🧬Inclisiran achieved marked LDL-C reductions at 🗓️90 days in real-world secondary prevention. The therapeutic 🎯, <55 mg/dL (<1.4 mmol/L), was achieved by 64.5%. Experience in 🇮🇨Hosp. Univ. de GC Doctor Negrin. 👁🗨https://t.co/NGevYUkXsV @SoCanCar@preventiva_SEC@unICaDrNegrin
My #ADASciSessions take home messages:
Wall Street needs to listen to Main Street:
Quality of weight loss (read tolerability) will outlast quantity of weight loss
You must not only get the weight off but also keep it off
We will likely end up with induction regimens and different maintenance regimens
Big weight loss may win headlines and Wall Street, but tolerability and affordability will win patients and Main Street.
#cmgsays
Grin. It was a similar story w LAAC. Now two trials have shown disappointing results after 600,000 pts have been treated.
ARNIs not likely harmful, I just question their value in a disease that places a lot of burden on pts.
Why was PARADISE so unimpressive? Similar type of condition.
Having traveled in Europe where value matters I strongly suspect there’d be no problem enrolling. Cc @kaulcsmc@Sensible__Med
An adequately powered RCT to evaluate similar outcomes as PARADIGM-HF would cost ~$300 to $450 million
You would need patients willing to volunteer/consent, investigators willing to randomize, and IRBs willing to approve
When most across the world already see ARNI as Class 1 https://t.co/iwjv0Y4wBe
América Latina no cuenta con un score de riesgo cardiovascular con datos de nuestra región validados.
Junto a @escardio estamos trabajando en la re calibración del SCORE2 en nuestra población
El SCORE2-LAC pronto estará disponible para ayudar a estratificar mejor a nuestros pacientes
Felicitaciones @siacprevent y al @DrPontecarlosi por liderar este proyecto
https://t.co/jD6sIq2BRm
The cardiology community has lost a giant. We honor the extraordinary legacy of Eugene Braunwald, MD, MACC, a visionary leader and pioneer whose outstanding contributions shaped the foundation of cardiovascular medicine as we know it today.
Read more: https://t.co/uaC2n4m5gD
Farewell to Eugene Braunwald... The Godfather of Modern Cardiology
Eulogizing a scientific giant of Eugene Braunwald's caliber does not require ornate words or emotional exaggeration. Rather, it demands a quiet moment of reverence for a career that altered the course of medical history in the treatment of heart disease.
Braunwald was not merely a physician or a researcher; he was the compass that guided successive generations. He transitioned the field of medicine from an era where heart attacks were treated with mere observation and bed rest, into the age of direct intervention and evidence-based therapy. Through his pivotal research—most notably the groundbreaking TIMI trials—and his profound contributions to understanding the pathophysiology of myocardial infarction and heart failure, he granted millions of people a second chance at life.
In every cardiac intensive care unit and catheterization lab, his spirit will remain strongly present. In our libraries, his timeless textbook will endure as a scientific trust and a foundational constitution we rely upon when making the most complex clinical decisions.
The man who listened so intently to the beating of hearts and deciphered their code has passed away, leaving behind an immortal legacy—a legacy that will continue to beat within every patient who regains their health, and within every physician searching for the scientific truth to save a life.
May his soul rest in peace, and may his knowledge endure forever.
وداعاً يوجين براونوالد.. عرّاب طب القلب الحديث
إن رثاء قامة علمية بحجم يوجين براونوالد لا يتطلب كلمات منمقة أو مبالغات عاطفية، بل يستوجب وقفة إجلال هادئة أمام مسيرة غيرت مسار التاريخ الطبي لعلاج أمراض القلب.
لم يكن براونوالد مجرد طبيب أو باحث، بل كان البوصلة التي وجهت أجيالاً متعاقبة. لقد أخذ بالطب من حقبة كانت فيها النوبات القلبية تُعالج بالمراقبة والراحة السريرية، إلى عصر التدخل المباشر والعلاج القائم على الدليل القاطع. من خلال أبحاثه المحورية، وتحديداً تجارب (TIMI) الرائدة، وإسهاماته العميقة في فهم فسيولوجيا احتشاء عضلة القلب وقصورها، منح ملايين البشر فرصة ثانية للحياة.
في كل وحدة رعاية مركزة للقلب، وفي غرف القسطرة، سيظل طيفه حاضراً بقوة. وفي مكتباتنا، سيبقى مرجعه الخالد أمانة علمية ودستوراً نستند إليه في أعقد القرارات السريرية.
لقد رحل الرجل الذي أنصت طويلاً لنبض القلوب ففك شفرتها، وترك خلفه إرثاً لا يموت؛ إرثاً سيظل ينبض في كل مريض يسترد عافيته، وفي كل طبيب يبحث عن الحقيقة العلمية لإنقاذ حياة.
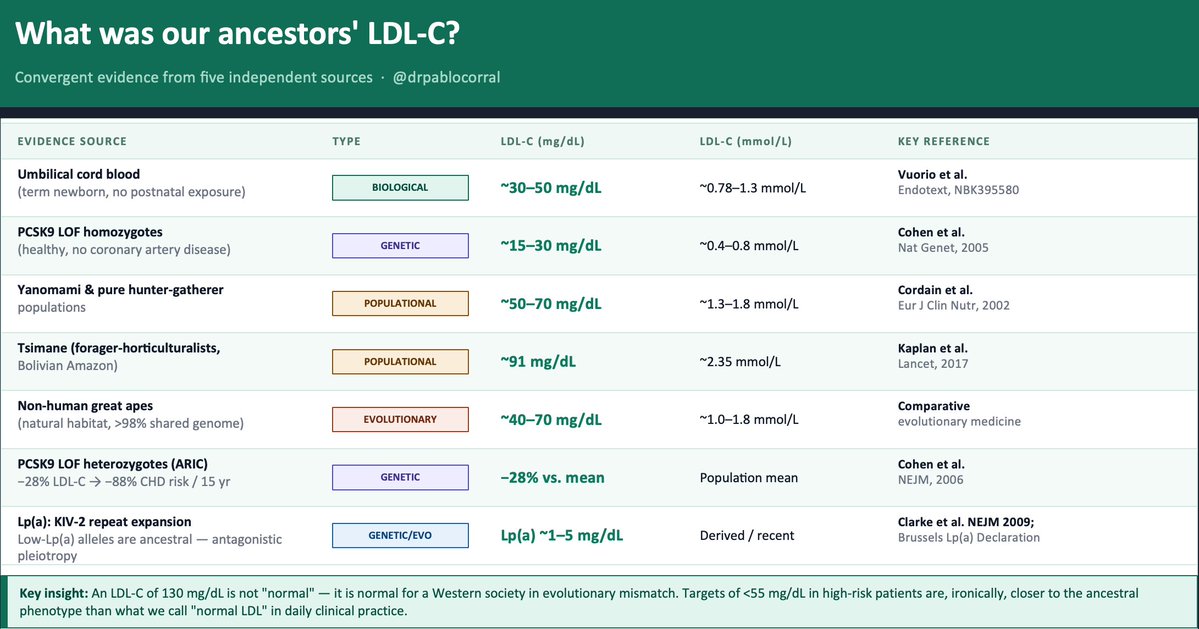
👉 We spend decades arguing about how low to push LDL-C
👆 Almost no one asks the obvious question:
🤔 How much LDL-C did our ancestors actually have?
The evidence exists — five independent lines, all converging on the same uncomfortable answer.
1️⃣ The term newborn. Before any dietary or metabolic influence, a healthy neonate arrives with LDL-C of ~30–50 mg/dL. That is the LDLR operating without environmental interference. Everything that rises after birth is acquired.
2️⃣ The Tsimane (Kaplan et al., Lancet 2017) — forager-horticulturalists of the Bolivian Amazon — have a LDL-C between 70 to 90 mg/dL and the lowest prevalence of coronary atherosclerosis ever recorded in any human population. Five times less than the U.S. in adults over 75. And their LDL is rising as roads and processed food arrive.
3️⃣ PCSK9 loss-of-function variants. African American carriers of nonsense mutations (Y142X/C679X, ~2% frequency): −28% LDL-C and −88% CHD risk over 15 years (Cohen et al., NEJM 2006). Homozygous LOF carriers live with LDL-C of ~15–30 mg/dL. Perfectly healthy. Nature already ran the trial.
4️⃣ Evolutionary genetics. Recent positive selection signals exist on gain-of-function PCSK9 variants that raise LDL-C — likely adaptive in food-scarce ancestral environments. Modern hypercholesterolemia is not "normal." It is an ancestral survival advantage turned pathological by evolutionary mismatch.
5️⃣ Great apes in natural habitat: ~40–70 mg/dL LDL-C. Same genome. Different environment.
👆 Bonus — Lp(a). The KIV-2 repeat expansion that raises Lp(a) is a derived, recent variant. Low-Lp(a) alleles are ancestral. Elevated Lp(a) is a textbook antagonistic pleiotropy signal — possibly protective against bleeding early in life, atherogenic over decades
📍The convergent estimate: ancestral LDL-C was ~30–70 mg/dL.
📍An LDL-C of 130 mg/dL is not "normal." It is normal for a Western society in evolutionary mismatch. Targets of <55 mg/dL in high-risk patients — which still feel aggressive to many clinicians — are, ironically, closer to the ancestral phenotype than what we call "normal LDL" in daily practice.
🤔 The question is not "is it safe to lower LDL this much?"
The question is: why did we let it rise this high?
@society_eas@nationallipid
The cholesterol wars are over.
LDL won.
New guidelines. Four landmark trials. An oral PCSK9 inhibitor that matches injectables. And data proving we should be treating patients we currently aren't.
Here's everything clinicians need to know. 🧵
This is a masterclass in why we need RCTs.
Observational studies were conflicting.
Physiologic rationale made sense.
Industry pushed adoption.
Reimbursement incentivized use.
But when 𝗿𝗶𝗴𝗼𝗿𝗼𝘂𝘀𝗹𝘆 𝘁𝗲𝘀𝘁𝗲𝗱: ❌
How many patients were harmed in the meantime? 🤔
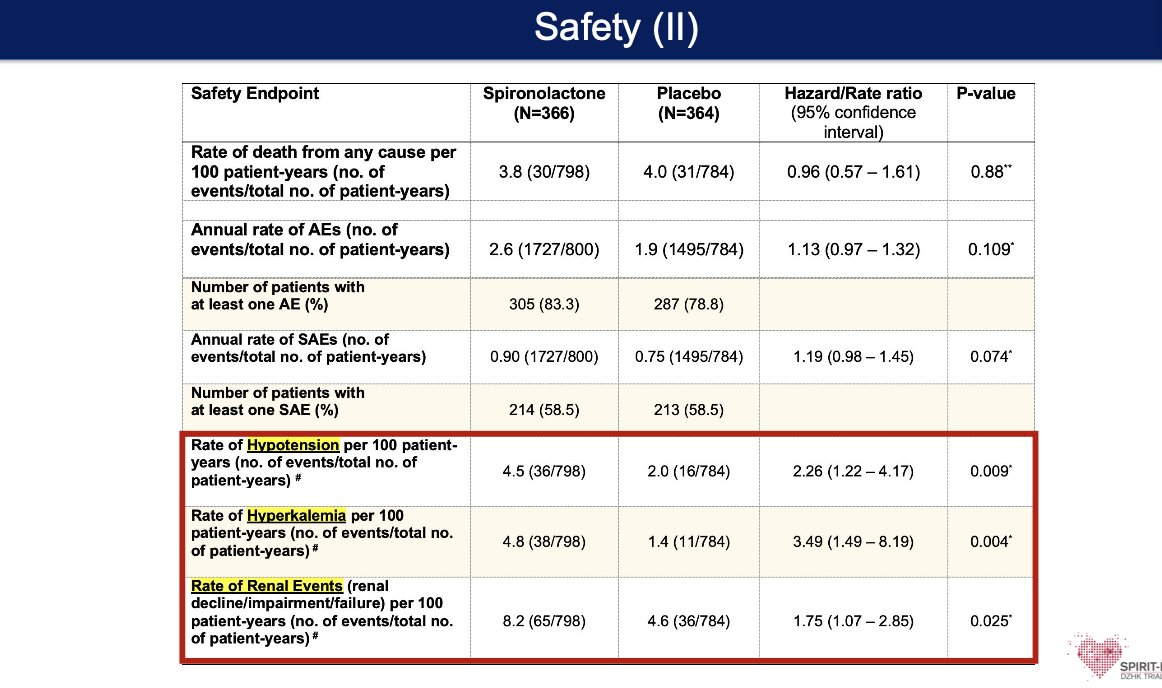
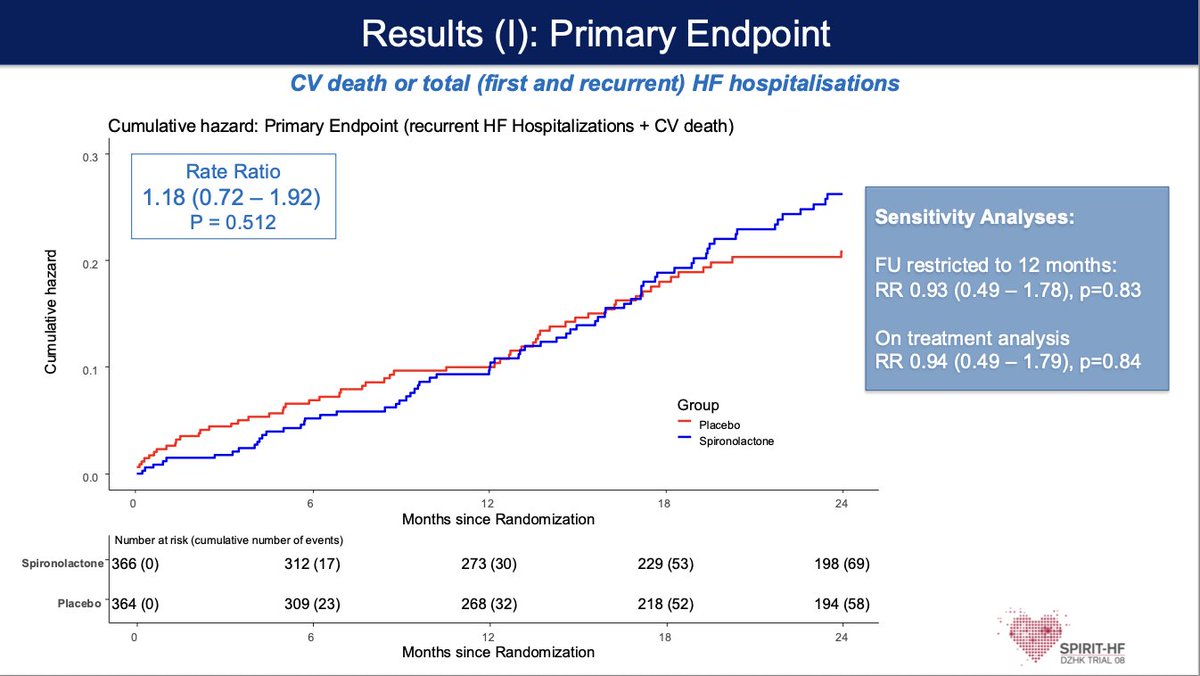
#SPIRIT-HF #ACC26
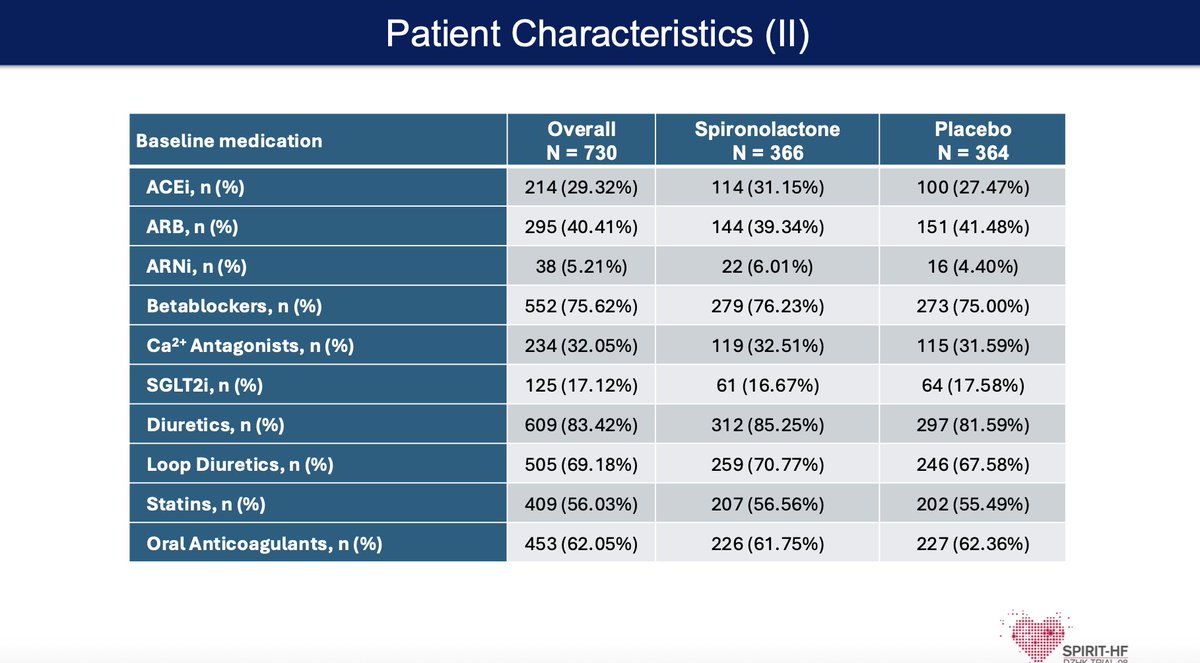
🧑⚕️ HF with preserved or mildly reduced EF (HFpEF/HFmrEF)—a large, underserved group with limited therapies
🧠 Does Spironolactone reduce CV death and HF hospitalizations, building on signals from prior trials like TOPCAT
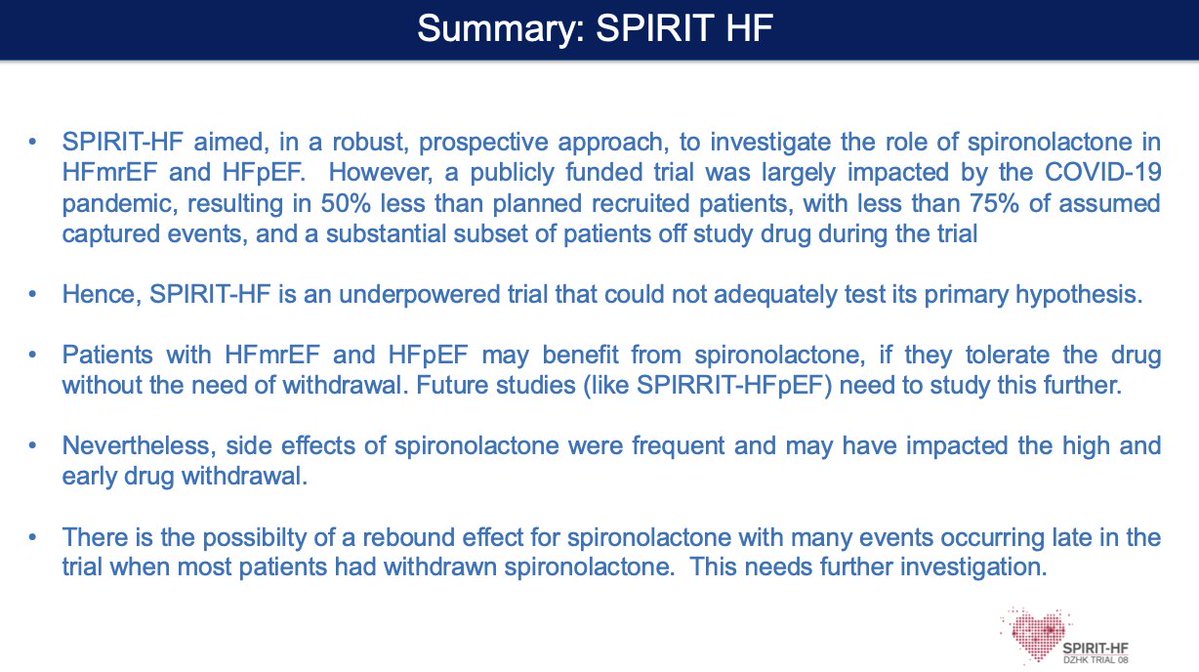
📊 Trial was underpowered (COVID impact, lower enrollment, high drug discontinuation) → unable to definitively test hypothesis
⚠️ No clear primary outcome benefit; side effects and drug withdrawal were common, potentially blunting efficacy
💡 Takeaway:
Signal for benefit may still exist—but tolerability + adherence remain the real barriers in HFpEF therapy
Great Discussion by @dranulala 👏👏
Presented at #ACC26:
Among patients with atherosclerotic cardiovascular disease, targeting an LDL cholesterol level below 55 mg per deciliter led to a lower 3-year risk of cardiovascular events than targeting a level below 70 mg per deciliter. Full Ez-PAVE trial results: https://t.co/q0vNdAoJJL
Editorial: Paving the Road toward Targeted Lipid Lowering https://t.co/zUwmo0r0n4
@ACCinTouch
🚨 Fellows. Residents. Early career cardiologists — listen up.
#ACC26 is NOT just a conference.
It’s a career accelerator 🚀
If you show up right, it can change your trajectory.
Here’s how to MAXIMIZE 🎯every minute 👇
@ACCinTouch@JACCJournals@ACCmediacenter
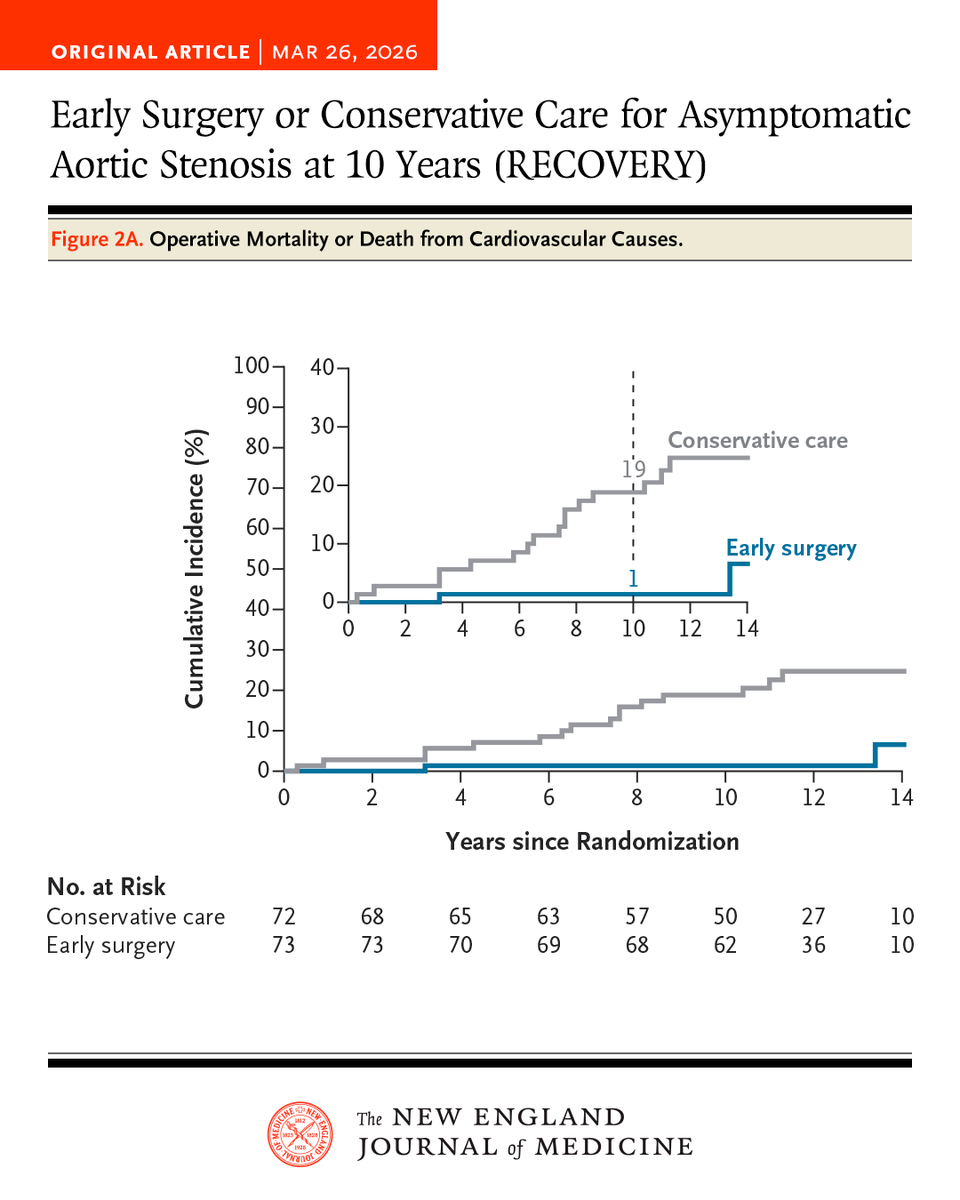
Early surgery in asymptomatic patients with very severe aortic stenosis led to a lower risk of a composite of operative mortality or death from cardiovascular causes at 10 years than conservative care. Full RECOVERY trial results: https://t.co/tLqC25ccCJ
I reviewed one of the most practical guides to literature reviews.
Here are 10 principles that separate average from publishable ones:
⸻
1. A literature review is a positioning document
Before you write anything, answer this:
→ What conversation am I entering?
→ What gap am I clarifying?
If you can’t answer that, you’re not ready to write.
⸻
2. Topic selection is a strategic decision
A strong review topic is:
→ narrow enough to be meaningful
→ broad enough to matter
→ active enough to contribute to
Most students choose topics that are either too safe… or too vague.
⸻
3. Searching is not a one-time activity
Serious reviewers:
→ iterate search terms
→ trace citations forward & backward
→ revisit the search as their thinking evolves
⸻
4. Reading without writing is wasted effort
If you finish reading 30 papers and have no notes…
You’ve retained very little.
Strong reviewers:
→ extract arguments, not just findings
→ write while reading
→ begin synthesis early
⸻
5. Decide your review type intentionally
Narrative, systematic, integrative, meta-analysis…
Each answers a different kind of question.
Confusion here leads to weak methodology and confused writing.
⸻
6. Synthesis is the core skill
Anyone can summarize papers.
Very few can answer:
→ What patterns exist across studies?
→ Where do findings conflict?
→ Why do they differ?
That is what reviewers are looking for.
⸻
7. Critical thinking is non-negotiable
A strong review:
→ identifies methodological weaknesses
→ questions assumptions
→ highlights gaps
⸻
8. Structure reflects clarity of thought
Disorganized reviews are not writing problems.
They are thinking problems.
A clear structure means:
→ logical flow of ideas
→ intentional grouping of evidence
→ a reader who never feels lost
⸻
9. Feedback is part of the process, not the end
Good reviews are:
→ challenged
→ questioned
→ reshaped
⸻
10. The best reviews connect time
Weak reviews focus only on recent papers.
Strong ones:
→ anchor in foundational work
→ integrate recent advances
→ show how the field is evolving
⸻
Hi Everyone -
🥸Here are all the 27 late breaking clinical trials presented at @ACCinTouch (ACC.26) with session number, day, time, and objective.
😱See you in NOLA:
👇👇👇
Hoping this gets better before departure day for #ACC26 but this is crazy at @iah#airport today
No PreTSA open and 240 minute wait in the lines if what is posted is accurate.
Please pay the TSA agents now. They need to pay rent, feed their families. Donations at food banks needed throughout Houston.
Paper of the day: Fundamental Anatomy and its Impact on Clinical Practice: Bachmann's Bundle and Interatrial Conduction (Part I-III)
González-Casal D, Baranchuk A, Sánchez-Quintana D, Cabrera JA. JACC CR doi: 10.1016/j.jaccas.2026.107414.2026 Mar 16:107414
Working with the best