Med students, listen up! Today let me explain how to analyze a Liver Function Test (LFT) step by step.
Stop looking at isolated HIGH or LOW flags on a lab report. You need to look at the patterns. Here is how you actually read an LFT panel like a CONSULTANT 👇 (1/10)
Interesting one for my radiology colleagues.
Reliably labelling the L5 vertebra for interventional treatment planning without whole spine imaging (counting down from C2) is not straightforward given how common lumbosacral transitional anatomy is (sacralisation/lumbarisation).
Paper proposes using the exiting L5 nerve root as a landmark to identify the true anatomical L5.
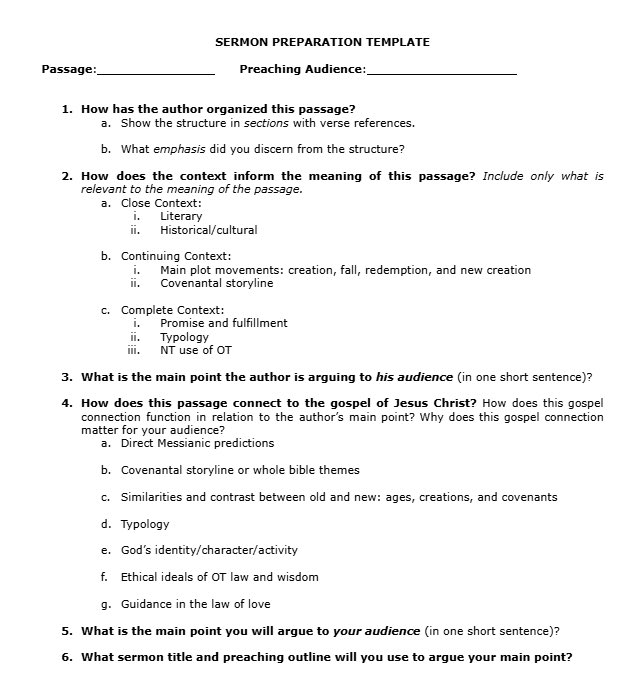
I’ve spent a few years tweaking my sermon prep process to be more balanced, efficient, clear, and replicable. The images below show the sermon prep template I’ve been using for the past year ( which has been really enjoyable and helpful to me).
I use the same 7 questions from the @simeontrust worksheets, but have added helpful insights I’ve gained from:
1️⃣ @jasonderouchie & @AndyNaselli’s helpful books “How to Understand and Apply the OT/NT: Twelve Steps from Exegesis to Theology.”
2️⃣Steve Wellum and @TrentHunter’s “Christ from Beginning to End”
3️⃣ @dandoriani’s excellent book on application “Putting the Truth to Work.” My chart is a summary of his main ideas.
4️⃣ @jeremypierre’s excellent work “The Dynamic Heart in Daily Life.” The heart image comes from his book.
5️⃣As for sermon outline and delivery, @tonymerida’s “Christ-Centered Expositor” has shaped me most.
@NickIlic_Physio Good point
It's from
Schirmer CM, Shils JL, Arle JE, Cosgrove GR, Dempsey PK, Tarlov E, et al. Heuristic map of myotomal innervation in humans using direct intraoperative nerve root stimulation. J Neurosurg Spine. July 2011;15(1):64-70.
Also more here: https://t.co/GXf4X2S4RE
I don’t know where I saved this handy reference pic from, but it’s a useful reminder of the overlap in lumbar motor innervation.
An L5 nerve root lesion won’t “wipe out” ankle dorsiflexion — it’s more likely to make it significantly weaker, because L4/S1 still contribute (~50%).
Hey @BBCSport could you just make a slight tweak to your website to make it even better? When I look at any football league table and you have the 'form' column (W/D/L), when you mouse over the 'W/D/L' please can you have it so it pops up with what the game/score was? thanks!
New article. Navigating the grey zone regarding surgery for disc herniation and sciatica! Feedback appreciated (I know it's long).
https://t.co/OhjCsVm3Wi
The hardest conversation I have in my office isn't about surgery. It's about time.
A 58-year-old sat across from me with knee pain. She’s otherwise healthy, but menopause has been rough on her. Her MRI shows some cartilage changes — age-appropriate, and a typical meniscus tear... basically, nothing that requires surgery. But she hasn't done any physical work in 15 years. She stopped playing tennis at 43. Stopped walking regularly at 50. Now the knee hurts when she climbs stairs.
The knee isn't the problem. The knee is just the messenger.
What has really happened is fifteen years of progressive capacity loss. Muscle mass has declined while tendon capacity has dropped. Her metabolic health shifted, and menopause has contributed to these changes. The knee was affected secondarily. The knee doesn't require my attention... that needs to be directed elsewhere.
I can't give her those fifteen years back, but I can help her start from where she is. And starting from where she is still works.
An 85-year-old can still synthesize new muscle protein after a single resistance-training session. The window of opportunity does narrow with age, but it never closes. Recovery takes longer. The risk of injury is likely higher. Progress is slower. But the biology of adaptation doesn't abandon you at 58, or 68, or 78.
What changes is the cost of waiting. Every year of inactivity makes the starting point harder and the ceiling lower. The leverage you have at 40 is real and significant — and it's greater than the leverage you'll have at 60.
That's not a reason for despair... It's a reason to start, wherever you find yourself now.
3 months later, after a solid strength/power program, she's walking daily with her weighted vest and is back on the tennis court.
In resident clinic, the patient says:
“I’m off balance.”
One sentence.
A problem that could live anywhere on the neuroaxis.
When the exam doesn’t scream cerebellum, vestibular, or spine—that’s when I reach for my neuromuscular buckets.
Woman, 52.
Doctor, I think I'm getting Alzheimer's.
She's not.
She's in perimenopause and nobody told her this is neurological.
Menopause = Brain event, not just ovarian.
Here's your complete OPD cheat sheet:
↓ What to screen (4 pillars)
↓ Brain fog vs dementia
↓ HRT vs non-hormonal Rx
↓ Clinical pearls
Save this.
#MedTwitter #NeurologyTwitter #WomensHealth #Menopause