The writer of the damaging article in @wired claims there is no such thing as #LongCovid. It doesn't exist!
How the hell did @wired publish this rubbish by an Associate Professor of Religion? @AlanLevinovitz
Please rectify! @WIRED
https://t.co/HazEZH6Yg7
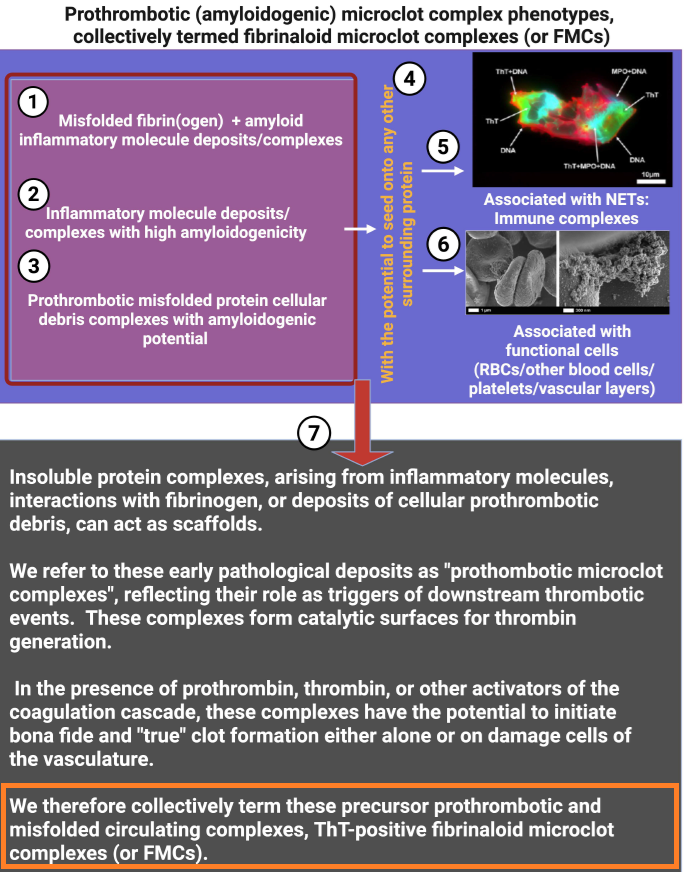
Surface cues shape procoagulant properties of amyloidogenic microclots
🚨YOUR ATTENTION: FMCs!
➡️This EVOLUTIONARY review synthesizes how cell-membrane surface changes during inflammation and cell death drive the formation of procoagulant, amyloidogenic microclots termed fibrinaloid microclot complexes (FMCs).
➡️FMCs are heterogeneous (1–200 μm), Thioflavin T (ThT)-positive complexes of fibrinogen, serum amyloid A (SAA), von Willebrand factor, neutrophil extracellular traps (NETs), and cellular debris/microparticles.
➡️The exceptional article introduces FMCs as a unifying conceptual framework that elegantly integrates membrane biophysics, protein misfolding, and coagulation, previously viewed in isolation, into a single membrane-centric model of thrombo-inflammation. Science, step by step!
➡️Its novelty lies in distinguishing these amyloidogenic, fibrinolysis-resistant complexes from both microparticles and canonical clots, while providing mechanistic evidence (PS exposure, SAA/fibrinogen cross-seeding, ThT positivity) for their role across inflammatory and post-infectious diseases.
➡️🤔By positioning FMCs as both pathological drivers and potential biomarkers/therapeutic targets (e.g, via anti-misfolding or NET-clearing strategies), the work offers a transformative lens for understanding and treating hypercoagulability in Long COVID and related syndromes, with broad implications for vascular medicine.
‼️In conclusion, this exceptional review offers a simple new way to understand how damaged cell surfaces during inflammation create tough, sticky microclots that clog blood vessels and drive long-lasting problems like those seen in Long COVID, opening the door to better tests and treatments that could help millions.
GREAT WORK, Thank you @resiapretorius https://t.co/ZHWPHNagnC and your additional explanation fig’s are really excellent!
https://t.co/meEfHpVcrS
‼️⚠️Please read this until the end.
A widely shared article has presented a deeply misleading view of Long COVID, suggesting once again that cognitive behavioral therapy, exercise, and “mind-body” approaches may be the uncomfortable truth patients refuse to accept.
This needs to be challenged.
Not because the nervous system does not matter.
Not because psychological support cannot help.
But because confusing support with cure, physiology with psychology, and heterogeneity with “it might be in your head” is exactly how medicine has harmed post-infectious patients for decades.
There are articles about Long COVID that look like science journalism, but in reality they repackage, in modern language, a very old idea: if we do not fully understand a disease, maybe the problem is in the patient’s mind.
And that is not science. That is repeating history.
The article begins with a striking sentence:
“There isn’t a single approved pharmaceutical treatment, not even a test to verify the presence of the illness.”
This may sound forceful, but it is a very misleading way of presenting the problem.
The fact that there is still no drug specifically approved for Long COVID, or a single diagnostic test, does not mean that “nothing has been found.” It means that we are dealing with a heterogeneous disease, probably with several biological subgroups, and that medicine has not yet converted those findings into validated clinical tools.
“No single diagnostic biomarker” is not the same as “no biology.”
In just a few years, immunological, vascular, neurological, endocrine, and metabolic abnormalities have been described in subgroups of Long COVID patients: autonomic dysfunction, herpesvirus reactivations such as EBV/HHV-6, alterations in the cortisol axis, autoantibodies against GPCR receptors — including adrenergic and muscarinic receptors — persistent viral antigens, endothelial damage, muscle abnormalities after exertion, mitochondrial dysfunction, persistent inflammation, and differential immune changes.
Is everything settled? No.
Does that mean it is psychological? Also no.
Science does not work like that. Multiple sclerosis did not stop existing before we had MRI. Many autoimmune diseases do not show up in routine blood tests. If a complete blood count, a basic biochemistry panel, or an X-ray comes back “normal, normal, normal,” that does not prove the absence of disease. It only proves that you are looking with inadequate tools.
One of the article’s most serious mistakes is this: it confuses the absence of a simple clinical test with the absence of organic disease.
And that mistake has caused harm for decades.
The article also says:
“Almost $2 billion and half a decade of international effort have yielded little more than hypotheses about micro blood clots and spike proteins and mitochondrial dysfunction.”
No. That is not correct.
A hypothesis is a provisional explanation. But when you compare patients and controls and find significant differences in muscle tissue, metabolism, response to exertion, immune biomarkers, viral antigens, autoantibodies, or vascular dysfunction, you are no longer talking about “little more than hypotheses.” You are talking about lines of biomedical evidence that still need to be organized, replicated, stratified, and translated into treatments.
That is not scientific failure. That is research into a complex and new disease.
🔵Continued in the next post.👇🏻
(1/6)
Wordt Ernst van Koesveld gevraagd waarom dossier #LongCovid telkens in een onderste la verdween? Hij was DG Langdurige Zorg (sept 2019 - sept 2023). Dus onder Conny Helder, minister LZ&S (jan 2022 - feb 2024) die blijkbaar niet wordt opgeroepen🙄.
#PAIS#PECorona
1) This video shows a unique care unit in Norway called Røysumtunet for people with #severeME & very severe ME.
It is one of the only places where the sickest patients can receive specialised care.
We need this everywhere!!
#pwme#myalgicE#millionsmissing#severeME
@WijersR De vragen zijn allesbepalend. Ik hoop maar dat het 'begin van de pandemie' weekthema ruimte biedt om het negeren van langetermijn gezondheidsschade aan te kaarten.
https://t.co/Ckuhw8K8gx
Van Dissel: "ik ga niet over Long Covid"
Dan moeten alle alarmbellen afgaan. Dé corona-adviseur van de regering vindt langetermijn gezondheidseffecten van het virus niet relevant voor beleidskeuzes.
Dat is grove nalatigheid. En massa's patiënten betalen daar nu de prijs voor.
Deze week #peCorona thema 'begin pandemie' met o.a Jaap van Dissel.
Wordt gevraagd waarom #LongCovid pas mei 2023 serieuzer aan de orde kwam in het OMT? Ondanks alle waarschuwingen en kennis van toen (die er wel degelijk was)?
Zie artikel Parool:
https://t.co/HdDFgBGLB7
@AlanLevinovitz@James6939710330@angryhacademic Thank you. Have you also reviewed the answer to Saris and presented it to the exercise physios you selected?
... "However, we strongly encourage Saris and colleagues not to draw causal conclusions that were not evidenced or supported by our work." ...
https://t.co/msjez32CDS
Dit zouden Kuipers en Bruijn nooit over Long Covid gezegd hebben, noch de ambtenaren in de brieven. Dus hopen en aandringen op koerswijziging. Dat VWS daadwerkelijk actie neemt en niet sust en zich beperkt tot dat wat keihard afgedwongen wordt.
Het onderzoeksbudget is NU op.
Long Covid bij de begroting VWS. Amendement @JulianBushoff: 3 milioen C support, 3 miljoen om tot reguliere zorgaanbod te komen. Eenmalig in 2027. Oordeel kamer.
Maar ook het gedeelde uitgesproken besef dat er meer nodig is. Langjarige inzet voor onderzoek en betere zorg.
Voor de duidelijkheid: vml minister Bruijn deed wel voor de bühne deze uitspraak op het malieveld bij het PAIS protest 👇. In het debat een heel andere toon: ga maar je huisarts met je complexe multisysteemziekte. Hetzelfde verhaal als Kuipers en de brieven van ambtenaren.
4 maanden geleden nam de oppositie deze motie aan: voortbestaan expertisecentra Long Covid.
Nog altijd niks vanuit @MinVWS over of en hoe ze dit gaan uitvoeren.
Met die constante onzekerheid jagen ze artsen en onderzoekers NU weg. Want ja, het onderzoeksgeld is ook op, zonder uitzicht op actie vanuit VWS.
Hoe dan ook geldverbrandende kortzichtigheid.
Gaan we het in de brief voor de zomer of pas op prinsjesdag horen? Of ze nou wel of niet, tegen de democratische meerderheid in, het enige medische zorgaanbod en de broodnodige kennisopbouw na dit jaar wegbezuinigen?
🧵OF KEY CONCERNS
We've now read Alan Levinovitz's WIRED piece on Long Covid.
Our concern isn't that it discusses psychological theories.
Our concern is that it repeatedly conflates criticism of evidence with creating a "climate of fear".
Those are not the same thing. /1
🟦 POSTCOVID 🟥 BELANGRIJKE CORRECTIE OP TNO-RAPPORT
🟧 berichtgeving zojuist van de Volkskrant: ‘ongelukkige schrijffouten’
⬛️ link naar het rapport 👉 https://t.co/bgzXo2RK7Y
⬛️ link naar rectificatie TNO 👉 https://t.co/zcnvl0wlEh
@BetterS460@EllenLuxnova1@TNO_nieuws@AnilvanderZee "De onjuistheid en twee onduidelijkheden in de TNO-programmarapportage [...] worden aangepast en tot die tijd wordt het rapport offline gehaald. Het ministerie is hierover op de hoogte gebracht en over deze rectificatie wordt door hen ook gecommuniceerd naar de Tweede Kamer."
Gut. @TNO_nieuws rectificeert TNO-programmarapportage Post-COVID [#LongCovid]
Wegens 'ongelukkige schrijffouten' 🤡
https://t.co/i3XukARZgh
Is dat afdoende? Neen. Zie de reactie van @AnilvanderZee op LinkedIn:
https://t.co/DRcd4jgrbZ
1) This paper provides the a structured, transdisciplinary care guide for people with #severeME in home settings.
The guide fills a major gap in professional knowledge and supports both family caregivers and health professionals in delivering safe, stabilizing care for people