Endocrine and Thoracic Surgical Pathology. Author of Endocrine Pathology and Patología de la glándula Tiroides. Editor in Chief of Archivos de Patología.
A study in Head and Neck Pathology analyzes 23 cases of oral carcinoma cuniculatum (CC) and classifies them into three groups: CC, conventional OSCC, and uncertain CC. This classification aids in understanding their distinct characteristics.
https://t.co/ZD5Hsue0EI
"Nuclear Palisading" at the edges of oncocytic epithelial fragments helps distinguish Warthin tumor from oncocytoma on salivary gland FNA (in addition to other features seen here - flat monolayering, lymphs and cystic debris).
@rqbittenc Dear Dr. Bittencourt,
I am Dr. Severino Rey, a Spanish pathologist and President PathoExpert. Please contact me at [email protected] to discuss an educational project I am leading and your potential participation. Kind regards.
Invasive fungal rhinosinusitis 🧫
Focus: what the pathologist must not miss in the report
Brief but potentially lethal: invasive fungal rhinosinusitis (IFR) is the form in which the fungus leaves the mucosa and invades submucosa, vessels, and bone, especially in neutropenic patients, decompensated diabetics, and transplant recipients.
Definition 🧬
IFR is histologically defined by invasion of the mucosa/submucosa by hyphae, with or without angioinvasion, clearly distinguishing it from non‑invasive forms (fungal ball, allergic fungal rhinosinusitis).
Histopathology 🔬
Architecture: nasal/sinonasal mucosa with necrosis and acute or mixed inflammation, often with “empty” areas of necrotic tissue permeated by hyphae.
Hyphae
📌Mucorales: broad, pauciseptate hyphae with irregular, often right‑angle branching (frequently collapsed on H&E).
📌Aspergillus: thin, septate hyphae with dichotomous, acute‑angle branching.
Vessels: thrombosis, necrosis of the vessel wall, and intraluminal invasion are the hallmark of the acute form; this explains the “black turbinate sign” on MRI.
Immunohistochemistry and special stains
H&E + Grocott–Gomori: highlights hyphae and their extent in vessel walls/bone.
PAS: useful, but less sensitive in extensive necrotic fragments.
IHC is occasional (for example, MUC5B, maspin in studies), not routine; the gold standard remains H&E + silver stain.
Diagnostic pitfalls ⚠️
Superficial biopsy with only crust/necrosis and no submucosa: high risk of calling “fungal colonization,” underestimating true IFR.
Necrosis without demonstrable hyphae: cut deeper levels, request Grocott, and if still doubtful, suggest a new biopsy in correlation with clinical/imaging data.
Confusing chronic invasive forms (Aspergillus, mucormycosis in diabetics) with tumor: solid masses with bone invasion can mimic malignant neoplasms.
What must be in the pathologist’s report 🧾
Explicitly state whether there is invasion of mucosa/submucosa and vessels by hyphae.
Suggest the likely genus (Mucorales‑type vs Aspergillus‑type pattern), with a recommendation to correlate with culture/PCR.
Indicate that the finding is compatible with invasive fungal rhinosinusitis and justify the urgency of clinico‑radiologic correlation and combined surgical + antifungal management.
Take-Home Messages NotasDePatologia
📌IFR is, above all, a histologic diagnosis of invasion, not merely of the presence of fungus.
📌Hyphae in vessel walls/lumina explain necrosis and worse prognosis; describe this clearly in the report.
📌Superficial, crust‑only biopsies are the main trap; ask for new material when necessary.
Selected References
Roland LT et al. Int Forum Allergy Rhinol, 2023 – AIFS consensus on pathology, imaging, and management.
Pagella F et al. J Cranio-Maxillofac Surg, 2016 – Acute vs chronic IFRS, clinicopathologic correlation.
Kurokawa M et al. RadioGraphics, 2022 – IFRS routes of orbital/cavernous invasion and imaging–pathology correlation.
⚠️Disclaimer⚠️
This text is an educational summary for healthcare professionals and students; it does not replace full pathology reports, local guidelines, or individualized clinical decision‑making.
#Pathology #HeadNeckPathology #InfectiousDisease #FungalSinusitis #InvasiveFungalRhinosinusitis
#SurgicalPathology #Histopathology #ENT #MedEd #MedicalEducation #NotasDePatologia
Especial médicos🩺⚕️🏥👨🏻⚕️👩🏻⚕️.
Os dejo esta carta en JAMA. Se la pondré a mis alumnos en la próxima clase:
He elegido estas frases :
👇🏻⏰
«La medicina puede tener un significado extraordinario. Pero no puede sustituir el estar presente en tu propia vida. El mundo puede necesitarnos como médicos. Pero las personas que nos aman nos necesitan como nosotros mismos. Y ese es el rol que nadie más puede llenar.»
«La residencia refuerza la lección de que las instituciones están diseñadas para perdurar más allá de los individuos. En cambio, las familias no.»
«Creo en formar a la próxima generación. Creo en el significado de este trabajo. Lo que ha cambiado es mi disposición a absorber el desgaste sin cuestionarlo.»
«Ya no estoy dispuesta a seguir posponiendo la vida. La medicina exige mucho. Y nosotros damos profundamente. Pero no puede tomarlo todo.»
«El significado de mi trabajo es profundo. El significado de mi presencia en casa es irremplazable.»
@TuiteroSismico Que función cumple la ONU que no paraliza los crímenes de lesa humanidad?
No funciona nada en el mundo mas que la violencia y el peso del más fuerte.
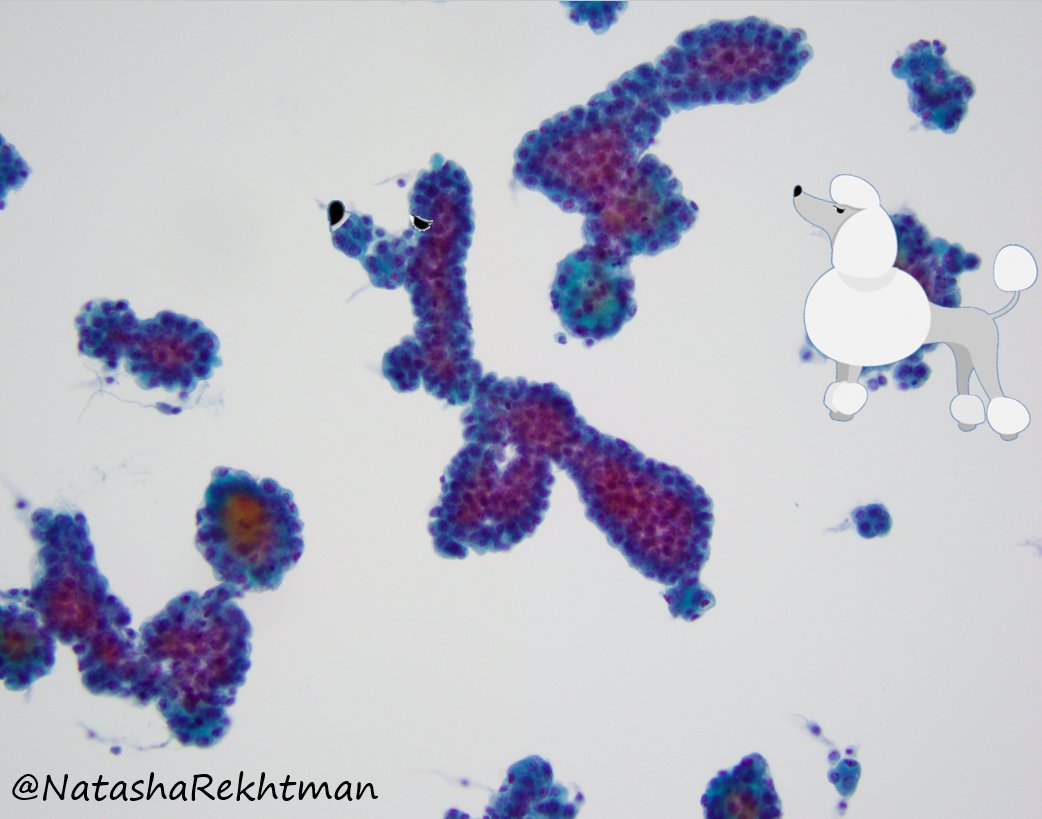
Hi #pathology friends!
Pleural effusion. Do you see what I see? 🐩
When mesothelial cells form complex arborizing groups like this - it is a good clue to mesothelioma.
So .. new diagnostic term: the “poodle sign”?
#PathArt
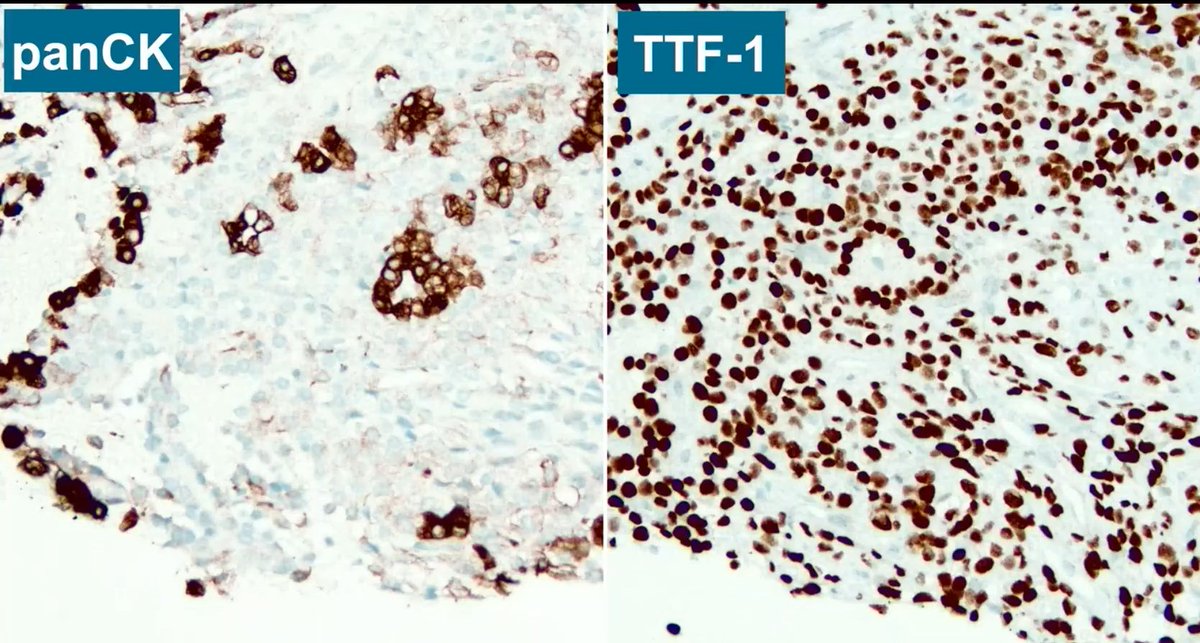
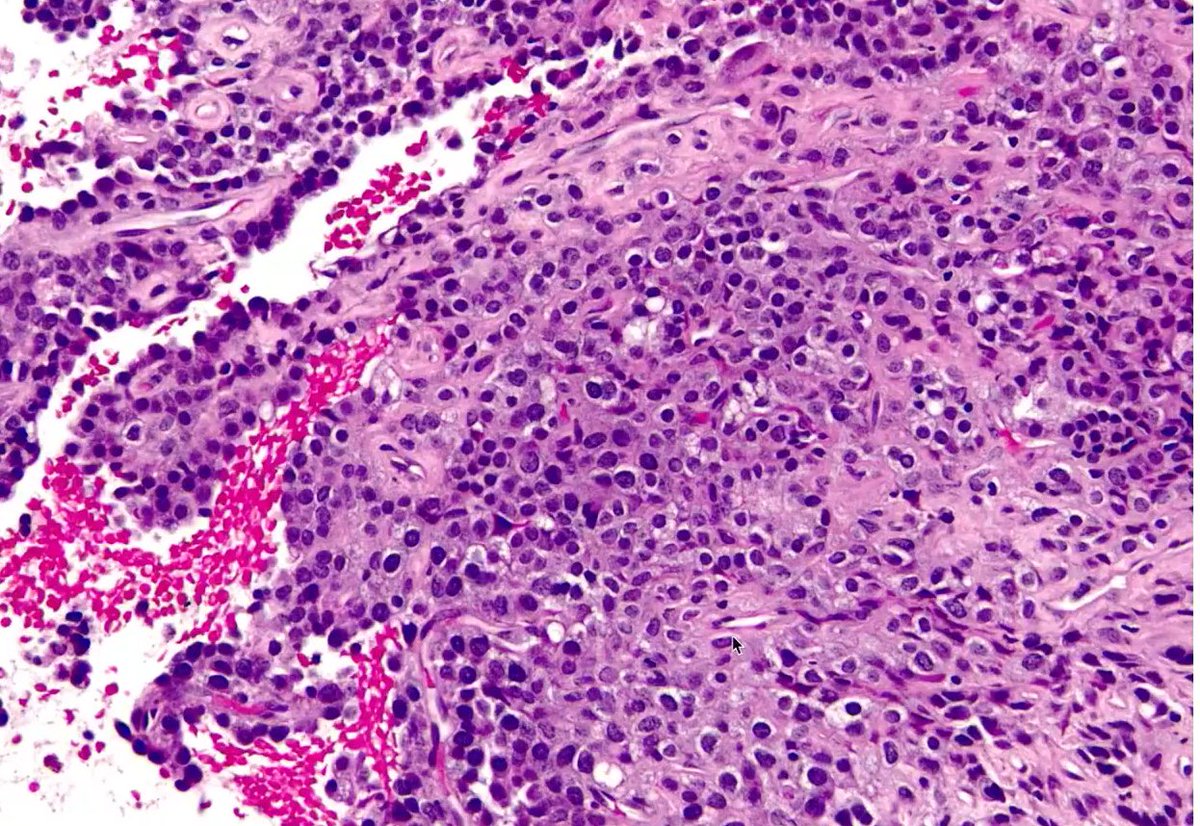
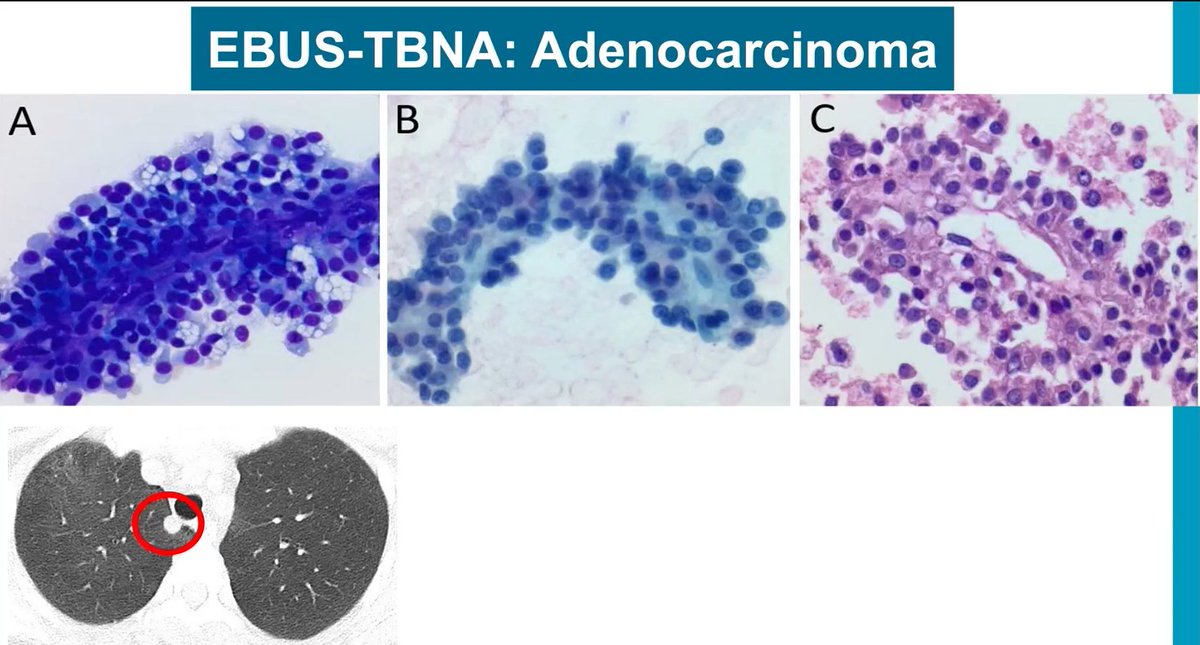
Common pitfall in lung cytopathology
Cytology mimicking adenocarcinoma (pic 1)
If you get a core biopsy and see a dissociation between CK AE1/AE3 and TTF-1 staining, stop!
Lung cells are not CK AE1/AE3 negative and TTF-1 positive; only stromal cells in sclerosing pneumocytoma are (pic 3).
Clues for sclerosing pneumocytoma in cytology (very hard diagnosis to make):
- Foamy macrophages, cuboidal cells, IHC (CK-, TTF-1+)
- Clinical clues: young to middle-aged women
Dr. Mukhopadhyay - Pathology on The Coast 2025, CAP On Demand #pathology #pathX #pathtwitter #CAP