To make LC more attractive to pharma we need
1. A surrogate biomarker
2. An international patient registry ➡️ reduces costly recruitment
3. Public precommitment by FDA for accelerated pathways for the first effective drugs
Explained: https://t.co/lzfpZUMcdx
#UniteToFight2024
🔍 Have an idea that needs the spotlight? Here's your chance! Recommend a topic for a public session!
How ?
Post your own tweet, mention your topic, and use #UniteToFight2024.
The most mentioned topic takes the stage! 🚀 at our global conference Let's shape the conversation together! 💡 #CommunityVoice #MECFS #LongCovid
It's true of course. Unfortunately it's also true that many scientists are biased towards their particular biomedical hypothesis and vastly inflate the field with "positive" findings
This WIRED article is a clear example of biased writing. It reads like the theory was decided before the evidence was reviewed.
The pro mind-body/psychological quotes are largely from people already invested in that model, so of course they reinforce the article’s premise. The critics are then framed less as a neutral scientific counterweight and more as part of a fear-driven taboo around the author’s preferred hypothesis.
This is selective cherry-picking to support a bias, not balanced science. Very poor from WIRED for publishing this.
@patio11@adamdangelo I remain very curious about how AI is affecting elite decision-making, executives, heads of state etc. It might already be pretty consequential and yet we hear very little of it
@RuxandraTeslo Somebody who confused art as making a statement with art as something beautiful. The former has a place but largely it's not in architecture
@wiredmau5@dwarkesh_sp Funnily enough I think humor is pretty verifiable. Comedians need to test a lot of their homes and their delivery and optimize their performance based on laughter from the audience
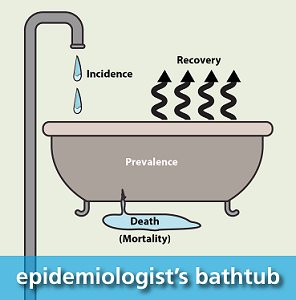
@solodoc Prevalence means how many people have a condition. You always need to take into account recovery for that. You might be thinking of incidence of
These prevalence numbers are insanely high and should ring your skepticism alarm bells.
1) There no control group!
2) This is not a representative sample of the population. They sought out healthcare
3) The data cannot establish prevalence because EHR doesn't track recovery
#LongCovid has not decreased from 2020-2024.
Prevalence is 13-23% of US population, increasing 0.4%-1.5% every 3 months.
Incidence was 10-29%, but began increasing in 2023.
"These findings indicate an accumulating rather than resolving disease burden." https://t.co/SZGm2NFkg0
@solodoc You're trying to measure whether being infected by covid increases the probability of developing chronic health issues, so you want to compare to the counterfactual (this is really difficult btw because almost everyone got infected and those who didn't aren't normal)
These prevalence numbers are insanely high and should ring your skepticism alarm bells.
1) There no control group!
2) This is not a representative sample of the population. They sought out healthcare
3) The data cannot establish prevalence because EHR doesn't track recovery
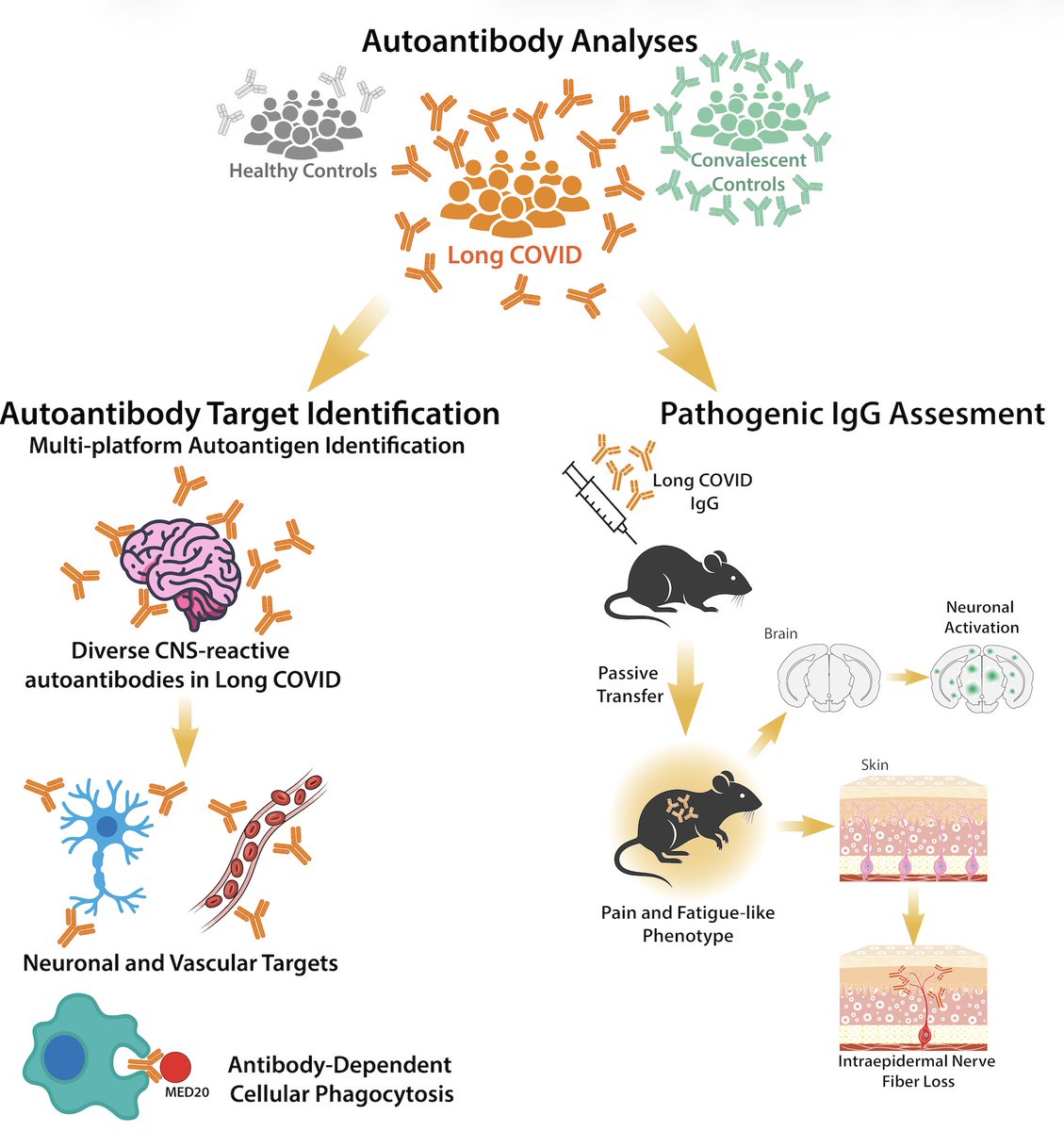
Hi Akiko @PutrinoLab
Can you clarify whether the behavioral experiments were blinded to whether mice were treated or in control group? The methods don't state this. We know that experimenter expectations can bias results
Excited to share our study by @keylas3 et al. on pathological autoantibodies in people with Long COVID. We asked whether IgG in patients with Long COVID bind to human tissues/antigens and cause pathologies when transferred into mice. With @PutrinoLab
https://t.co/tcowCufWyf
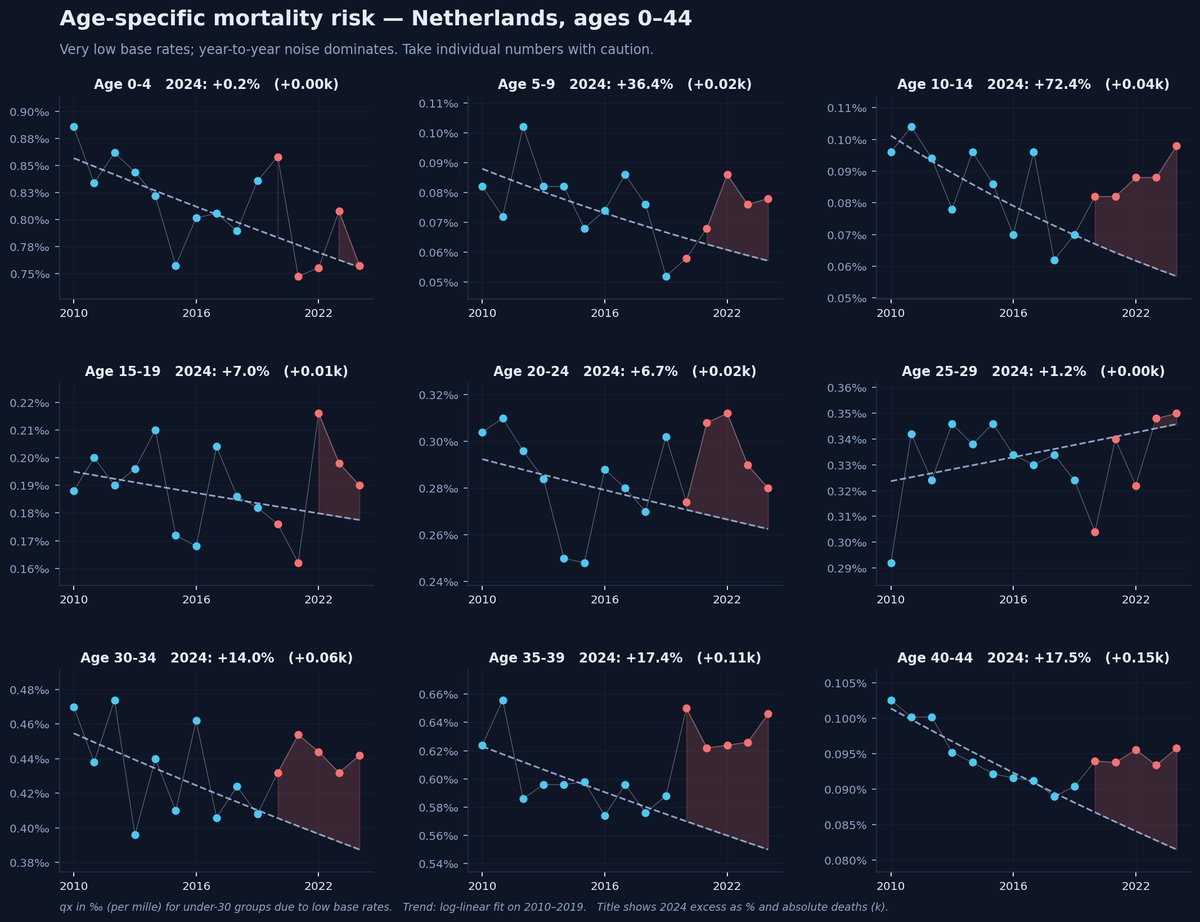
@R9_Fury@simon_faire@JOG412@rubenivangaalen@mzelst@mkeulemans Thanks that's really useful.. I'm an amateur working with Claude on this. CBS has age specific mortality data for 2024 though, have a look :)
There's slowly declining excess mortality across many age groups. Total number depends somewhat on method
From
https://t.co/taRy8ndXPX