Presented at #ASCO26:
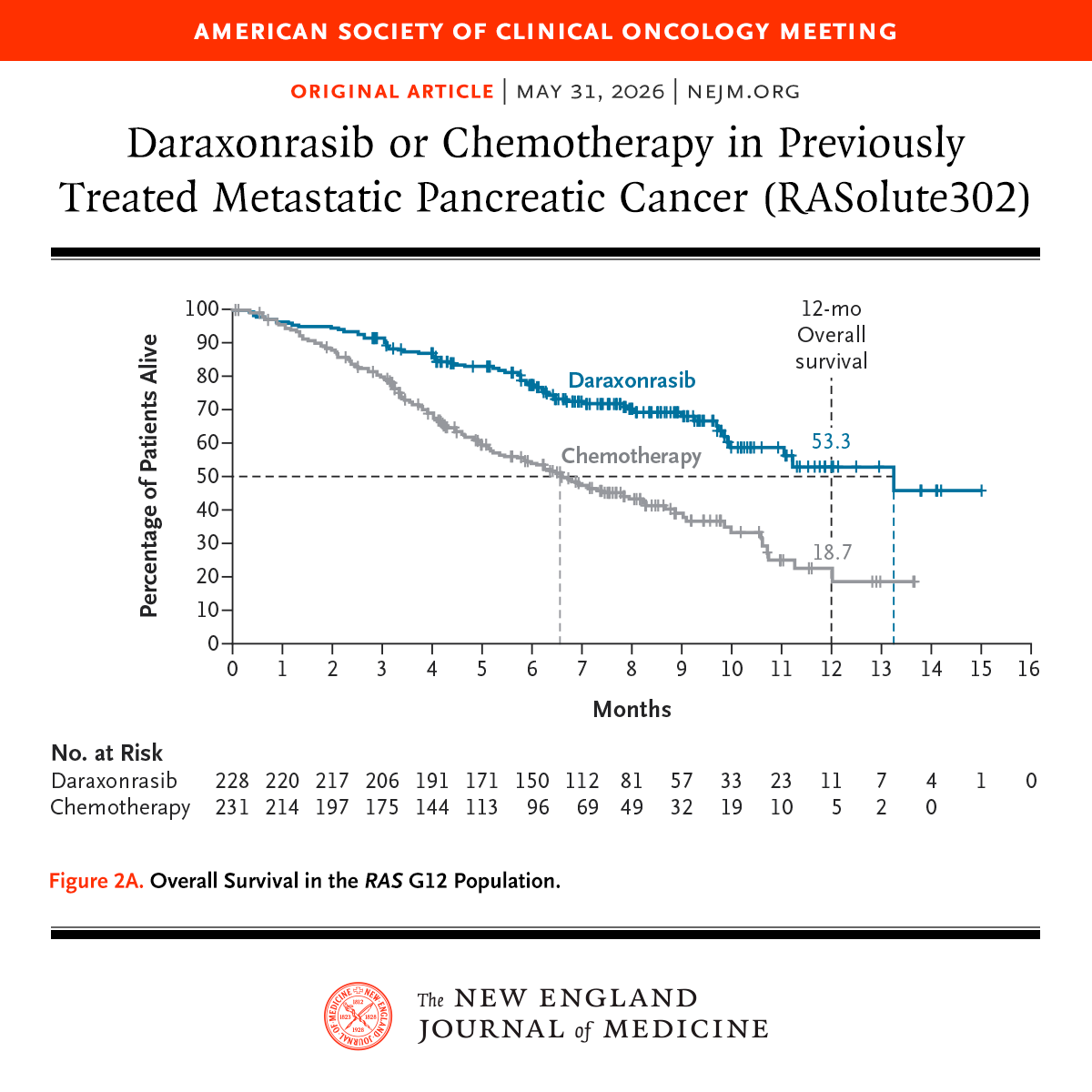
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
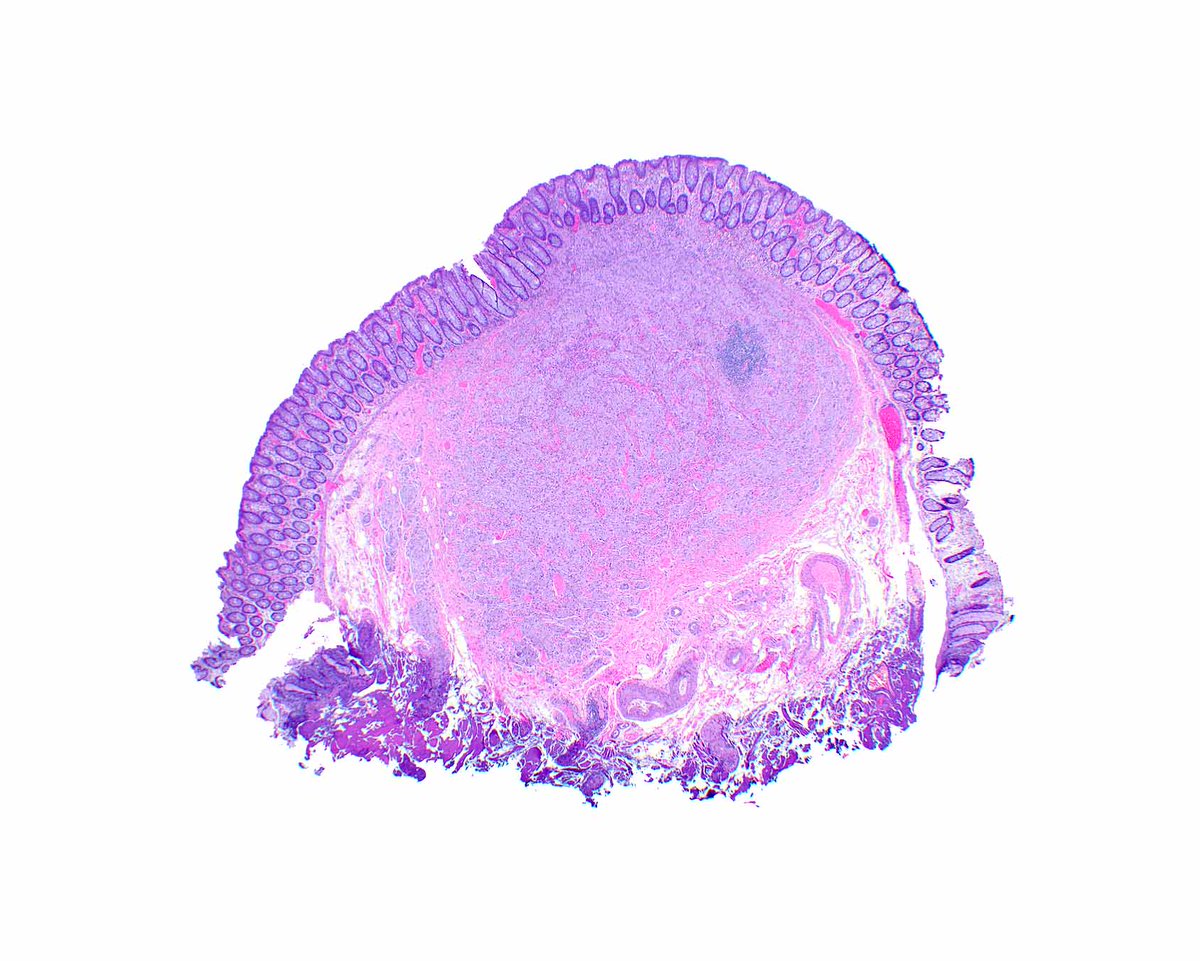
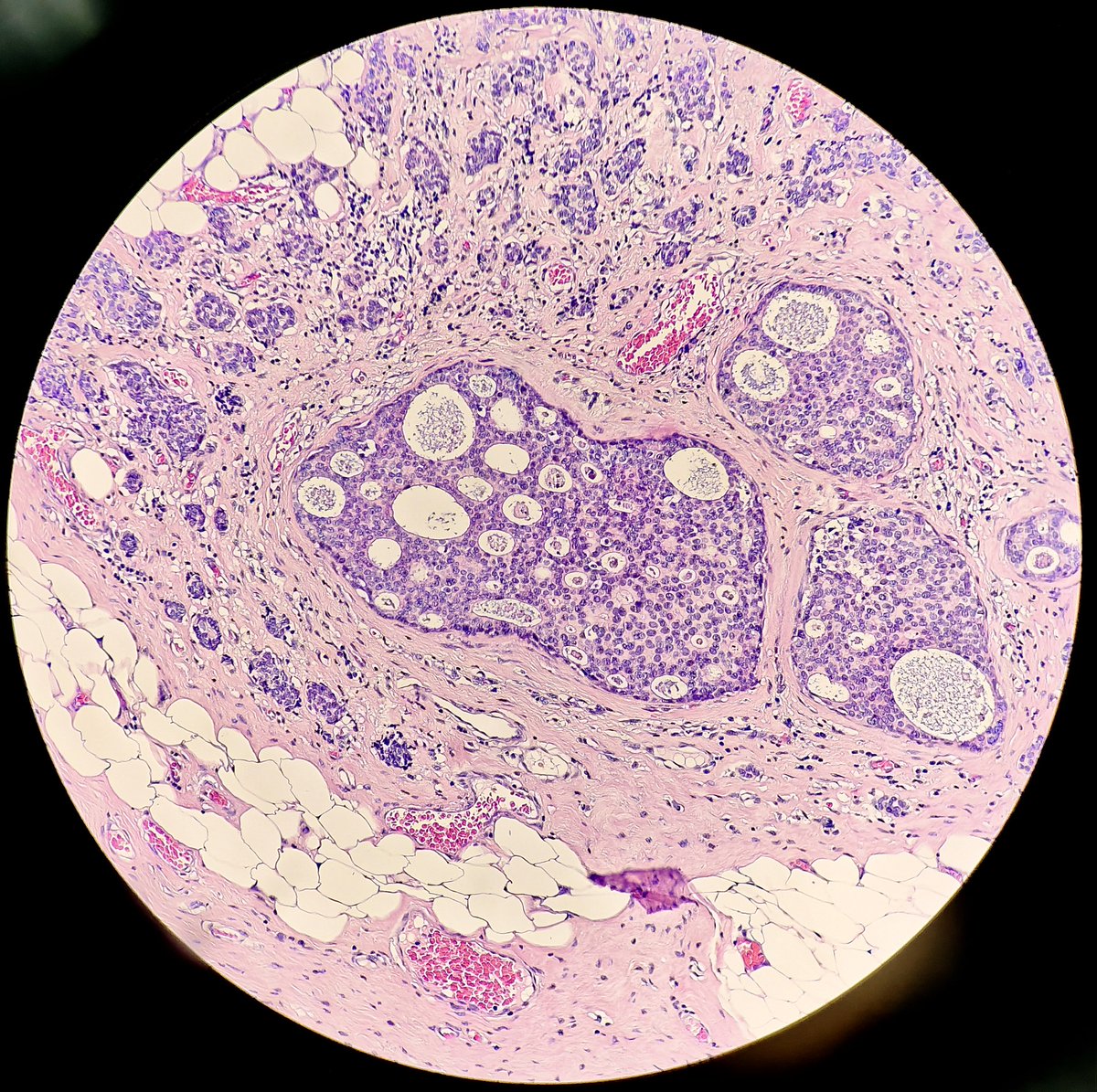
Atypical lipomatous tumor/well‑differentiated liposarcoma and p16: what pathologists should keep in mind 🧬🧪
Short thread on morphology of atypical lipomatous tumors (ALT/WDL) and how to use p16 wisely in daily sign‑out.
Definition 🧾
ALT/WDL is a well‑differentiated adipocytic neoplasm, locally aggressive, with nuclear atypia in fibrous septa and typically associated with MDM2/CDK4 amplification in 12q13‑15.
In practice, “large deep lipoma vs ALT/WDL” is one of the most common soft‑tissue dilemmas.
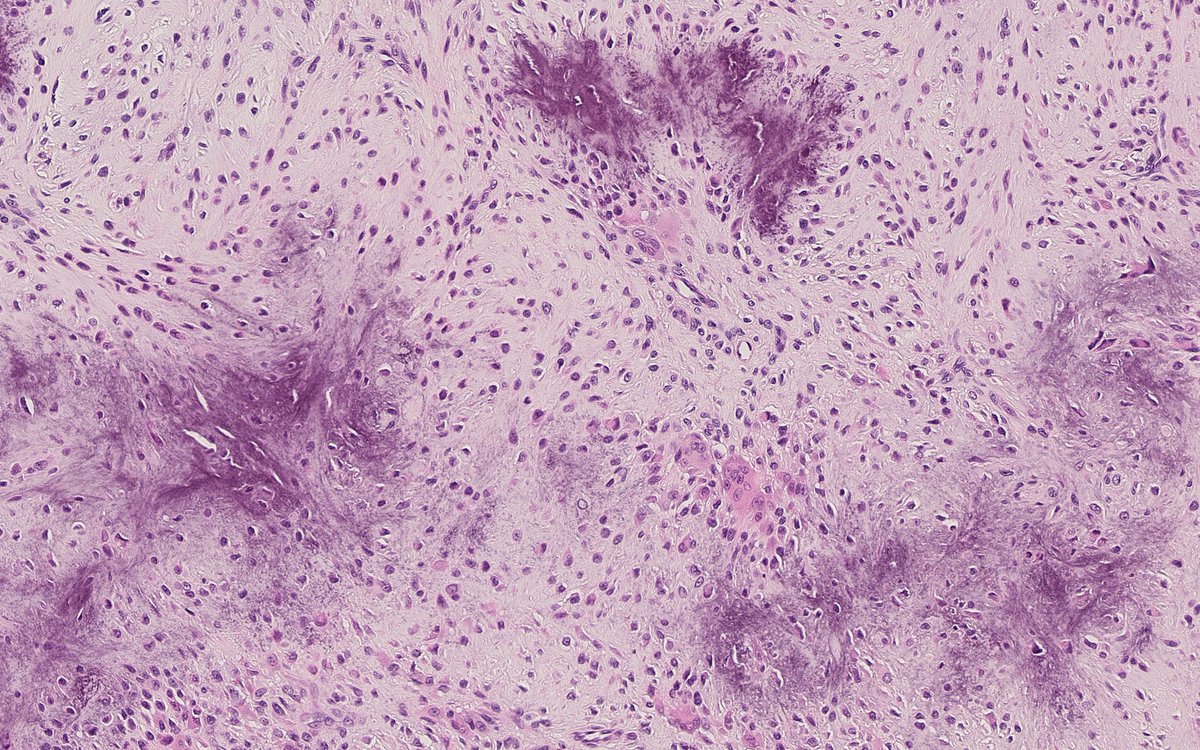
Histology: what to look for on H&E 🔬
Architecture
Predominantly adipocytic, lobulated lesion, often very similar to a lipoma.
Thickened fibrous septa, sometimes hyalinized, traversing the adipose tissue.
Cytology
Mature adipocytes with mild variation in cell size, usually without striking pleomorphism.
Stromal cells in septa with hyperchromatic, enlarged nuclei, sometimes frankly bizarre (“marker cells”).
True lipoblasts can be rare or absent and are not mandatory for diagnosis.
Special patterns/pitfalls
Large lipomas may show fat necrosis, inflammation and fibrosis that mimic “atypical” septa.
Intramuscular lipomas, spindle cell lipoma and pleomorphic lipoma may show nuclear enlargement, but in a different, more “dysplastic” than overtly sarcomatous pattern.
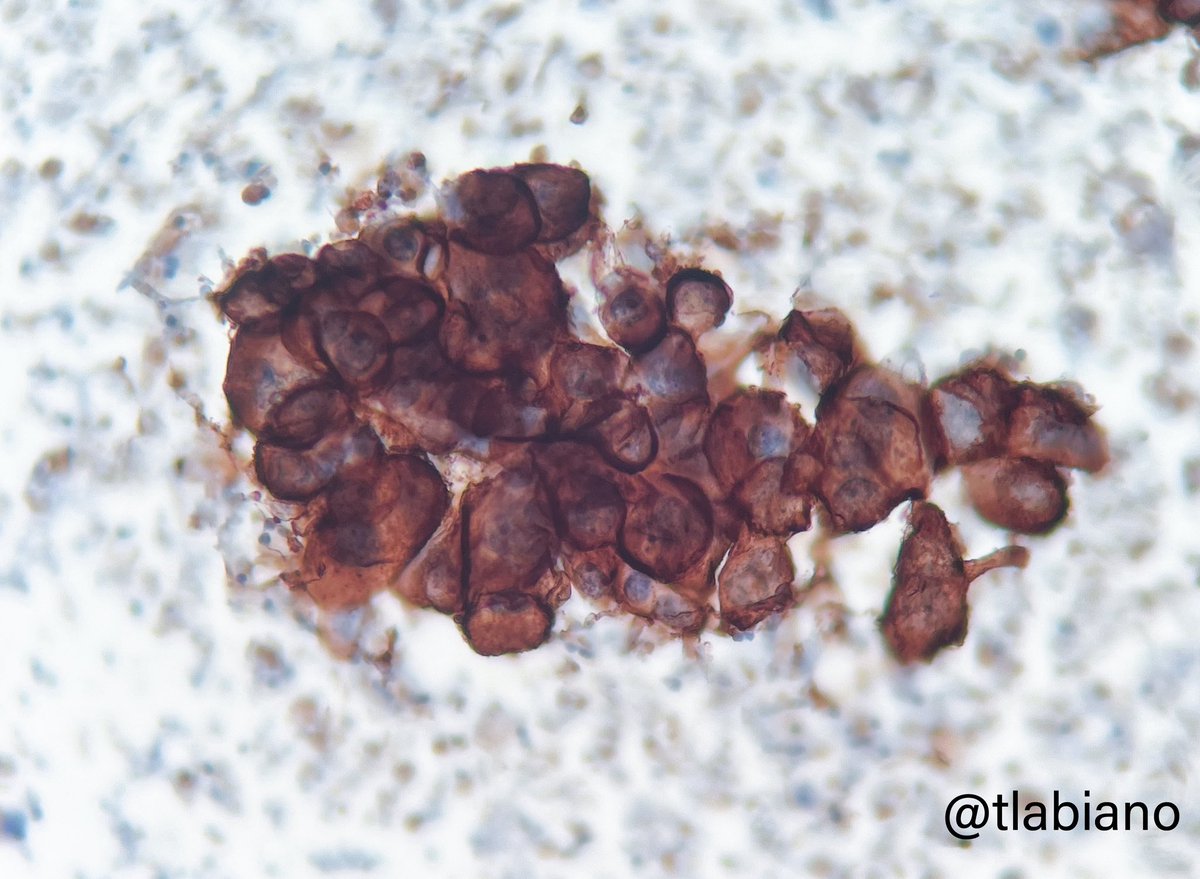
p16 in practice: when it helps, when it hurts 🧷
What does p16 stain in these tumors?
Diffuse, moderate–strong nuclear overexpression is frequent in ALT/WDL and in DDL, in both atypical adipocytes and septal spindle cells.
In large series, p16 has been the single most sensitive marker for WDL/DDL, with specificity also high when strict nuclear criteria are used.
⚠️Lipoma vs ALT/WDL⚠️
Several studies show p16 negativity in essentially all deep “ordinary” lipomas, with strong positivity in most ALT/WDL cases.
However, lipomas with fat necrosis and secondary/reactive changes may show adipocytic nuclear p16 positivity, lowering specificity, especially in small biopsies.
DDL and mimicking sarcomas
DDL usually maintains strong/diffuse p16 expression, similar to the WDL component.
Other high‑grade sarcomas can also express p16, so the marker is not highly specific in that setting; conversely, some myxofibrosarcomas that are MDM2‑positive can be p16‑negative, which is helpful in retroperitoneal cases.
How to interpret p16 in the MDM2/CDK4 panel 🧪
Typical ALT/WDL and DDL scenarios
p16+, CDK4+, MDM2+ (moderate/strong, diffuse pattern): classic profile for ALT/WDL/DDL when morphology fits.
p16+, CDK4+, MDM2– by IHC: ALT/WDL is still strongly suspected; MDM2 FISH may confirm amplification in a subset of these cases.
Patterns that favor benignity
p16–, MDM2–, CDK4– in a deep adipocytic tumor with completely bland morphology favors lipoma (while not absolutely excluding ALT/WDL).
Tumors that are MDM2–/p16– in series with FISH confirmation have been consistently benign.
Key caution points
Avoid calling ALT/WDL based on p16 positivity alone, particularly in:
Small/incisional biopsies.
Lesions with extensive fat necrosis or marked inflammation.
Value diffuse, strong nuclear staining in atypical septal cells far more than scattered staining in reactive areas.
Take‑home messages NotasPatologia 📌
📌ALT/WDL is, morphologically, a “lipoma with septal atypia”; recognizing those atypical septal cells on H&E is the critical step.
📌p16 is a sensitive marker for ALT/WDL and DDL, but its specificity drops in lipomas with secondary changes and in biopsies.
📌The p16 + CDK4 + MDM2 panel is one of the most useful combinations to separate ALT/WDL/DDL from lipomas and other adipocytic tumors.
📌In a large deep adipocytic tumor of limb or retroperitoneum, diffuse nuclear p16 in atypical septa should strongly raise the suspicion of ALT/WDL, ideally backed up by MDM2 (IHC and/or FISH).
📌Never interpret p16 out of context: morphology, site, size and the full panel still outweigh any single marker.
📚Selected references: Thway et al., Am J Surg Pathol 2012; Kammerer‑Jacquet et al., Hum Pathol 2017; Hedayat et al., Immunopathol Persa 2024; Wu et al., Sci Rep 2025.
⚠️Disclaimer: educational content only; does not replace full pathology reports, guidelines or case‑specific clinical decisions.
#Pathology #SoftTissuePathology #Sarcoma #Liposarcoma #ALTWDL #Immunohistochemistry #p16 #NotasDePatologia #MedicalEducation #PathTwitter
🔎Nuevo paso frente al cáncer desde Albacete
▶️El estudio, liderado por la UCLM y el CSIC, identifica dos proteínas clave en el desarrollo de los sarcomas🔻
#cáncer#investigación#sarcomas@CSIC@uclm_es@pacientescancer
https://t.co/IwSWTAFtdL
Agenda formativa | Próximos eventos
🔹 3rd N.O.D.E. Bone Pathology Session 17 feb 2026 | 16:00 CET Dr. Fernanda Amary
🔹 IMPERAS Sarcoma Educational Session 24 feb | 16:30 CET Dr. Luis Pérez-Casanova
🔹 MaGISTraL · Programa Educativo 2026 5 feb 2026 | 16:30–18:00 h
🌐 International Congress on Interventional Pathology.
💉 #ICIP2026.
📺 For those who didn't have the opportunity to watch it live, or in case you would like to review any topics...
⏺️ Recording:
🔗 January 28 https://t.co/a7pTKnNpvE
🔗 January 29 https://t.co/FqUTL0JgLl
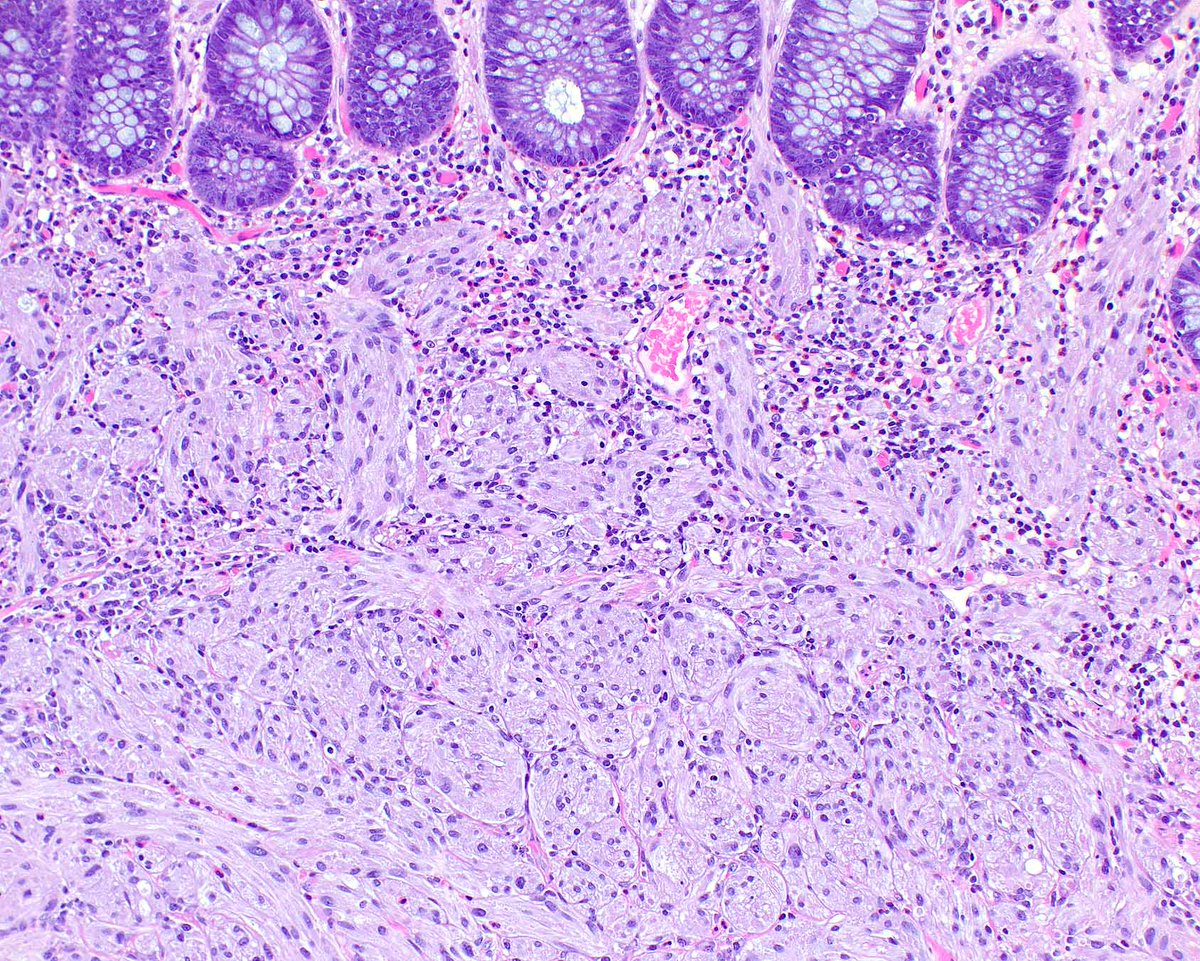
Fun fact - Doug Reye was an Australian pathologist working at Royal Alexandra Hospital for Children in Sydney. I am old enough to have worked with people who worked with him. Although his name is most well know for Reye's syndrome, he actually described two distinct paediatric tumours with which his name is not as intrincially linked these days but used to be in the olden days. These are pictured below. On the left is inclusion body fibromatosis (previously known as 'infantile digital fibromatosis' or just 'Reye's tumour'). On the right is calcifying aponeurotic fibroma. Whilst not common, these two tumours are much more common than Reye's syndrome
Happy to share our contribution to #PediPath. I hope you find it useful! Pathology reporting of hepatoblastoma resections: recommendations from the international collaboration on cancer reporting - López‐Terrada - Histopathology - Wiley Online Library https://t.co/NuIsZ1FwrU
Dear Friends.
👏🏽 We're pleased to announce the First International Congress on Interventional Pathology (Online edition)
🗓️ January 25-25, 2026.
📍 Virtual venue: @HUCA_Asturias.
🔜 Coming soon: Guest Speakers and Registration.
#ICIP2026#InterventionalPathologist
Challenging #FNA#cytology - Apocrine Carcinoma of the breast
🔬Pleomorphic cells w/large nuclei, prominent nucleoli,pink granular cytoplasm.
🏰Arranged in sheets or groups with irregular borders and singly scattered.
🍪HER2 3+ (Androgens +;Estrogen neg).
#breastpath#cytopath
As CLDN18.2 assessment in tissues become increasingly common, important to keep in mind pre-analytical variables like antibody clone. The same tumor can show widely different CLDN18.2 staining pattern as shown in this #GastricCancer.
TL;DR Ventana/Roche (clone 43-14A) way to go.
Before and After. Just 8 weeks.
Nope, not lymphoma.
THIS is non-small cell lung cancer.
THIS is why molecular profiling matters.
THIS is why targeted therapy changes lives.