Subsecretario @EduardoClark sostengo que están comprando medicamentos a sobreprecio, a proveedores de dudosa procedencia, menos claves y con afectaciones para los pacientes👇
Revisen sus datos: el precio promedio por pieza de medicamento en 2018 fue de $38.72 pesos, y con la presidenta Sheinbaum, en 2026, de $91.83 pesos.
Ustedes dicen que se debe a que están comprando más medicamentos de especialidad, pero eso también está en duda.
El 30 de marzo de 2026 se anunció una reducción del catálogo de medicamentos del sector público de 2,753 a 1,929 claves. La justificación oficial habla de priorizar los tratamientos más eficaces, seguros y disponibles, y de optimizar el uso de los medicamentos. En la práctica, eliminaron más de 800 claves de medicamentos sin que su decisión pudiera ser evaluada por especialistas externos y sin consultar a los pacientes, una restricción sin precedentes de las opciones terapéuticas disponibles para los médicos y pacientes del sector público.
A esto se suma que también compran medicamentos falsificados que ponen en riesgo la vida de los pacientes. Está el caso de las 11 mil piezas de Keytruda, la mayoría adquiridas por el ISSSTE y el IMSS-Bienestar. Todo por seleccionar proveedores apócrifos, sin antecedentes, sin verificar registros sanitarios y a precios de “ganga”, según el gobierno.
Hoy el sector privado concentra 72.8% de las piezas de medicamentos distribuidas a los mexicanos. Esto confirma que, ante las fallas del sistema público, el acceso a medicamentos descansa cada vez más en el bolsillo de las familias y en el mercado privado.
Le comparto las ligas de estas investigaciones que el gobierno se ha empeñado en desacreditar, pero no en atender:
https://t.co/qC8WleDGj2
https://t.co/RGCT8syMrv
https://t.co/PDIoi4tTxi
https://t.co/p4K9mO9s8M
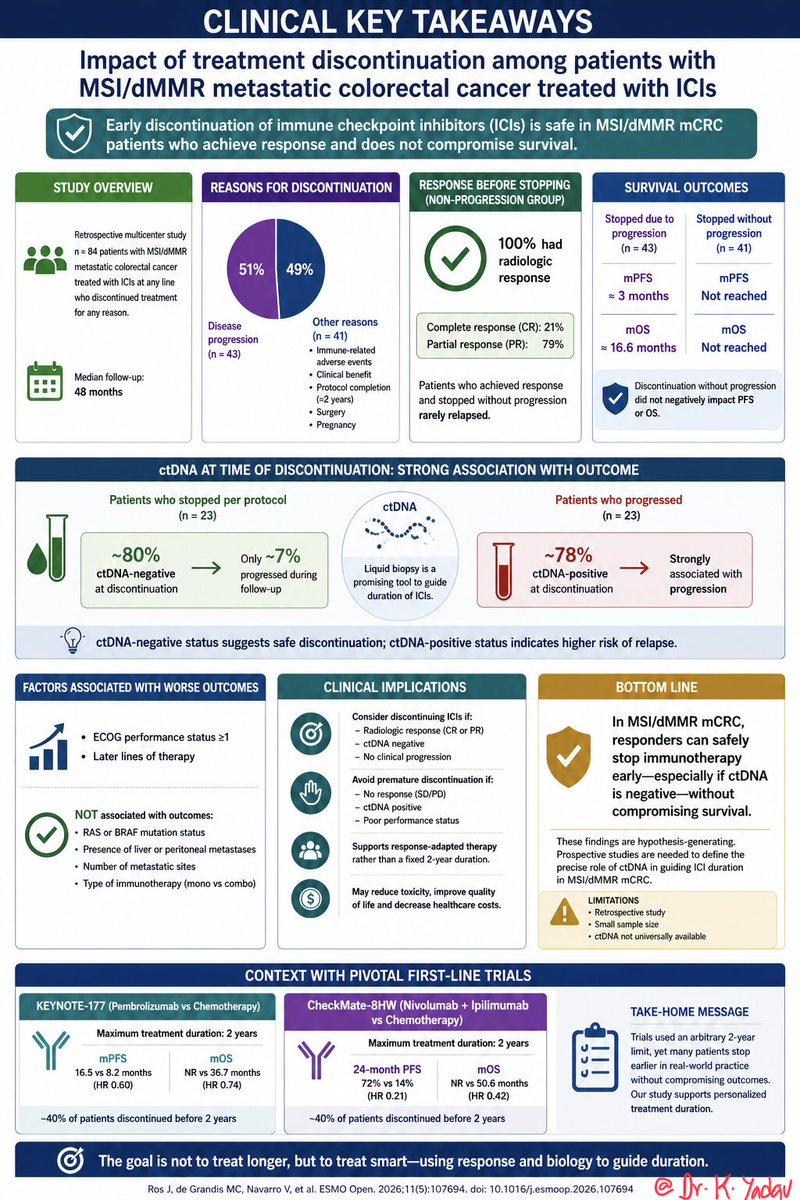
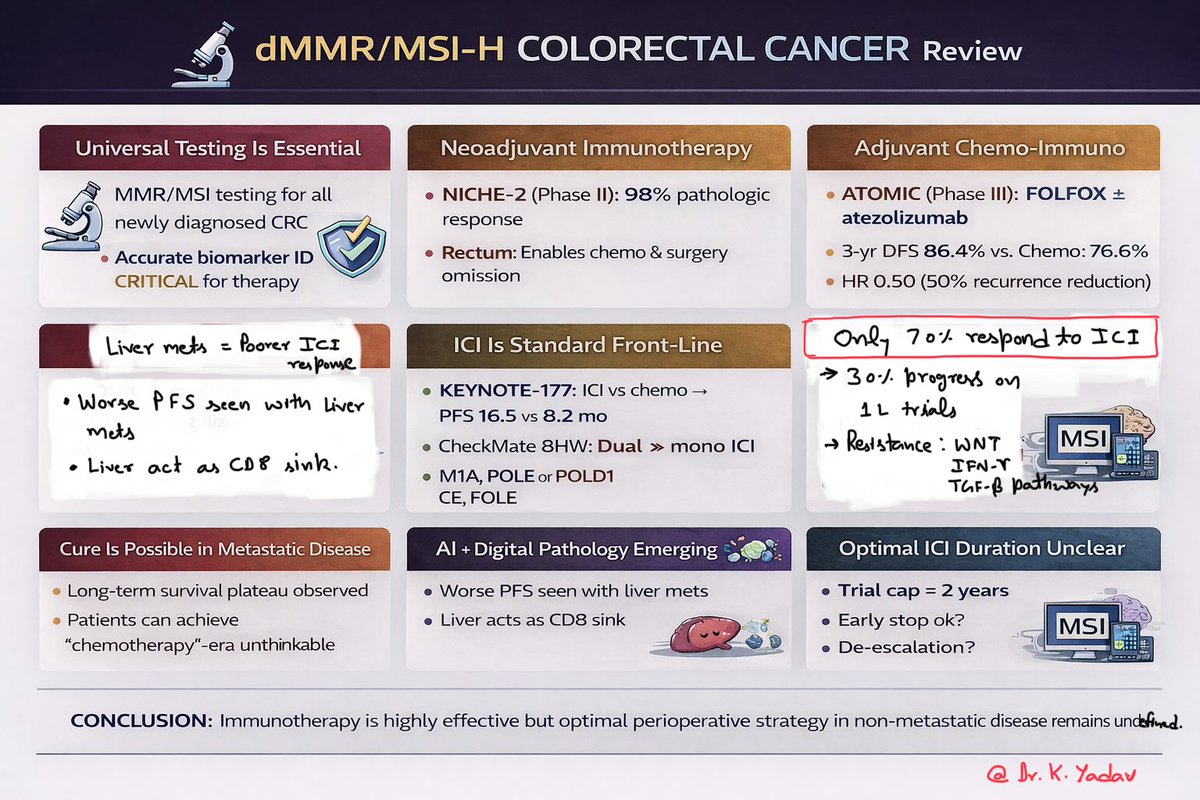
Can we safely STOP immunotherapy early in MSI mCRC? 🤔
New real-world data says YES — if patients respond.
✔ No OS/PFS compromise
✔ ctDNA-negative → very low relapse risk (~7%)
✔ Fixed 2-year duration? Probably arbitrary
👉 Time for response-adapted ICI duration?
#Oncology #CRC #Immunotherapy #MedTwitter @ESMO_Open #precisiononcology @OncoDailyGI@OncoDailyIO
https://t.co/roXv3yn1iW
A comprehensive, step-by-step video guide on Pancreatoduodenectomy. We cover:
✅ Dissection planes
✅ Vascular preservation
✅ Reconstruction technique
Perfect for trainees looking to master the steps.
🦓PanNETs @BJS_Surgery Commission: MEN1
👀NF ≤2 cm without growth → observe
🔪Functional → resect, but parenchyma-sparing
🚫NO total pancreatectomy
🔄Expected recurrence 21-63% — nature of the disease, not surgical failure
🔗https://t.co/fqS90z6MkO
@spartelli
#Obesity is associated with higher risk for 12 #cancer types and accounts for approximately 10% of annual new cancer cases in the US.
📄 This Review summarizes the primary biological pathways connecting obesity and cancer development.
https://t.co/1ggRbdtW56
About 25 years in pancreatic cancer, what we’ve really done is the same: rearranging treatment sequence and intensity.
For the first time, that cycle may be breaking👇
Daraxonrasib (pan-RAS inh)
was reported to nearly double OS compared with chemotherapy.
https://t.co/GaDveHpf2v
TNBC is no longer a chemo disease.
This 1 algorithm shows the shift:
👉 ADCs + biomarkers are now driving frontline decisions.
🧬 Metastatic TNBC - how to think today
PD-L1 ≥10
• Pembro + chemo
• OR Pembro + SG
PD-L1 <10
• SG or Dato-DXd now competing with chemo
BRCA-mut
• PARP inhibitors
HER2-low
• T-DXd option
Later lines
• ADC sequencing
• Biomarker-directed therapy
🧠 Paradigm shift
❌ Before: one-size chemo
✅ Now: IO + ADCs + PARPi + precision oncology
⚠️ What matters next
Not just “which drug”
👉 but “what sequence”
Topo-1 ADCs → real cross-resistance concern
🎯 Takeaway
Advanced TNBC has entered the ADC era.
Smart sequencing will define outcomes. 🔖
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #TNBC #BreastCancer @OncoAlert@myesmo@esmo_open@JCOPO_ASCO
🚨 New ASCO Guidelines (2026): Anaplastic Thyroid Cancer (ATC)
One of the most aggressive cancers.
Now finally algorithm-driven.
🧠 Step 1 = GENOMICS (don’t skip this)
👉 Test for: BRAF | RET | NTRK
🔥 If BRAF V600E → THIS CHANGES EVERYTHING
👉 Dabrafenib + Trametinib = STANDARD
📊 ROAR trial
• ORR ~69%
• Durable responses in a historically lethal disease
👉 Consider adding Pembrolizumab (selected cases)
🧠 If NO actionable mutation
👉 Options:
• Lenvatinib ± Pembrolizumab
• Ipilimumab + Nivolumab
📊 Evidence: small phase II / non-randomized studies
⚠️ Modest activity vs BRAF-targeted therapy
🧠 RET / NTRK fusion (rare but important)
👉 Treat like precision oncology
• RET → Selpercatinib (LIBRETTO-001)
• NTRK → Larotrectinib / Entrectinib (TRK pooled / STARTRK)
🧠 After progression
👉 Clinical trial = BEST option
If not available:
• Lenvatinib ± Pembrolizumab
• Chemotherapy (last-line)
🔖 Save this - ATC decisions are time-critical
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #ThyroidCancer #ATC #PrecisionOncology @OncoAlert@myesmo@esmo_open@asco
📌 Lymph Node Management of Patients With Breast Cancer in the Era of Therapy De-escalation
🔗 https://t.co/UpfZoB0ZH5
@OncoAlert#OncoAlertAF#BreastCancer
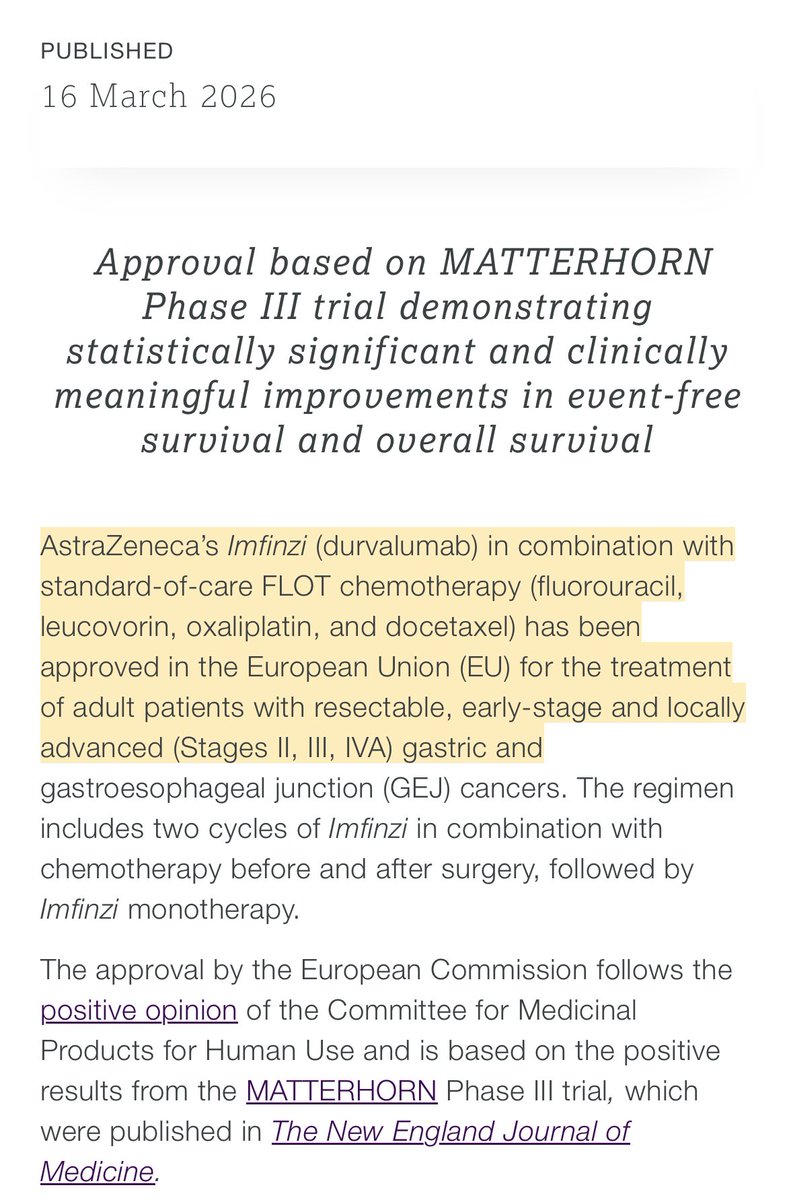
🧬 Durvalumab (Imfinzi) approved in EU
📍 1st perioperative IO for resectable GC/GEJ (stage II–IVA)
💊 + FLOT ± surgery → durva maintenance
📊 Based on Ph III MATTERHORN (↑ EFS & OS)
🔎 New SoC in early GC/GEJ
🔗 https://t.co/PO5hmOPurW
@OncoAlert@Larvol@GrupoTTD
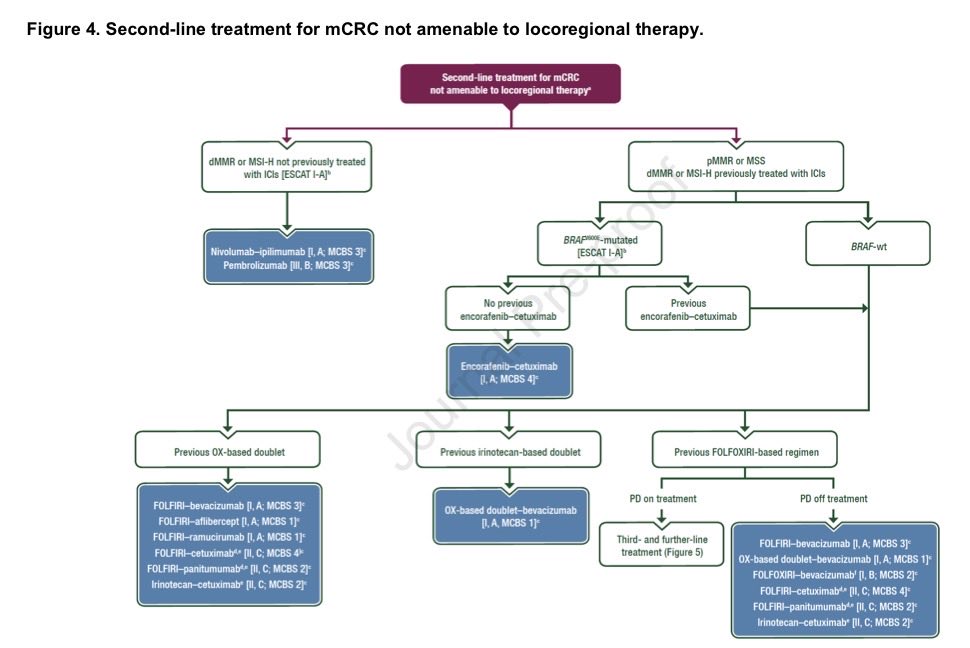
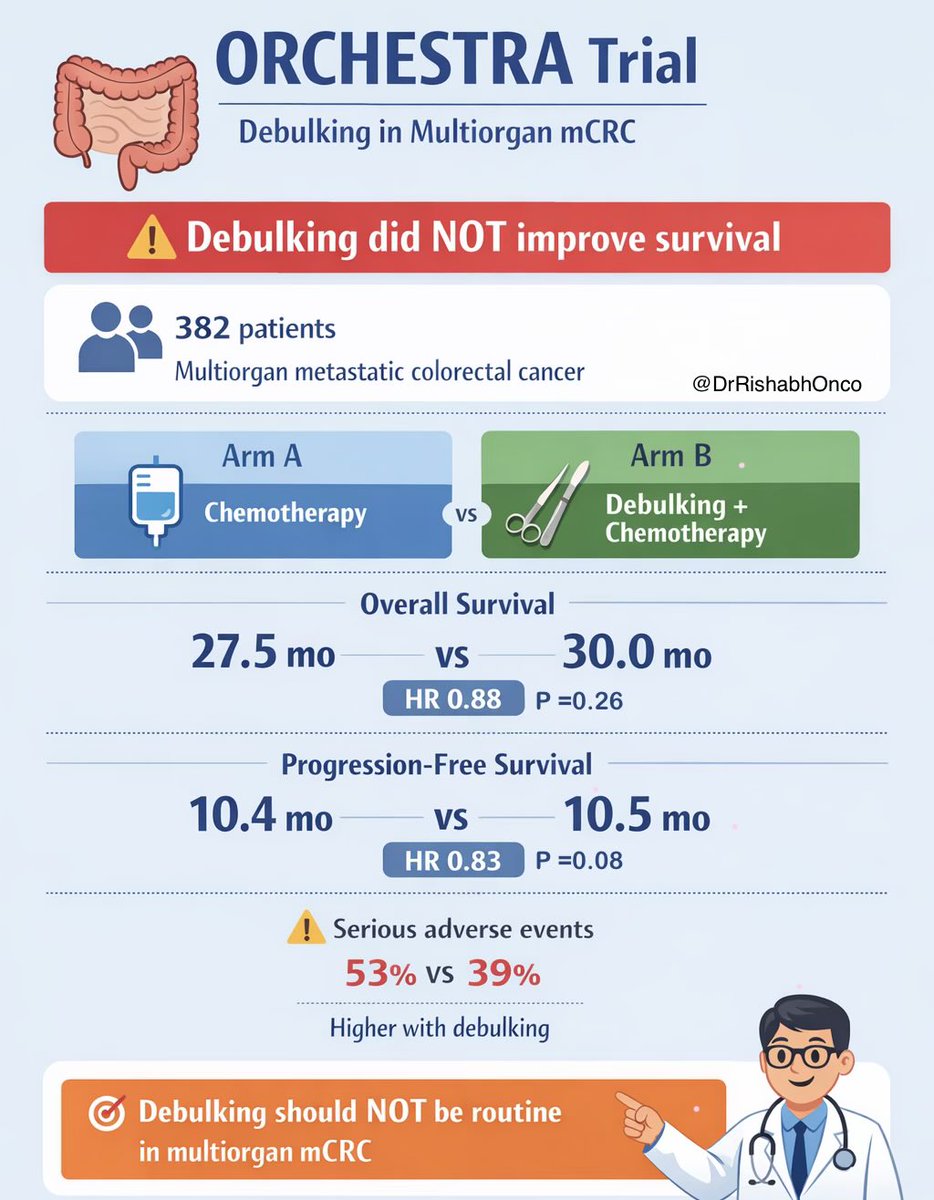
🧬 More treatment is not always better in metastatic colorectal cancer.
The phase 3 ORCHESTRA trial tested whether adding aggressive tumor debulking to systemic therapy improves outcomes in multiorgan mCRC.
The answer: No survival benefit.
🧪 Trial design
Patients with multiorgan metastatic colorectal cancer whose disease was controlled after induction chemotherapy were randomized to:
🔹 Chemotherapy alone
🔹 Tumor debulking + chemotherapy
📊 Key results
Overall survival
• 27.5 vs 30.0 months
• HR 0.88 (NS)
Progression-free survival
• 10.4 vs 10.5 months
• HR 0.83 (NS)
⚠️ Toxicity
Serious adverse events were higher with debulking
53% vs 39%
🎯 Clinical takeaway
In multiorgan mCRC, adding aggressive tumor debulking to palliative chemotherapy does not improve survival and increases complications.
An important negative trial for MDT decision making.
🔖 Save for GI oncology discussions.
📖 Full paper in comment ⬇️
@OncoAlert@myesmo@esmo_open@asco
#OncoTwitter #MedTwitter #ColorectalCancer #GIonc
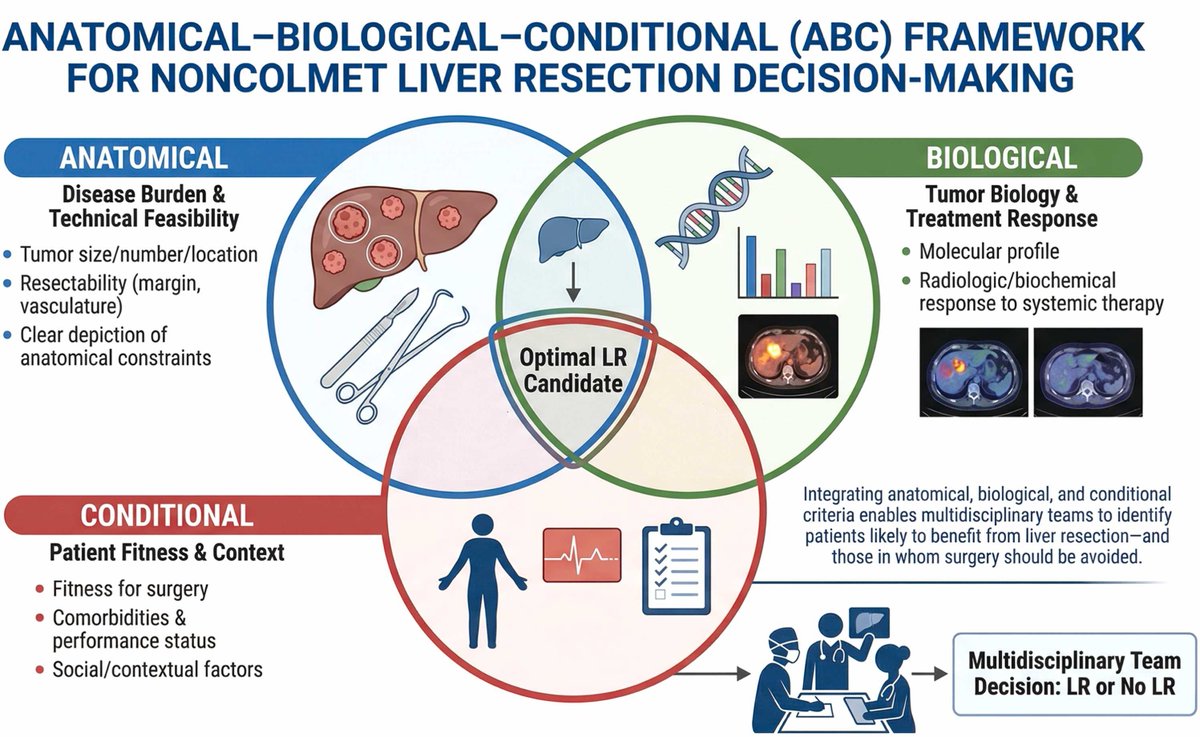
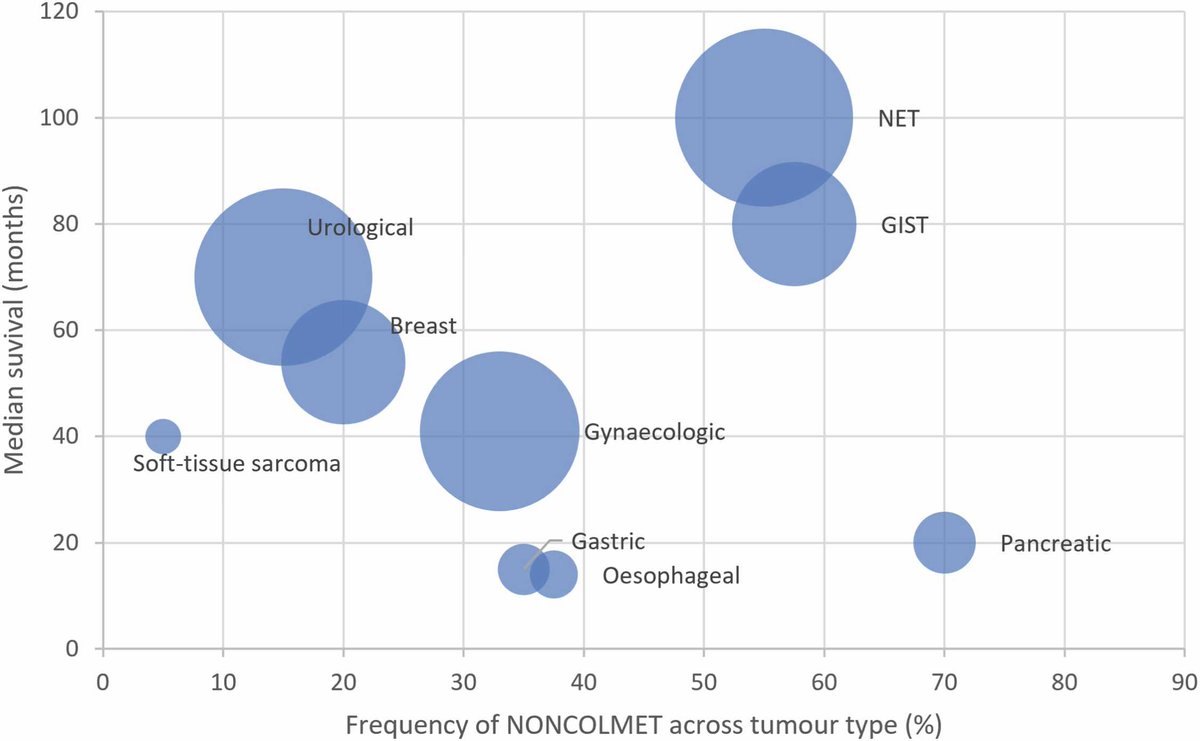
Liver resection for non colorectal mets 🫧 biology biology biology!
🧬 Survival depends on indication 🦓 NET and GIST after TKI best
✋ Pancreas and UpperGI ONLY in extremely selected oligo and liver-only
https://t.co/FksGq9T7p9