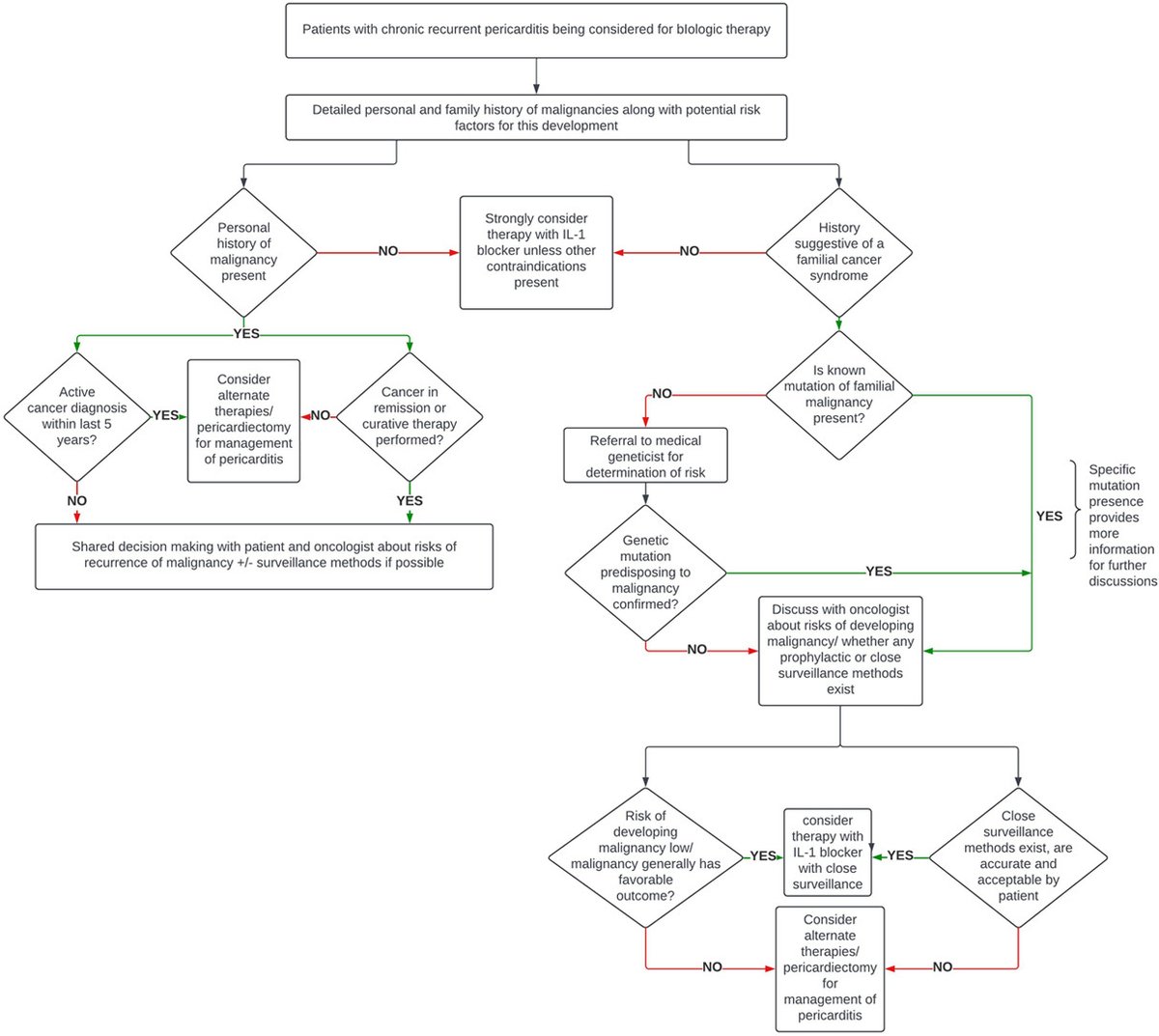
🩺 Managing pericarditis in patients with cancer risk? #CardioOnc
Don’t let risk hold back treatment. Our latest manuscript provides a new framework to guide biologic therapy decision-making and ensure viable options for RP patients.
Read more: https://t.co/rhh2POZxs7
Explore practical and advanced multimodality imaging—echo, nuclear, CT, and CMR—to support diagnosis, risk stratification, and management across cardiovascular disease in modern #cvImaging and #Cardiology practice: https://t.co/WvppVXlleV @DrAmyPollak@PanithayaC
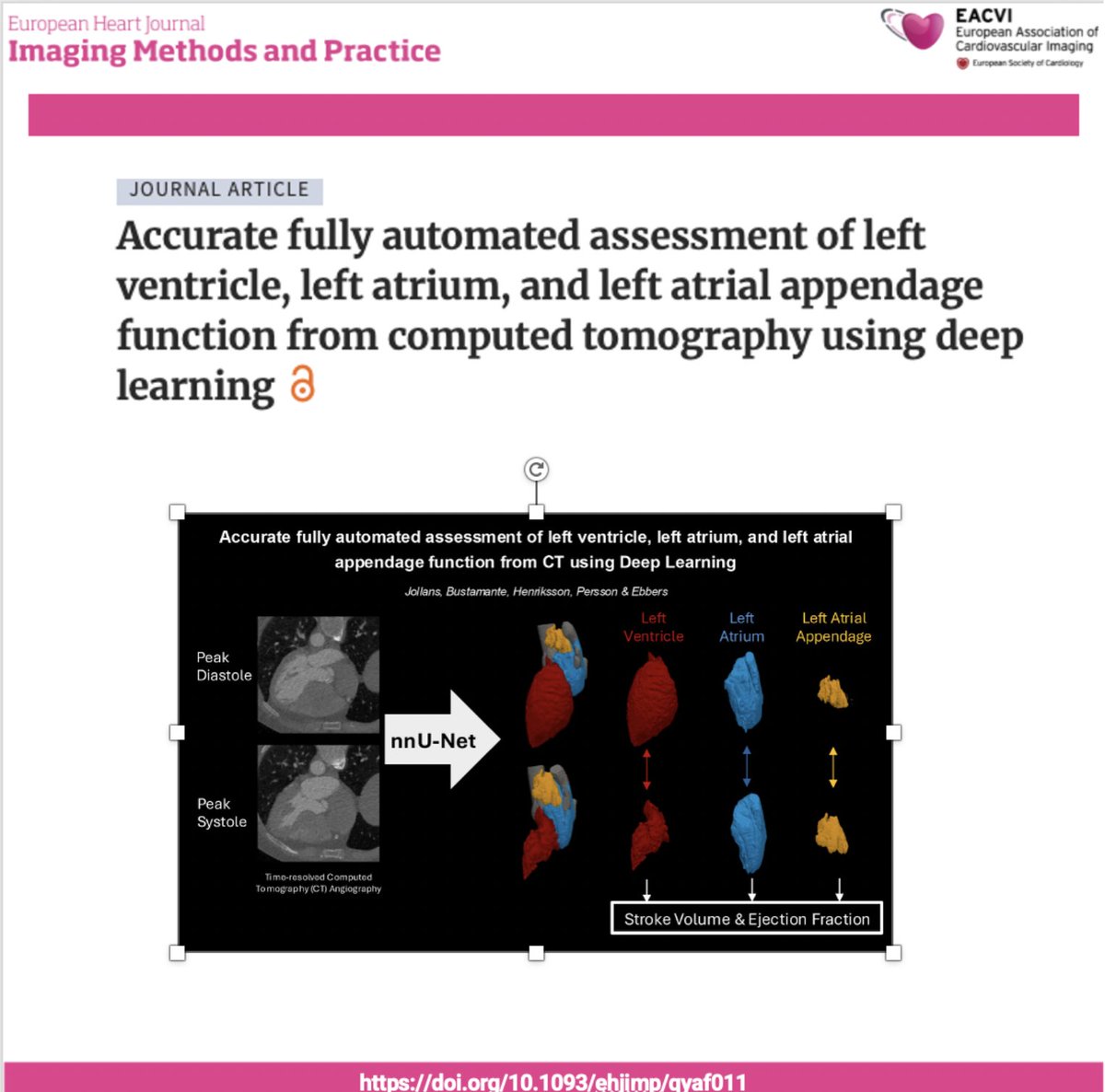
📢 New study! 🤖🫀 A deep learning model can fully automatically quantify LV, LA & LAA function from CT scans, offering fast, reliable measures of cardiac volumes and ejection metrics — boosting reproducibility and reducing manual effort in heart function assessment. 🩺🧠
#EHJIMP #CardioAI #CTimaging #HeartFunction #AIinMedicine @jgrapsa@saramoscatelli7@alessia_gimelli@EHJIMPEiC@EACVIPresident https://t.co/10n1QnyrpP
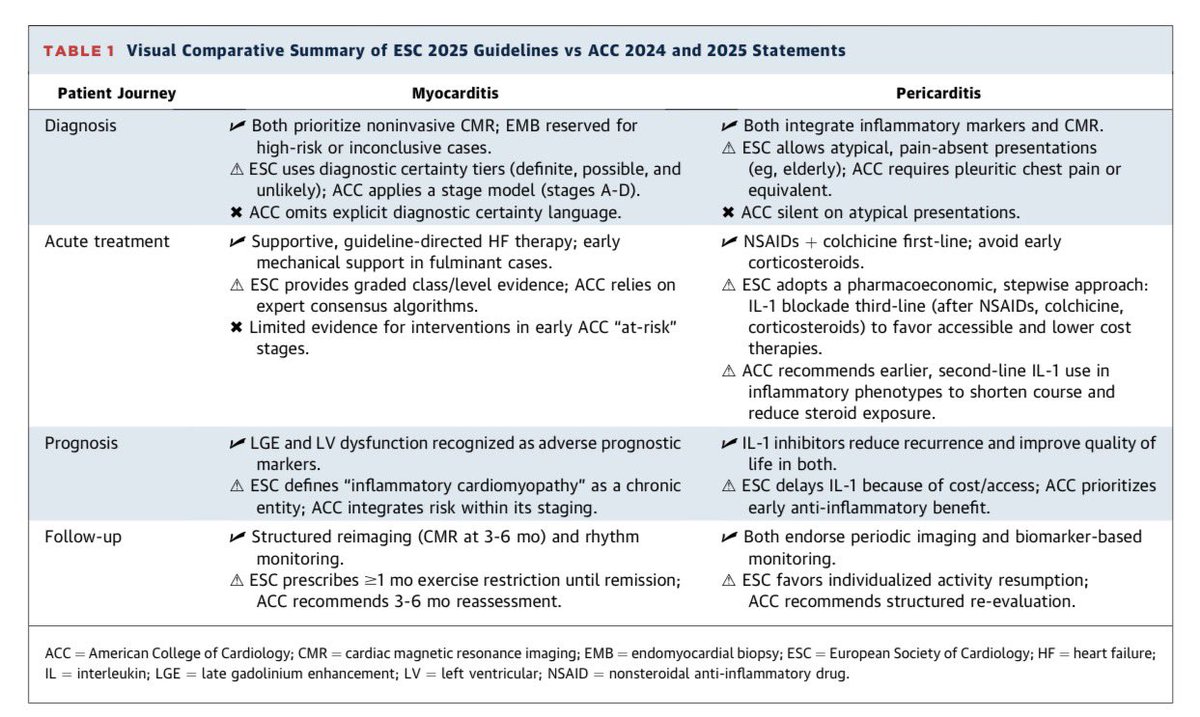
Myocarditis and Pericarditis in Focus
A Brief Report Comparing the 2025 ESC Guidelines and Latest ACC Position Papers. Learn more in J Am Coll Cardiol
2025 Nov 19:S0735-1097(25)10033-8.
doi: 10.1016/j.jacc.2025.10.047
Quantitative Coronary Plaque Analysis (QCPA): promise, but also important pitfalls — a critical reading of the 2025 ACC Scientific Statement
The 2025 ACC Scientific Statement on Quantitative Coronary Plaque Analysis (QCPA) is an important step toward integrating AI-driven plaque quantification into clinical cardiology. However, the document also implicitly reveals several major weaknesses and unresolved pitfalls that deserve explicit attention before widespread adoption .
1. Reproducibility across platforms remains a major Achilles’ heel
QCPA results are not interchangeable across vendors or software versions. Different algorithms use distinct lumen–wall segmentation methods, HU thresholds, training datasets, and post-processing rules. As a result, total plaque volume and plaque composition can differ substantially between platforms—even when analyzing the same scan. True cross-vendor standardization is still lacking.
2. CT acquisition parameters strongly influence plaque quantification
Plaque volumes and composition are highly sensitive to scan parameters, including:
Tube voltage (kVp)
Reconstruction kernel and slice thickness
Iterative vs deep-learning reconstruction
Scanner generation (energy-integrating vs photon-counting CT)
Small technical differences can translate into artificial changes in plaque volume or composition, particularly for non-calcified and low-attenuation plaque—precisely the components most often linked to risk.
3. Serial QCPA is biologically appealing but methodologically fragile
The statement rightly discourages routine serial QCPA. Even with the same patient, apparent plaque “progression” may reflect technical variability rather than biology, unless acquisition and reconstruction are rigorously matched. Proposed progression thresholds (e.g. ΔTPV 10–20 mm³/year) remain expert opinion, not outcome-validated cut-offs.
4. Risk of overcalling subvisual plaque
This is particularly tricky since conventional CT technology (with few exception in the current market namely Cleerly) is not able to properly set the lower threshold for normal coronary artery wall volume.
AI-based QCPA frequently detects plaque volumes below visual thresholds. The clinical significance of minimal plaque (<20–30 mm³) is unknown and risks overdiagnosis, overtreatment, and patient anxiety, especially in low-risk populations.
5. Outcome evidence is still indirect
While plaque burden correlates with risk, no randomized trial has yet demonstrated that QCPA-guided management improves outcomes beyond standard CTA interpretation, CAC scoring, and clinical risk assessment.
Bottom line:
QCPA is a powerful research and risk-phenotyping tool, but today it remains technically sensitive, platform-dependent, and insufficiently standardized. Until reproducibility, calibration, and outcome validation improve, QCPA should be used selectively, cautiously, and always interpreted in clinical context—not as a standalone decision-maker.
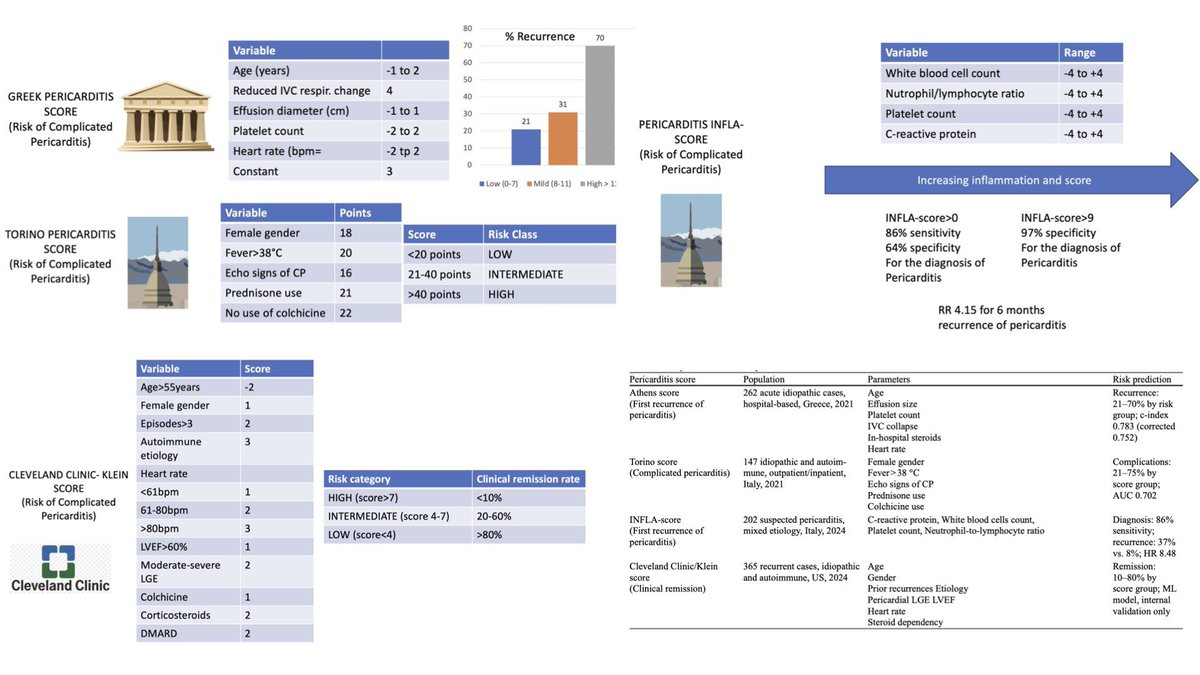
Scoring Systems for Pericarditis: A Step Toward Structured Risk Stratification. Learn more on Current Cardiology Reports (2025) 27:101. https://t.co/e7d6fZhwoI
SLDA during tTEER presents a sig. procedural challenge but can be managed effectively with clip retrieval using the EN Snare & ŌNŌ devices. Both cases demonstrated successful clip retrieval w/out injury to valve leaflets & successful #TEER https://t.co/HSKLqJo5tQ #JACCCaseReports
Loose tricuspid SLDA? ONO facilitated retrieval: https://t.co/FXpBQNjWwq
ONO basket allows stand up of snared clip vertically allowing smooth retrieval into sheath without getting stuck perpendicularly at sheath entry/injury to vein @SinaOSullivan@mirvatalasnag@DrPeterPollak
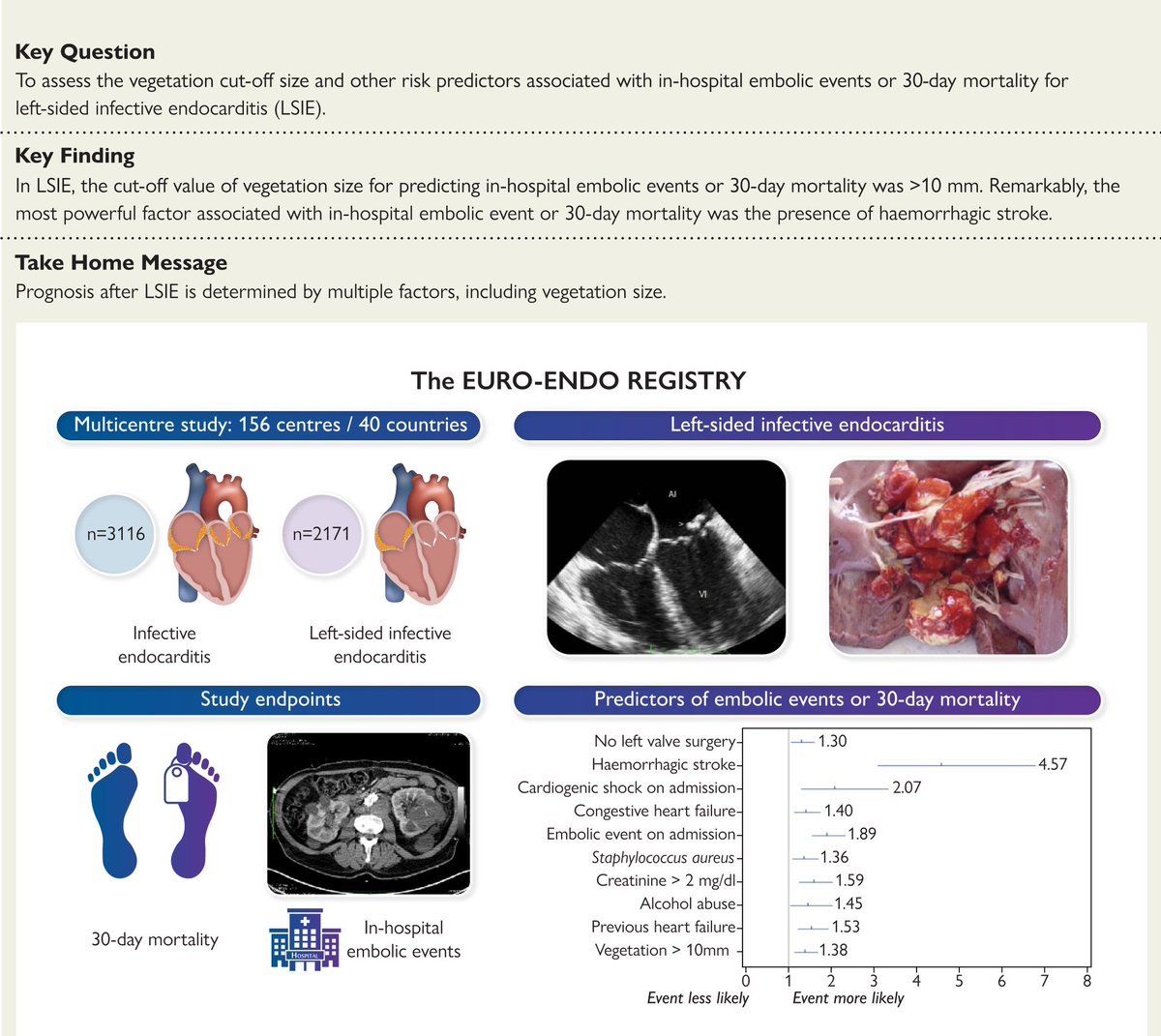
In this #BeyondtheData, Mamas Mamas (@mmamas1973), Abdallah El Sabbagh (@aelsab), and Julia Grapsa (@JGrapsa), discuss how mechanical aspiration can be used in infective endocarditis treatment, as seen in the CLEAR-IE study. #tct2024 Watch the full video: https://t.co/7famvKZfGi
Read the new #JACCIMG international position statement on multimodality #cvImaging for #pericardial disease evaluation & treatment (pericarditis, effusion, constriction, & masses). https://t.co/AnRhvp7yVI
#Echofirst#YesCCT#whyCMR
We are committed to moving the conversation forward in TAVR and have partnered with experts in 4D MRI to study the flow patterns post-TAVR compared to the healthy aortic valve. Restoration of laminar flow is associated with favorable reverse remodeling.(1)
Listen to Dr. João Cavalcante’s presentation on flow patterns and restoration of laminar flow with the novel DurAVR™ valve: https://t.co/x4qq0ueTUV
#laminarflow #4DMRI #TAVR #TAVI
1. Cavalcante J. Biomimetic Design Restores Flow and Hemodynamics and Leads to Significant LV Mass Regression: update from First-in-Human (FIH) Study with novel DurAVR™ Transcatheter Heart Valve. Oral Presentation at: New York Valves; June 2024; New York, New York.
DurAVR™ INVESTIGATIONAL USE ONLY. NOT AVAILABLE FOR COMMERCIAL SALE.
EU: Exclusively for clinical investigations. US: CAUTION – Investigational Device. Limited by Federal (or United States) law to investigational use.
Which recurrent #pericarditis patients should have #pericardiectomy and how effective is it? Kevin Greason, MD and S. Allen Luis from @MayoClinic discuss these questions and more on this week's #CardiovascularCME Podcast: https://t.co/O2GHD8YMEj