@SimonLo21054188@England That's the expertise of Carlos Queiroz no matter who the opponent is!! He always park the same bus. He was the coach of Iran for the previous three world cups, believe me I know him well.
🔥Hot off the press🔥
1/5
Our new meta (18 trials, n=1,619) on adding ICI to neoadjuvant CRT in pMMR/MSS locally advanced rectal cancer —~90-95% of rectal cancers where ICI monotherapy may not work. Does radiation-induced immune priming change that? 🧵
https://t.co/gx7i5J8ZHW
4/5
Why might short-course win? Possibly more CD8+ TIL infiltration with SCRT vs LCRT (our previous study). Hypofractionation may prime a “hotter” tumor microenvironment for checkpoint blockade. Hypothesis-generating, not proven by these RCTs directly.
Bottom line: chronological age alone is a poor decision tool. A comprehensive geriatric assessment — not a birthday — should guide who gets aggressive therapy.
>50%of HNSCC patients are diagnosed at 65+, yet this group is chronically underrepresented in the trials that shape treatment guidelines. 🔥Our new review in Head & Neck looks at what the evidence on systemic therapy + radiotherapy really shows.🔥
Paper:
https://t.co/9w6IFd18MY
For cisplatin-unfit patients, carboplatin- and cetuximab-based regimens are reasonable alternatives, though results vary across studies. Adding immunotherapy to RT looks safe and feasible (IMPORT trial), but efficacy data specific to older adults remain preliminary.
@NiuSanford@OncoAlert Last thing is, the immunocompromised state by pelvic RT is transient and the lymhocyte depletion recovers after two to three weeks post radiation with even higher CD8+ lymphocytes. So, it would be a clever approach to start IO as the consolidation therapy following CRT.
@NiuSanford@OncoAlert In addition, our systematic review is underway showing no definite OS benefit of adding IO to CRT in pMMR despite many phase 2 studies reporting very high PCR rates. The PCR benefit is limited to SCRT and not LCR so far.
@NiuSanford@Alejogom@OncoAlert 🙏 Better control of distant failure revealed the true benefit of RT in OS. Showing we need both modalities. The median OS is very high, maybe higher than ESOPEC and absolutely higher than TOPGEAR. The question is why the results are better than TOPGEAR?
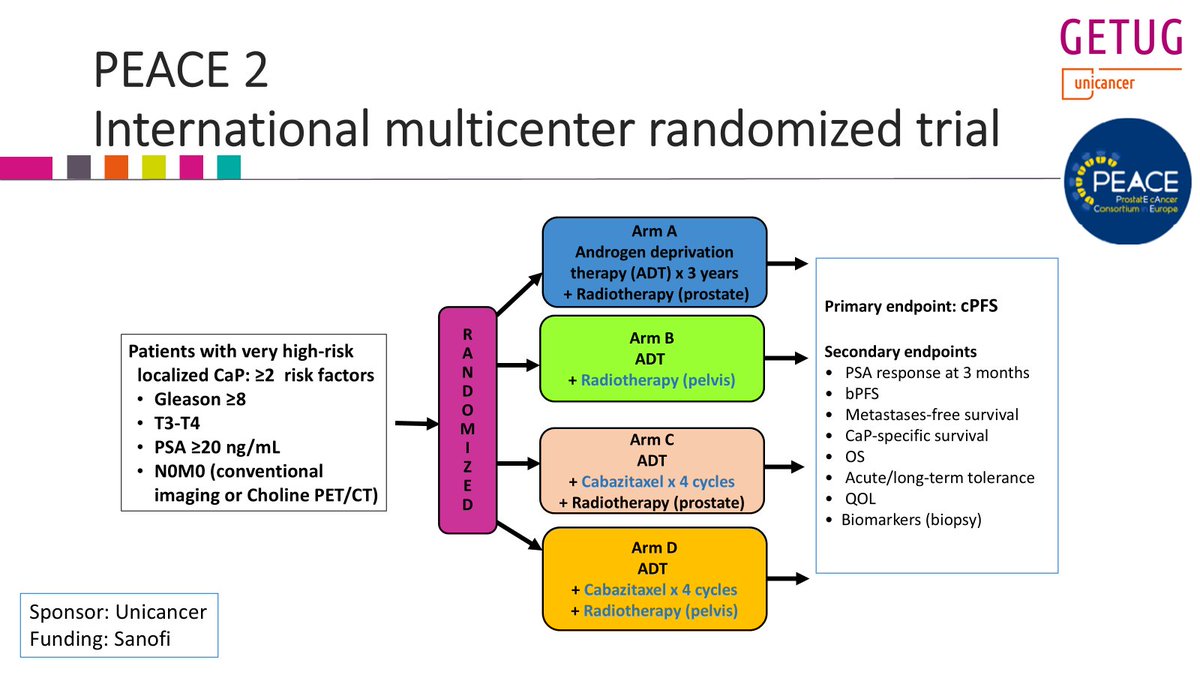
@DrAndrewLoblaw@LuisAlberto3P 80% of POP-RT Pts had PET staging. In PEACE 2, with very high risk pts, many were metastatic already without PET staging.
@PBlanchardMD@RadioterapiaMex How is this come with your presentation of PEACE-2 dear @PBlanchardMD Elective node RT was useless in very high risk but should be done in high-risk? Do you yourself do pelvic RT for PSMA PET negative pelvis in high-risk?
Yesterday, I presented the @GETUG_Unicancer PEACE 2 trial at #ESTRO26 on the role of pelvic RT in very high risk #prostatecancer pts (staged with conventional imaging).
Twittorial below
Key conclusion: pelvic RT did not improve clinical outcomes (cPFS, MFS, PCSS, OS)...
1/n