Raising awareness about post-SSRI sexual dysfunction (PSSD). Tweeting about upper airway resistance syndrome (UARS) & ME/CFS (& related disorders) @nataliezzz3
Follow @PSSDNetwork and @PSSDInstitute to learn more about and stay updated on PSSD. If you’re interested in my UARS and ME/CFS content, follow me @nataliezzz3 (and I somehow accidentally “left” my UARS 🧵 on this account so I won’t receive any notifications related to it, btw)
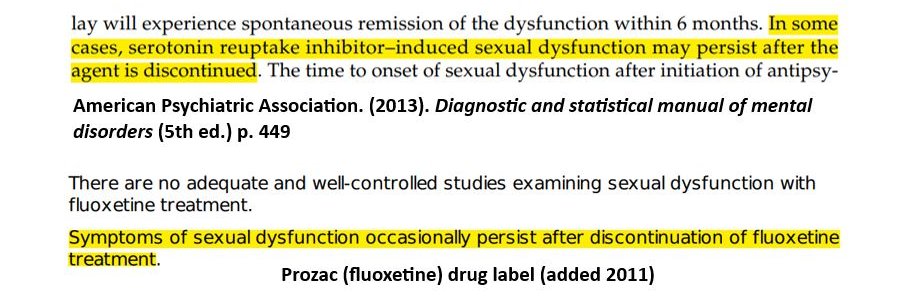
POST-SSRI SEXUAL DYSFUNCTION (PSSD) is a condition where genital numbness/⬇️ sensation (& other sexual side effects) persist after treatment w/ a serotonin reuptake inhibitor (SSRI/SNRI/etc.) Non-sexual symptoms like emotional blunting, anhedonia, & 🧵 1/n
https://t.co/QckKiukPKH
Amazing @IamBrandiCarlil ASL cover. From the comments: "If the world could bottle your right dimple I think we could solve world peace." 😄🥰
https://t.co/PTITzOmnCJ
This is such a cool style of Irish dancing. I miss dancing; never did Irish/tap though -- I wonder if I can cure myself of ME/CFS if it's too late to start in my late 30s?
https://t.co/PTtiiZvoAv
@Davemconte@creeront Then why do you see only a weak correlation between AHI and sleepiness (& no correlation with fatigue/psychomotor vigilance)? Since most (hypoxic) apneas/hypopneas terminate in an arousal, you should see a correlation if arousals are the cause of symptoms.
https://t.co/Qga3N6OpYj
"Eppur si muove, baby." Yup.
You can show ppl piles of evidence that sleep fragmentation is not cause of fatigue in SDB pts & a SDB stress response can cause ME/CFS/fibro/etc. but ppl will ignore it & continue to believe what they want.
The truth will come to light one day. 1/
"Windows" suggest capacity for normal function is preserved—& finding out out how to stabilize "windows" may be a promising treatment approach. Many PSSD cases may require intervention at multiple levels: epigenetic (HDAC inhibitors/CRISPR); peripheral (shockwave/laser/etc.) 5/n
A 2025 case series by @KennethMPeters1 & colleagues at @BeaumontUrology tested treatments targeting peripheral genital nerves in 3 male PSSD, PFS & PRSD patients. Modest improvement in some symptoms was noted but patients remained profoundly affected. 70/n
https://t.co/6Oqqrp3sAq
An epigenetic etiology for PSSD offers a unifying framework for many of its features: diverse symptom constellations/severities, variable exposure/onset timings, & objective findings like SFN. If not coming from my main 🧵 see ⬇️ for referenced @abcsoka & colleagues papers. 🧵1/n
Potentially unifying the diverse symptoms of PSSD discussed here, @abcsoka & Szyf propose that drugs can cause enduring epigenetic changes—alterations to DNA methylation & chromatin architecture—resulting in various persistent post-treatment effects. 88/n
https://t.co/7pnj75FBun
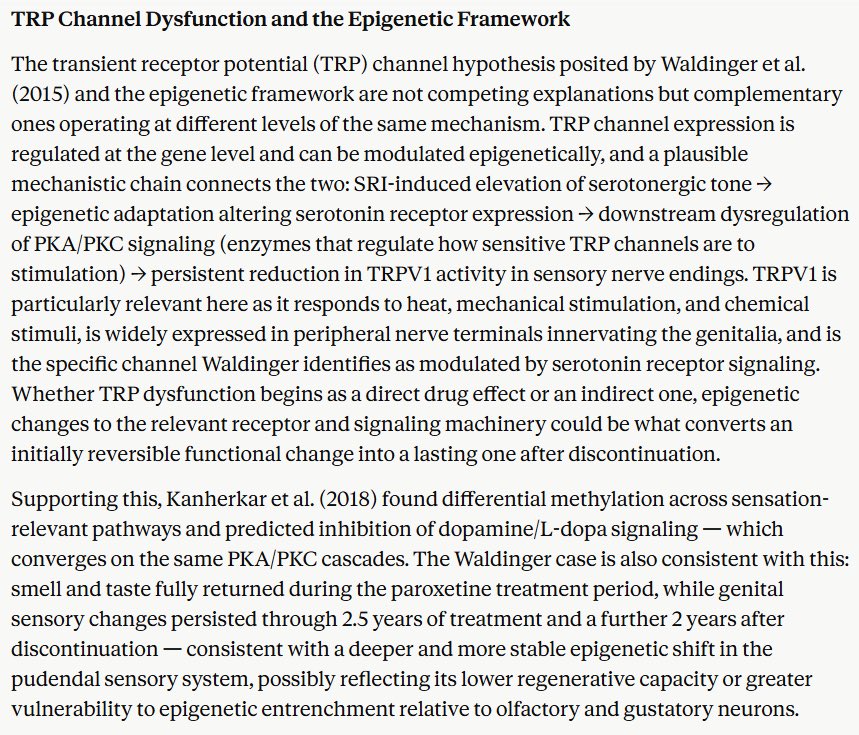
The TRP channel hypothesis & epigenetic framework are complementary: epigenetic adaptation altering serotonin receptor expression could produce persistent ⬇️ TRP channel activity in sensory nerve endings—converting an initially reversible functional change into a lasting one. 4/n
Case report supporting a peripheral element to the numbing: man w/ total penile anesthesia 2 years post-tx w/ paroxetine (he could rub Tiger Balm into his penis & feel nothing) regained partial tactile sensation w/ low-power laser irradiation (LPLI). 32/n
https://t.co/4bNKG72bpL
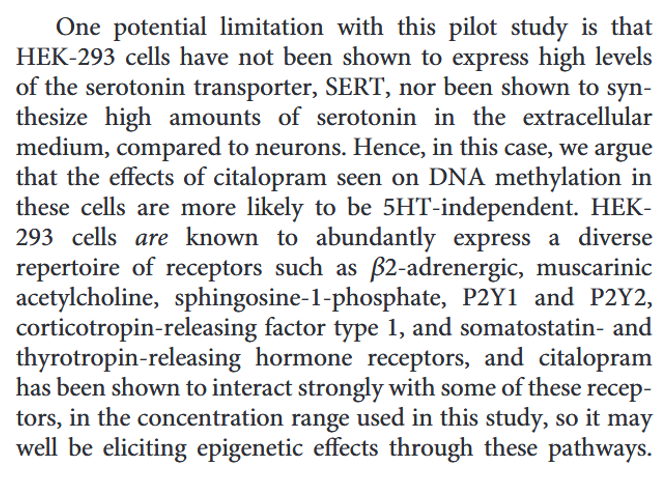
The epigenetic effects observed were likely serotonin (5HT)-independent, though the authors note 5HT-dependent effects may also occur. Findings relevant to sexual function included downregulation of the OXT (oxytocin) gene and predicted inhibition of dopamine & FSH pathways. 93/n
POST-SSRI SEXUAL DYSFUNCTION (PSSD) is a condition where genital numbness/⬇️ sensation (& other sexual side effects) persist after treatment w/ a serotonin reuptake inhibitor (SSRI/SNRI/etc.) Non-sexual symptoms like emotional blunting, anhedonia, & 🧵 1/n
https://t.co/QckKiukPKH
Pathway analysis revealed effects spanning nervous system development & function, neurotransmission, dopaminergic & neuroendocrine signaling, & sensation. Predicted upstream regulators included NFκB (inflammation), dopamine/L-dopa signaling, BDNF (nerve growth factor) & FSH. 92/n
@PSSDNetwork@GrantS0227 PSSD & PFS def. do NOT belong under an umbrella with ME/CFS & PTSD tho (if anyone thinks that is going to help PSSD's cause, think again lol--take it from someone with ME/CFS). An epigenetic theory fits PSSD & PFS nicely; it makes little sense for ME/CFS:
https://t.co/WR0LJYDHMj
@PsychotropicDC@awaisaftab@BShapiroMD Ppl do say this tho (scroll up): I was explaining why @BShapiroMD's hypothesis that PW is a "central sensitization" syndrome (of which CFS is 1 of many, incl. fibromyalgia/IBS/etc) makes no sense (the person I was responding to in the tweet on my @nataliezzz3 account argued same)
@atomicaceso@awaisaftab It goes back to my point about POTS being heterogenous tho. While POTS may be a transient WD/tapering-related problem for some, for others w/ SRI-related damage/dysf. it may be a more enduring problem. At least 1 PSSD pt in this tracker received an immune-mediated SFN w/ POTS dx.
@atomicaceso@awaisaftab “Normal POTS never goes away”—it does w/ treatment (see my informal case report ⬇️, and the published case report of resolution of low BP/orthostatic intolerance [not POTS specifically] w/ CPAP in the link above). OI/POTS can spontaneously remit too (but I understand your point).
@DocBorelli and some ppl (myself included) have had both OH & POTS, even alternating between the 2 within short time frames. My acute symptoms on standing are largely resolved on BiPAP (confirmed by pre-BiPAP vs. on-BiPAP tilt table tests) & my overall dysautonomia/OI is greatly improved. 3/