• ↓ All-cause mortality (RR 0.61, 95% CI 0.47–0.81)
• ↓ Worsening HF events (RR 0.67, 95% CI 0.48–0.94)
• ↓ Cardiovascular death (RR 0.68, 95% CI 0.47–0.99)
• Neutral: HF rehospitalization (trend favorable but not significant)
• No clear increase in AKI
Severe post COVID myocarditis, free TR, mod MR, massive ascitis and pleural effusion, small pericardial effusion, look at the mobile masses, do you know what this is?
Venous vascular pharmacology: how does it contribute to #HFpEF?
This review discusses current literature on the vasoactive effects of #EDRF and #EDCF in the venous vs. arterial systems, in both preclinical and clinical models on #HFpEF
https://t.co/2jjJkp38qn @ESC_Journals
ASE and @accpchest recently partnered on a project to develop two educational webinars to improve the understanding of cardiovascular ultrasound's application in pulmonary hypertension (PH). @chest
You can find them on our Right Heart Resources web page! https://t.co/aHA1IniTS3
@drjohnm
https://t.co/YZqOiAdMHP
TRACK trial lesson: sicker patients ≠ more benefit from treatment.
Statins failed in dialysis. ICD failed in CKD. Now rivaroxaban fails in advanced CKD.
Every therapy has a sweet spot. Outside it, harm beats benefit.
Don't assume. Demand the trial in YOUR population. 📌
🫀Transcatheter MR interventions in #HF are evolving rapidly, but patient selection remains important⚠️
Excellent presentation by @MariannaAdamo1 at #HeartFailure26 on #TEER vs #TMVR:
📍Not all secondary MR is the same:
➡️Ventricular SMR:TEER has strongest evidence (Class I) ➡️Atrial SMR: TEER may be considered after optimization of medical/rhythm control (Class IIb) ➡️Primary MR: TEER for selected high surgical risk patients (Class IIa)
📍Before intervention: optimize HF therapy; GDMT, CRT, AF rhythm/rate control, revascularization when indicated
📍Anatomy matters for TEER suitability Ideal anatomy ≠ very complex anatomy.
Features such as: multisegment lesions, severe calcification, leaflet perforation, rheumatic disease may favor TMVR or alternative strategies
📍TMVR is emerging rapidly, particularly for HF patients unsuitable for TEER & prohibitive surgical risk
📍Heart Team evaluation is crucial
@escardio@EACVIPresident@HFA_President@MarcoMetra
Don’t discharge without checking for residual congestion by ultrasound 👁️ #HeartFailure26
213 acute HF patients: clinical model vs clinical + congestion ultrasound (LUS + VExUS) at discharge
Adding US significantly improved prognostic performance at 3 months:
📈 AUC: 0.80 → 0.85 (DeLong p=0.025)
📈 NRI: 0.27 categorical / 0.73 continuous (p<0.00001)
📈 IDI: 0.08 (p=0.001)
📈 Better model fit (AIC/BIC lower), both models well calibrated
Take-home: Congestion is highly prognostic — and ultrasound assessment at discharge needs to become standard
Torrelles A et al #CardioTwitter #AcuteHeartFailure #POCUS #Congestion #HF2026
More provocative data from Nir Uriel’s presentation on the evolving role of LVADs in advanced heart failure care.
#HeartFailure26
Several analyses presented today showed:
• HeartMate 3 LVAD implantation outperforming transplant listing alone in freedom from death/delisting
• Particularly strong signals in patients aged 50–64
• A growing argument for ‘LVAD bridge first’ strategies in younger patients to extend lifetime therapeutic options
The framing is changing:
Not ‘LVAD vs transplant’
—but how to sequence therapies to maximize total years of survival and quality of life.
Advanced HF care is entering a new era of strategy-driven personalization.”
#HeartFailure #LVAD #HeartMate3 #HeartTransplant #AdvancedHeartFailure #MechanicalCirculatorySupport #Cardiology #TransplantCardiology #ISHLT #MedTech #HealthcareInnovation #MCS #CardiacSurgery #DigitalHealth
“Another key concept from Milton Packer’s talk on obesity-related HFpEF:
The target may not simply be weight loss — but reduction in visceral adiposity and correction of adipokine imbalance.
Therapies including:
• GLP-1 receptor agonists
• SGLT2 inhibitors
• MRAs
• ARNI therapy
• Bariatric surgery
may improve HFpEF in part through favorable effects on visceral fat biology and inflammatory signaling.
This reframes HFpEF as a cardiometabolic disease strongly linked to adipose tissue dysfunction, not just fluid overload or diastolic dysfunction alone. 🫀
#HFpEF #Obesity #CardioMetabolic #HeartFailure #GLP1 #SGLT2 #Cardiology”
#HeartFailure26
💧 Fluids are not benign.
They are pharmacologic interventions with indications, contraindications, dose limits, adverse effects, and cumulative toxicity.
“If hypotensive, give more fluid.” 😬
The paper highlights five classic pitfalls in fluid therapy that most intensivists encounter daily:
1️⃣ Confusing: • resuscitation fluids
• maintenance fluids
• replacement fluids
2️⃣ Ignoring “hidden fluids” (medication diluents, flushes, fluid creep)
3️⃣ Focusing on volume while underestimating sodium burden
4️⃣ Using nonspecific markers as automatic fluid triggers
5️⃣ Assessing fluid responsiveness while ignoring fluid tolerance
One of the strongest concepts in the review:
🧠 “Fluid responsiveness does not equal fluid tolerance.”
A patient may increase stroke volume after a bolus and still deteriorate from: • venous congestion
• pulmonary edema
• renal congestion
• abdominal hypertension
• impaired microcirculation
That distinction is fundamental.
The article strongly supports integrating: 📡 Lung ultrasound
📡 VExUS
📡 venous Doppler
📡 congestion assessment
📡 organ specific fluid tolerance
🚨 Lactate is a clue. Not a fluid order.
Also
• hyperlactatemia
• oliguria
• tachycardia
• low CVP
are often misinterpreted as direct triggers for fluid administration despite poor specificity for hypovolemia.
Especially after:
• ANDROMEDA SHOCK
• early vasopressor strategies
• capillary refill guided resuscitation
• fluid stewardship concepts
One of my favorite lines conceptually from this review:
🧂 “Sodium may matter more than volume.”
That idea deserves much more discussion.
The authors emphasize that: fluid accumulation is frequently driven not only by liters, but by cumulative sodium and chloride exposure.
Including: • maintenance fluids
• replacement fluids
• medication diluents
• “fluid creep”
This is a critical but frequently ignored concept in ICU practice.
The paper also revisits the ROSE model: 🌹 Resuscitation
🌹 Optimization
🌹 Stabilization
🌹 Evacuation
A framework that encourages phase specific fluid therapy instead of continuous indiscriminate fluid loading.
Particularly interesting: the review supports earlier vasopressor initiation in vasoplegic shock.
Not every hypotensive patient is “fluid depleted.”
Sometimes the real pathology is: 🩸 vasoplegia
🩸 endothelial dysfunction
🩸 vascular leak
🩸 loss of vascular tone
In these situations: more fluid may simply worsen interstitial edema while norepinephrine addresses the actual pathophysiology.
My main takeaway:
Future fluid management will probably become: less protocolized, less volume centered, and far more physiology driven.
The intensivist of the future may think less in terms of: “how many liters?”
And more in terms of:
🧠 perfusion
🧠 tolerance
🧠 congestion
🧠 sodium load
🧠 vascular tone
🧠 phase of shock
From flood to finesse.
📖 Reference
Vanden Eede, M. Annals of Intensive Care, 16, 100074. https://t.co/u6Zf8P3DHG
🫀📝Recomendaciones de Expertos para el Manejo del Shock Cardiogénico
🔰📚Annals of Intensive Care 2026
https://t.co/wQMBA8BEy0
Enlace a Artículo Completo👇🏻✅🆓
https://t.co/xumUMHaxVK
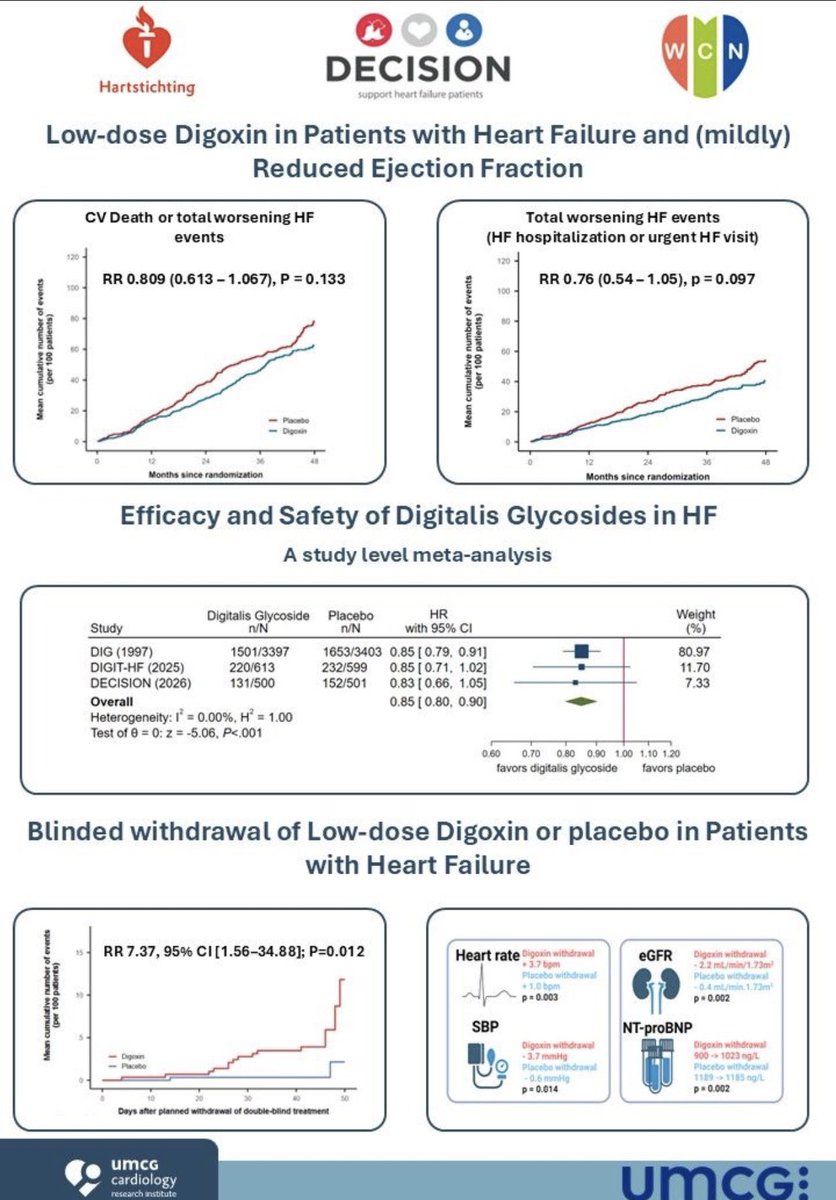
Digoxin: the drug everyone loves to forget… until the data keep coming back.
#HeartFailure26
DECISION trial + updated meta-analysis:
• ↓ worsening HF events
• Consistent signal across studies
• Withdrawal associated with rapid clinical deterioration
Maybe digitalis glycosides deserve a more nuanced conversation in modern HFrEF management.
#HeartFailure #CardioTwitter #ESCCongress #Digoxin
@SJGreene_md@gcfmd@DrMarthaGulati@hvanspall@kevin_damman@BiykemB@MartaCoboMarcos@hfcollaboratory
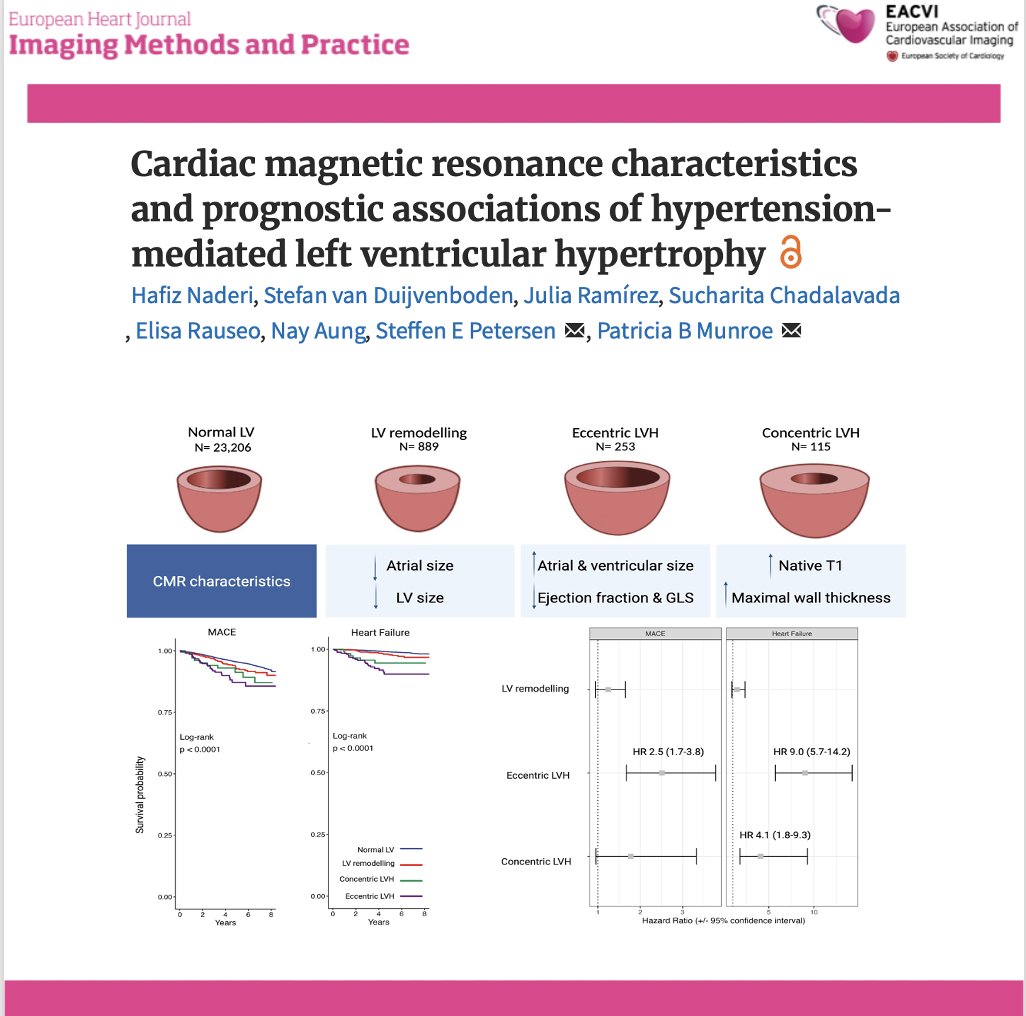
📄 Hypertension-related LVH: not all phenotypes carry the same risk
🔗 DOI: https://t.co/W1SFC0ZCz6
🫀 Hypertension is the most common cause of LV hypertrophy—but its cardiac expression is far from uniform.
This large UK Biobank CMR study (n >24,000) provides a comprehensive look at LVH phenotypes and their prognostic impact.
✨ Four CMR-defined phenotypes:
👉 Normal LV
👉 LV remodelling
👉 Eccentric LVH
👉 Concentric LVH
📊 As shown in the graphical abstract (page 2):
➡️ each phenotype has distinct structural and functional signatures
✨ Key findings:
🔹 Eccentric LVH = worst phenotype
➡️ Most impaired LV function (EF + strain)
➡️ Largest chambers
➡️ Highest risk:
MACE → HR 2.5
Heart failure → HR 9.0
🔹 Concentric LVH:
➡️ Highest wall thickness and native T1 (fibrosis)
➡️ ↑ Heart failure risk (HR 4.1)
➡️ No significant MACE association
🔹 LV remodelling:
➡️ Intermediate phenotype
➡️ Smaller chambers, milder changes
📊 Key pathophysiological insight:
👉 LVH is not a binary condition—but a spectrum of myocardial adaptation
➡️ From remodelling → concentric or eccentric hypertrophy
➡️ Driven by pressure load, volume load, and myocardial response
💡 Clinical take-home message:
👉 Not all LVH is equal
✔ Eccentric LVH → high-risk phenotype
✔ Concentric LVH → fibrotic, HF-prone phenotype
👉 CMR enables:
precise phenotyping
improved risk stratification
potential tailored treatment strategies
🚨 Bottom line:
In hypertension, LV geometry matters—because different phenotypes carry very different prognoses.
#Cardiology #CMR #Hypertension #LVH #CardiacImaging #HeartFailure #RiskStratification #PrecisionMedicine #UKBiobank 🫀📊
🫀 ARDS is not just a lung disease.
It’s a right ventricle disease.
⚠️ And we keep ventilating like it isn’t.
🧠 The blind spot
We focus on:
✔️ Tidal volume
✔️ Plateau pressure
✔️ Oxygenation
But we ignore:
👉 Right ventricular (RV) afterload
🔥 What really kills in ARDS
Not only hypoxemia.
👉 RV failure → hemodynamic collapse → death
💥 Why?
ARDS creates a perfect storm:
▪️ Hypoxemia → pulmonary vasoconstriction
▪️ Hypercapnia → ↑ PVR
▪️ Microthrombosis → vascular obstruction
▪️ “Baby lung” → ↓ compliance
👉 Result:
🫀 Massive increase in RV afterload
⚠️ And then we make it worse.
💉 Your ventilator can injure the RV
Even “protective” settings:
👉 6 ml/kg PBW
can STILL:
❌ Overdistend alveoli
❌ Compress pulmonary vessels
❌ Increase RV afterload
🔥 The paradox
Lung-protective ≠ RV-protective
Examples:
🔺 High PEEP → better oxygenation
BUT
→ ↑ RV afterload
🔻 Low driving pressure → lung protection
BUT
→ hypercapnia → ↑ pulmonary vasoconstriction
⚠️ You fix the lung… and crash the RV.
🧬 Key concept
👉 RV afterload is dynamic
👉 It increases during inspiration
👉 It depends on HOW you ventilate
💡 What should change
Stop ventilating only for:
❌ PaO₂
❌ PaCO₂
Start ventilating for:
✔️ RV afterload
✔️ Pulmonary vascular resistance
✔️ Cardiopulmonary coupling
🛠️ Practical shift
Think:
▪️ Driving pressure (target ↓)
▪️ Recruitability-guided PEEP
▪️ Avoid overdistension AND collapse
▪️ Control hypercapnia (don’t blindly accept it)
🫁 + 🫀 = ONE system
🔥 Game changer
👉 Personalized ventilation
based on:
▪️ Lung mechanics
▪️ RV function
▪️ Hemodynamics
🧠 Tools:
✔️ Echo
✔️ EIT
✔️ Esophageal pressure
✔️ Pulmonary pressures
🚨 Final message
If you are not monitoring the RV…
👉 You are ventilating half the patient.
🫀 Protect the lung
🫀 Protect the RV
👉 Or you protect neither.
📚 Slobod D. et al.
Intensive Care Medicine, 2026
https://t.co/cnvTDCQtcF
💧 Albumin in the ICU: life-saving drug… or expensive myth?
We’ve been using it since the 1940s.
Yet in 2026 we still don’t fully agree when it actually helps.
🧠 First principle
Albumin is NOT just a volume expander.
It does much more:
▪️ Maintains oncotic pressure
▪️ Protects endothelium & glycocalyx
▪️ Modulates inflammation
▪️ Alters drug pharmacokinetics
➡️ It’s a biologically active molecule, not “fancy saline”
⚠️ The uncomfortable truth
👉 50-70% of albumin use is inappropriate
👉 In some studies: >90% misuse
Yes… even in modern ICUs
🔥 Where albumin actually WORKS
✔️ Hepatorenal syndrome (HRS)
→ Albumin + terlipressin = better renal outcomes
✔️ Spontaneous bacterial peritonitis (SBP)
→ ↓ AKI + ↓ mortality
✔️ Large-volume paracentesis
→ Prevents circulatory collapse
⚖️ Where evidence is… mixed
🟡 Septic shock
→ No mortality benefit vs crystalloids
→ BUT better hemodynamics in some patients
🟡 ARDS
→ Improves oxygenation (if hypoalbuminemic)
→ No survival benefit
🟡 Major surgery
→ ↓ fluids, ↓ complications
→ BUT watch renal risk (especially 20%)
🚫 Where you should think twice
❌ Traumatic brain injury
→ ↑ ICP
→ ↑ mortality
➡️ Albumin crosses disrupted BBB → worsens edema
💡 Key ICU insight
Albumin is NOT about:
❌ “giving protein”
❌ “correcting labs”
It’s about:
✔️ hemodynamics
✔️ endothelial integrity
✔️ patient selection
📉 Hypoalbuminemia matters
Every ↓10 g/L:
▪️ ↑ mortality
▪️ ↑ complications
▪️ ↑ length of stay
➡️ But correction ≠ automatic benefit
🎯 Clinical decision rule
Use albumin when:
✔️ Cirrhosis-related complications
✔️ Refractory shock after crystalloids
✔️ Severe hypoalbuminemia with instability
Avoid when:
❌ Routine resuscitation
❌ TBI
❌ “just low albumin”
🧠 Take-home
➡️ The question is NOT
“Does albumin work?”
➡️ The real question is
“In which patient, at which moment?”
📚 Rubio-Baines I et al. (2026)
Journal of Clinical Medicine
DOI: 10.3390/jcm15051981