Obesity Medicine Physician, Medical Director, UNC Physicians Network Weight Management Program, Advocate for better obesity care for ALL. #GDTBATH My views
The enormous amount of UPF consumed by children/teens is causing serious harm in the STROKE BELT. "Pharmacotherapy alone" approach is NOT the answer! Here is our latest paper on a strategy to reduce UPF/SSB consumption: https://t.co/PnMfsNKdr9
This OMA podcast explores how our food environment is affecting the health of our children. Dr. V. Sushma Chamarthi, MD, FAAP, DABOM & I unpack our latest article, "The Impact of Ultra-Processed Foods on Pediatric Health" hosted by Dr. Suzanne Cuda.https://t.co/vwPDUgvC2A
In a much needed collaboration, @AmDiabetesAssn , @ObesityAction , and @ObesitySociety yesterday convened a symposium and workshop to focus on better systems for obesity care. Great way to start @ObesityWeek!
https://t.co/wLn6kKXIr3
The enormous amount of UPF consumed by children/teens is causing serious harm in the STROKE BELT. "Pharmacotherapy alone" approach is NOT the answer! Here is our latest paper on a strategy to reduce UPF/SSB consumption: https://t.co/PnMfsNKdr9
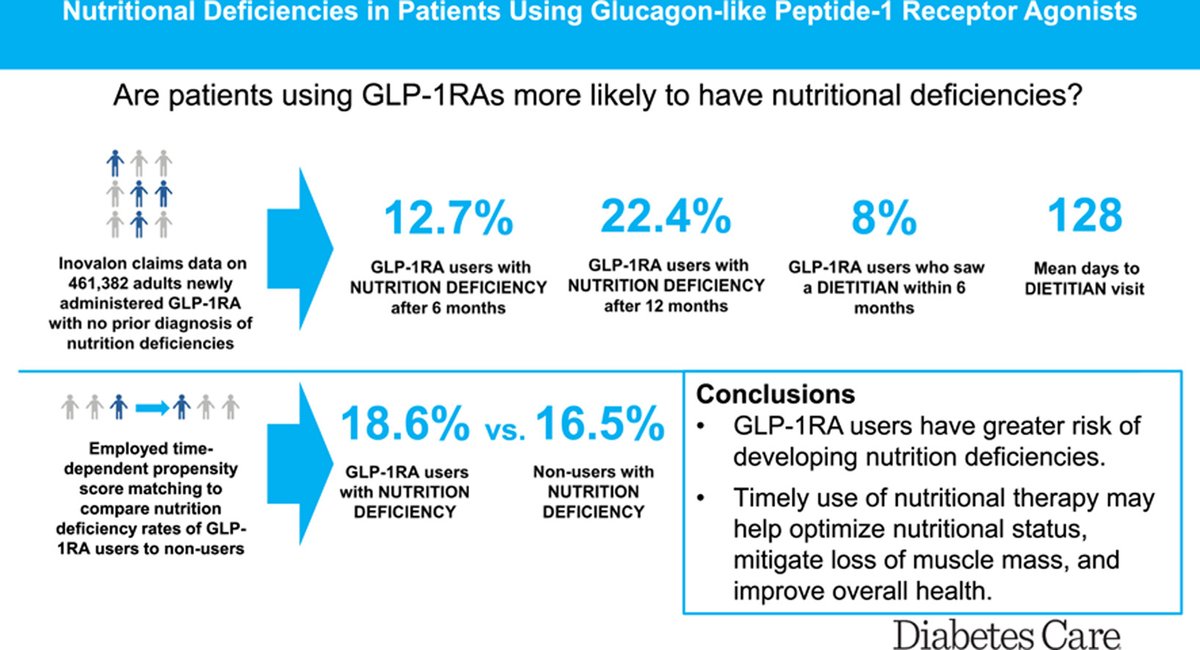
💉 GLP-1 meds don’t just curb appetite—sometimes they curb essential nutrients too.
- - -
📉 In a study of 460,000+ adults on GLP-1s (mostly with T2D):
🔹13% developed nutritional deficiencies in 6 months
🔹22% within 12 months
🔹Vitamin D deficiency was most common (13.6%)
🔹3% experienced muscle loss
🔍 Patients who saw a dietitian were more likely to have deficiencies identified—not because dietitians caused harm, but because they actually looked.
💡 Clinical translation:
🔹Appetite suppression can lower intake of protein, vitamins (D, B12, folate), and minerals.
🔹Without supervision, this can compromise muscle mass, hydration, and metabolic health.
🔹Older adults and those with obesity are especially vulnerable due to baseline deficiencies.
Treating obesity isn't just about weight loss—it's about preserving health while losing weight.
✅ That’s why supervised care with physicians + registered dietitians is non-negotiable.
✅ Monitor labs (Vit D, B12, iron, folate).
✅ Emphasize protein, strength training, and hydration.
📚https://t.co/zFOUF6CKcv
Credit to @drbutsch and colleagues.
“It’s not enough to think that ‘I have to go swimming several times a week,’” Forman said. “We are talking now about adding in strength training at least twice a week. And it is just as essential if not more so to prevent decline.”
Adults who aced the so-called sitting-rising test were far less likely to die of natural or cardiovascular causes over about 12 years of follow-up than those who scored the lowest, according to a study published online on June 18 in the European Journal of Preventive Cardiology.
The study added to the body of evidence showing that various measures of physical function beyond aerobic fitness, including flexibility, the ability to stand on one leg, and grip strength, can predict longevity. https://t.co/RGYaAFeM1S
Adults who aced the so-called sitting-rising test were far less likely to die of natural or cardiovascular causes over about 12 years of follow-up than those who scored the lowest, according to a study published online on June 18 in the European Journal of Preventive Cardiology.
The study added to the body of evidence showing that various measures of physical function beyond aerobic fitness, including flexibility, the ability to stand on one leg, and grip strength, can predict longevity. https://t.co/RGYaAFeM1S
2/ Also grateful to the course directors for the opportunity to return and share my favorite topic: "Ensuring Equal Access to Obesity Care for ALL: A North Carolina Story."
What a privilege to join the panel at the 38th Harvard Blackburn Obesity Course alongside Dr. Jamy Ard, Mr. Joe Nadglowski (CEO of Obesity Action Coalition), and Dr. Amandeep Singh. Our conversation focused on obesity-related health disparities and the ongoing impact of stigma.
@MichaelAlbertMD There is actually a term for this: "buried penis". I get referrals for weight loss from urologists so they can address cancer, infections etc. Any weight loss (not just from ozempic) will expose more.
@l_oshman@NeilFlochMD@MichaelAlbertMD Agree! Primary care perspectives &BARRIERS are often missing. It is EASY to just say Lifestyle modification. But what practical tips & obesity best practices can we share with our primary care colleagues?? Need to include folks who practice obesity medicine in primary care spaces
END/🧾 Summary:
Bariatric Surgery: Myths vs. Data
🔹Perioperative mortality: <0.25% globally
🔹Michigan data: 0.02%
🔹Safer than gallbladder removal, hip surgery, CABG
🔹Long-term mortality ↓ by up to 89%
🔹Complications continue to decline with modern surgical standards
🧠 Knowledge saves lives. So does metabolic surgery.
“We experienced what amounts to censorship and controlling of the reporting of our science,” Dr. Hall said. I appreciate @KevinH_PhD sharing his difficult story for my article, and his longstanding commitment to communicating science to the public. https://t.co/YZVWOl626I
@RapidCarnivore@KevinH_PhD@calleymeans Lifelong behavior change is NOT that simple. Personalized titrations using SMART goals have been quite effective with longitudinal care. Success begets success in this historically underserved populations. These kids are now healthy college students returning on their breaks.
After 21 years at my dream job, I’m very sad to announce my early retirement from the National Institutes of Health. My life’s work has been to scientifically study how our food environment affects what we eat, and how what we eat affects our physiology. Lately, I’ve focused on unravelling the reasons why diets high in ultra-processed food are linked to epidemic proportions of chronic diseases such as diabetes and obesity. Our research leads the world on this topic.
Given recent bipartisan goals to prevent diet-related chronic diseases, and new agency leadership professing to prioritize scientific investigation of ultra-processed foods, I had hoped to expand our research program with ambitious plans to more rapidly and efficiently determine how our food is likely making Americans chronically sick.
Unfortunately, recent events have made me question whether NIH continues to be a place where I can freely conduct unbiased science. Specifically, I experienced censorship in the reporting of our research because of agency concerns that it did not appear to fully support preconceived narratives of my agency’s leadership about ultra-processed food addiction.
I was hoping this was an aberration. So, weeks ago I wrote to my agency’s leadership expressing my concerns and requested time to discuss these issues, but I never received a response. Without any reassurance there wouldn’t be continued censorship or meddling in our research, I felt compelled to accept early retirement to preserve health insurance for my family. (Resigning later in protest of any future meddling or censorship would result in losing that benefit.) Due to very tight deadlines to make this decision, I don’t yet have plans for my future career.
The NIH has been a wonderful place because it allows scientists to take risks, form unique collaborations, and do studies difficult to conduct elsewhere. I’m proud of what we’ve accomplished and I’m fortunate to have had such wonderful colleagues and scientific collaborators. I hope to someday return to government service and lead a research program that will continue to provide gold-standard science to make Americans healthy.