Here at @RadOncUH we train our residents to become the trailblazers for tomorrow’s standard of care.
@lauren_henke@angela_jia_
Full video here: https://t.co/0cbh6iHggA
One of the best parts of residency is the people 💙 Huge thanks to Dr. Janice Lyons for hosting our residents with Michelin-level food and even better company
A really thought-provoking study at #ASCO26 (Abstr 4512, Clinical Science Symposium): decision regret after adjuvant pembrolizumab in RCC.
🔹 The question
Do patients regret receiving adjuvant pembro — and if so, is it driven by long-term toxicity that CTCAE grading doesn't adequately reflect? They built a patient co-designed tool focused on long-term toxicity.
🔹 The study
104 RCC pts post-adjuvant pembro across 3 London centres, median f/u 30 mo. Pts completed the Ottawa Decision Regret Scale alongside their own rating of irAEs as life-changing, significant, or non-significant.
🔹 What they found
28% rated their toxicity as significant and 11% as life-changing — but these ratings did NOT correlate with CTCAE grade (a third of G1–2 events were rated significant), and regret was identical for G1–2 vs G3–4 irAEs. Regret was driven by patient-perceived long-term toxicity, especially permanent endocrine and MSK irAEs — and not by disease recurrence (only 1/14 who relapsed expressed regret). Lower baseline expectations of toxicity → more regret.
🔹 My take
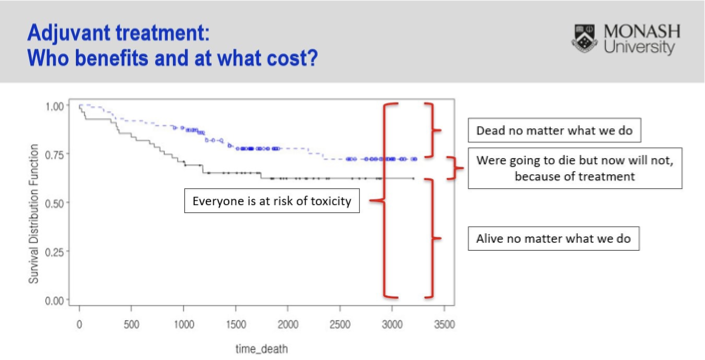
Striking that >1 in 4 reported significant and >1 in 10 life-changing toxicity. What concerns me most isn't that CTCAE missed these events — it's that the grade didn't correlate with how significant patients found them, nor with regret at all. That deviates from the very purpose of grading. The hard part: a regret analysis is tough to contextualize when the alternative, no treatment, risks recurrence — arguably worse than a long-term toxicity. Adjuvant therapy is challenging by nature: most patients are either cured already or destined to recur regardless — we expose everyone to toxicity to benefit a minority. We urgently need biomarkers to find the few who truly benefit. This slide from @Prof_IanD says it all 👇
Looking forward to seeing the presentation!
🔗 https://t.co/laVM7xBbxr
#kcsm #ASCO26
@BethN01@tompowles1
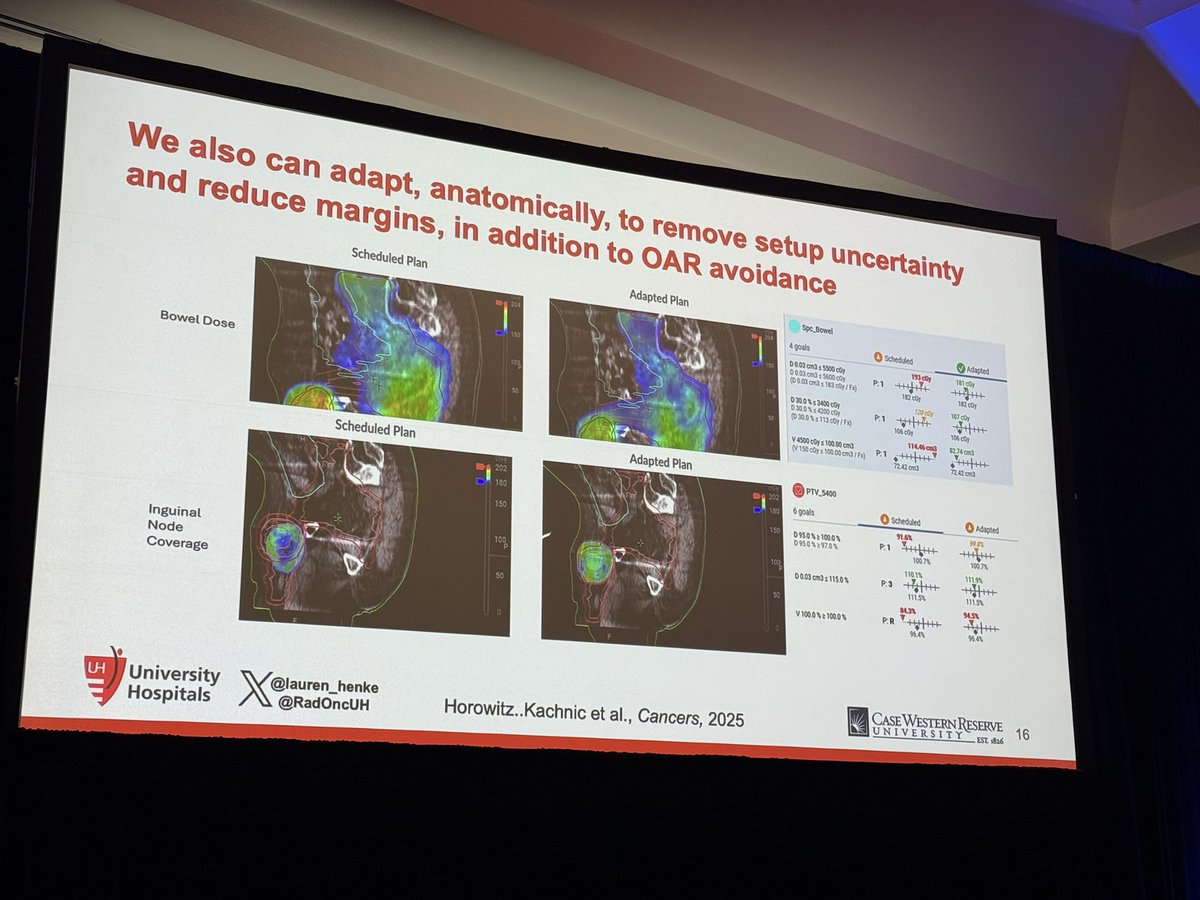
Want to know if you can accurately calculate dose for either offline or online ART using a truebeam hypersight image? You can! HU accuracy to 2%/1mm confirmed across CNS/H&N, thoracic, abdomen, and pelvis prospectively accrued cohorts! Go @KenGreggMP !!
Dear @ESTRO_RT and @Mat_Guc , thank you for letting this crew help you close out another great year! We hope we gave everyone in attendance some food for thought and inspiration for the trip home. And to the Closing Team: mission accomplished. 💫🍾 See you in Milan next year!
Feeling so grateful to have graduated yesterday with so much love and support. Thank you to @angela_jia_ , @DrSpratticus up on stage, the newly minted Dr. @jessica_bai_ graduating with me, and everyone else who has supported me on this journey! Love my #radonc family !!! 💙💚☢️
An amazing theranostics session chaired by Dr. Finkelstein, thanks to Dr. Taunk for answering my questions @NeilTaunkMD. Thrilled about all the advancements in the field. Looking forward to the collaborative efforts of Radiology and Radiation Oncology! @ACR2026
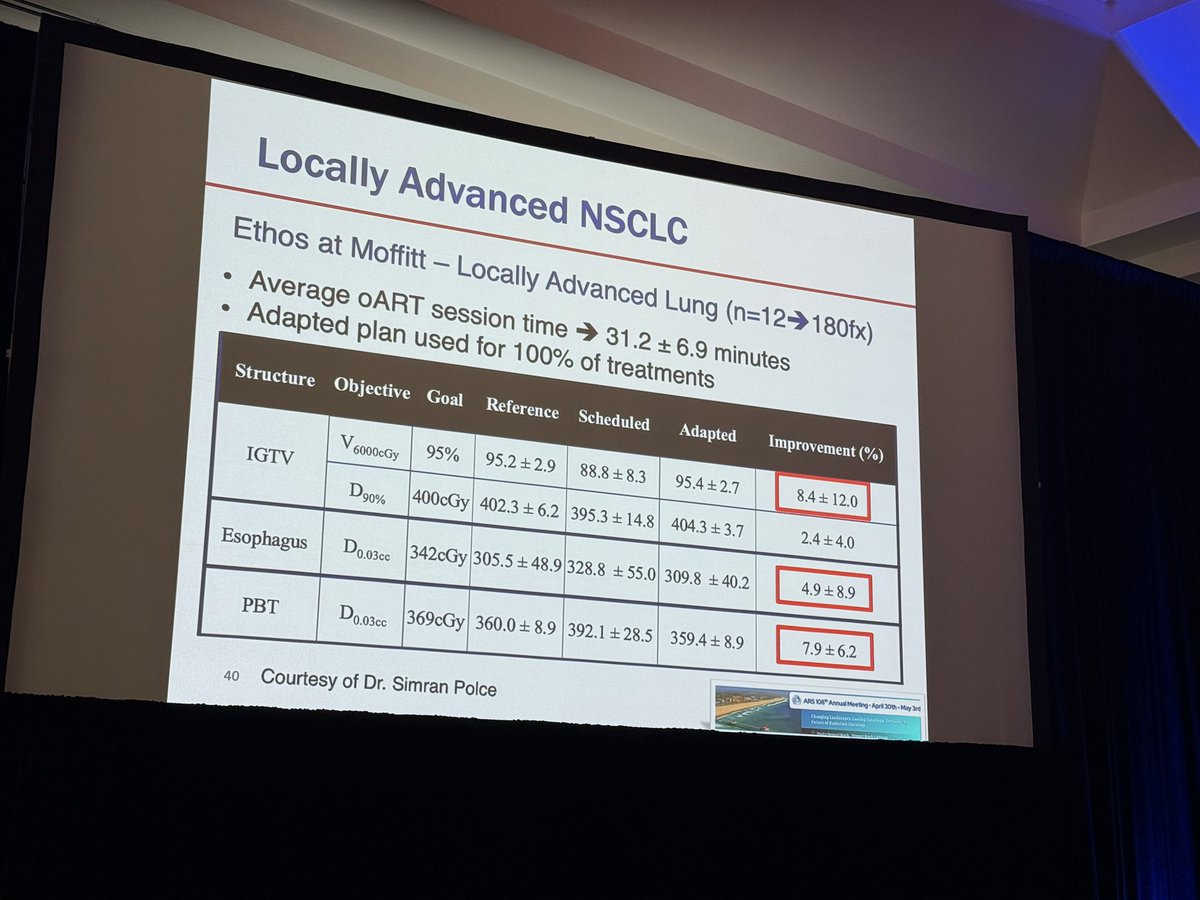
Had so much fun sharing the stage with some leaders in Adaptive Radiation at #ARS2026
One of the coolest parts about being a junior faculty is going from learning from your mentors to sharing the stage with them now as colleagues and friends @lauren_henke
Outstanding #ARS2026 session on Adaptive Radiotherapy by @lauren_henke, @SA_Rosenberg, & @JoshuaSchiffMD highlighting how my two ❤️ imaging🩻 & biology🧫 can ⬆️ the therapeutic window to improve outcomes & ⬇️tox for our patients. @RadiumSociety
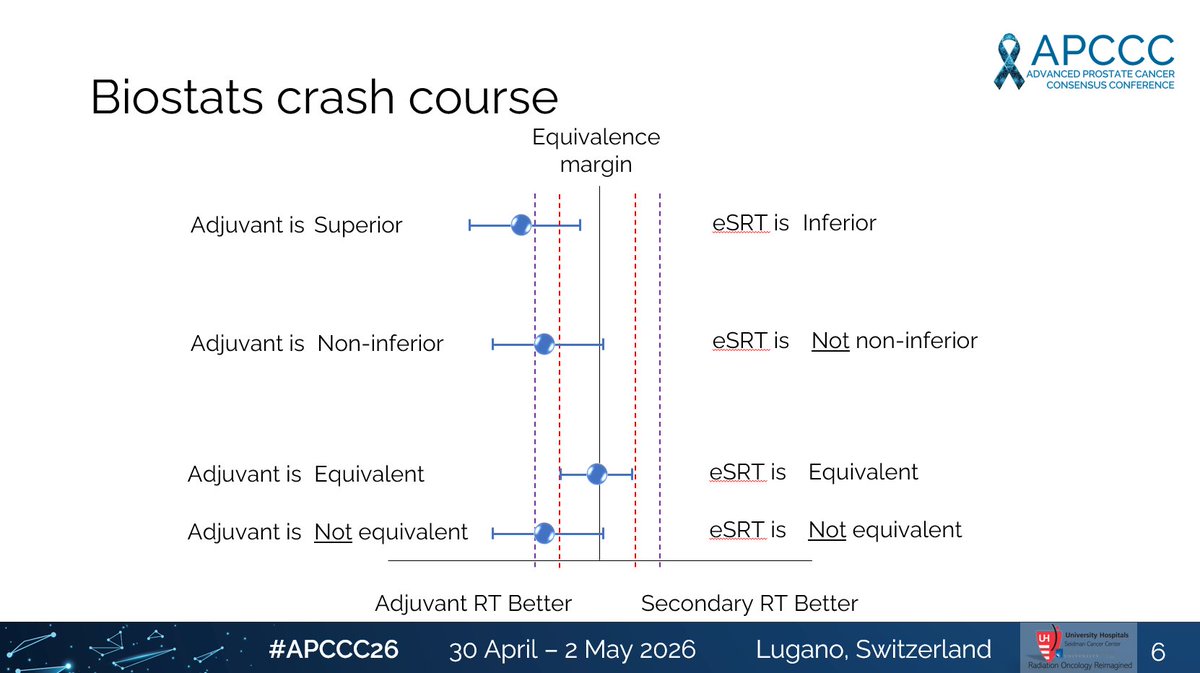
#APCCC26@APCCC_Lugano No one better to debate than @piet_ost
Is early SRT "equivalent" to adjuvant RT in high risk/locally advanced disease? Statistically, absolutely not if you believe the RADICALS-RT data.
@APCCC_Lugano#APCCC26@US_FDA@DrMakaryFDA
This is very important for patients, providers, and regulators to understand. ICECAP showed MFS by conventional imaging is a surrogate endpoint (strong correlation to OS treatment effects and high surrogate threshold effect (STE)).
However, multiple groups have shown that event-free survival (EFS) very closely mirrors PSMA PET/CT MFS. Thus, use of EFS or PET defined MFS have very poor correlation to OS, very low STE, making it nearly impossible for any trial to have a HR low enough for it to serve as a surrogate endpoint for OS.
I hope @DrMakaryFDA and FDA appreciate this. Inhibiting AR will nearly ALWAYS lower PSA. Thus, testoerone suppressed for prolonged period you will near always improve BCR --> EFS --> PSMA PET defined MFS. None of that means you improved outcomes or survival.
@ZEROCancer@PCF_Science
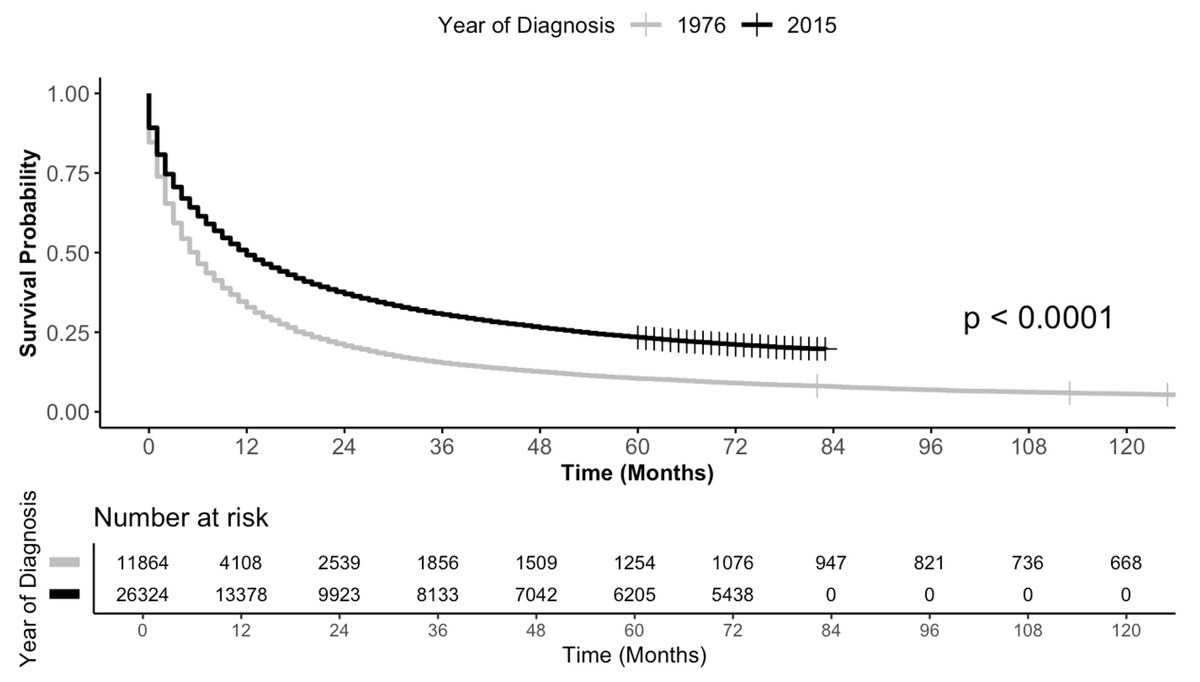
Long-term survival for patients with newly-diagnosed metastatic cancer has more than doubled ⏫in the past 40 years.
However, not all patients live longer.
https://t.co/zNg546hKcc
https://t.co/X6wTFytYPL
Work via @JCOOP_ASCO from team at @UHhospitals@CWRUSOM@MayoClinic
Seriously delightful to host Neil Newman @nbn426 from @UMiamiHealth this morning for an outstanding lecture on HCC for our residents. Neil is always awesome & this was no exception- insightful, engaging, & clinically impactful. Thanks for sharing yourself with @RadOncUH, Neil! 🥳