before starting pred or tac in MCD #NephJC
@ThePeanutKidney@aishaikh@Ashidotic@renalpathdoc@SethiRenalPath @toates_19 Yes, can detect by IP, but sensitivity meant to be better with IF. The extra step is the pronase antigen detection, but if done correctly, IP and IF should work. You can always refer slides to Terry Cook who does this routinely on most C3G pts, esp those over 50yrs age
I’m convinced! From Famine to Feast - clinical trials in #IgAN from Dana Rizk at @ASNKidney#KidneyWk. But how do we select and stratify our patient for all these competing studies? @NickRhysMT@IgAN_JBarratt
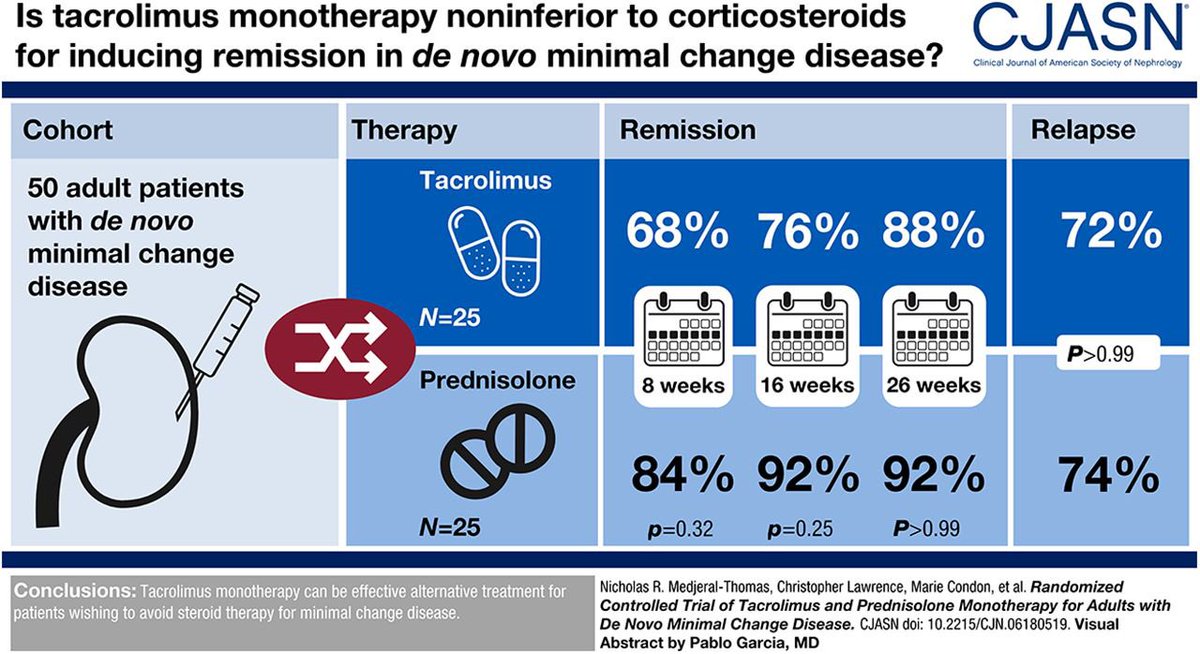
Grilling them? Ha, nah, more like praising them. Important work from @megan_griffith1 and @NickRhysMT providing an efficacious alternative to high dose steroids for minimal change podocytopathy. @LGlomcon #KidneyWk