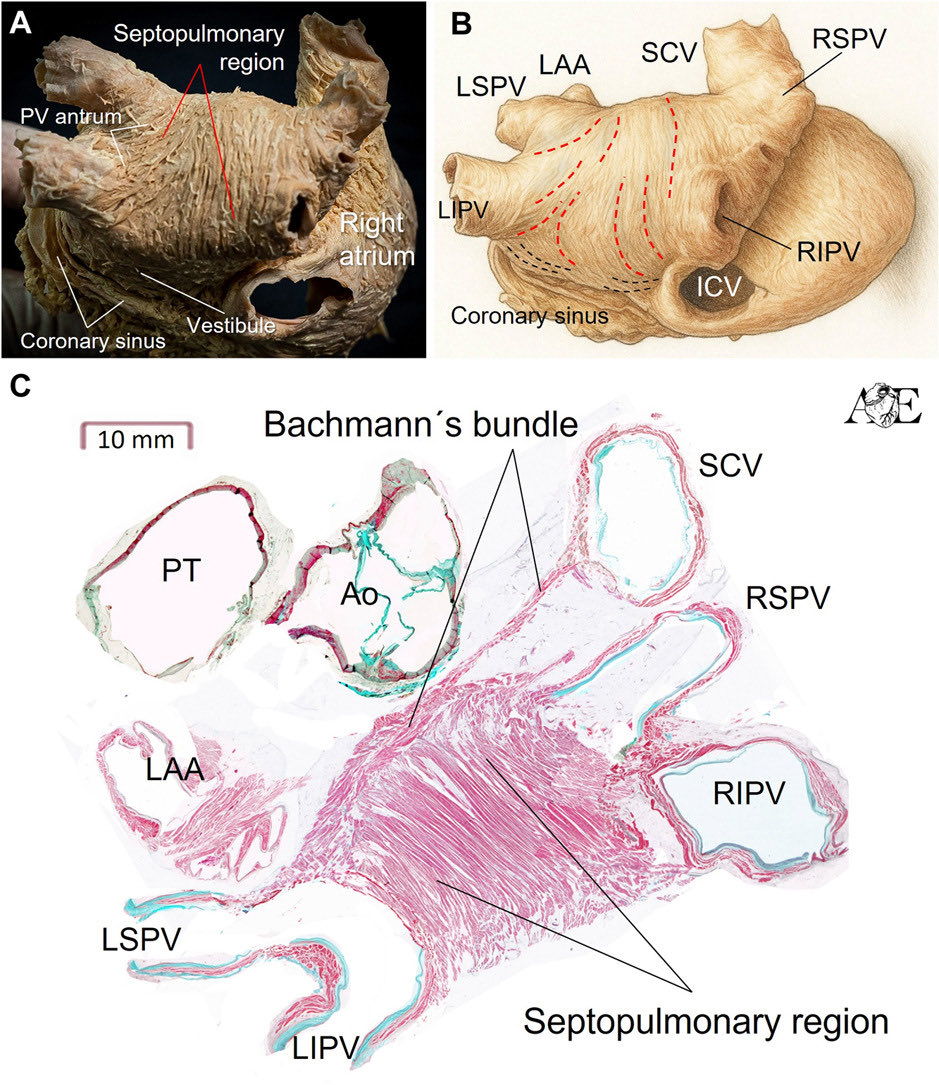
The rightward extension of Bachmann’s bundle
In this new #DaVinciAnatomyCorner@JACCJournals chapter, we explore its anatomy and clinical implications for physiological atrial pacing (BB pacing) @cardiac_anatomy
We hope you find it useful .
https://t.co/typfGFxizz
🚨 Can serial CMR redefine risk stratification in HCM?
A new study suggests that it may not be the amount of fibrosis alone that matters—but how quickly fibrosis progresses over time.
Researchers followed 313 patients with hypertrophic cardiomyopathy (HCM) who underwent two CMR scans approximately 4 years apart, assessing changes in late gadolinium enhancement (LGE), a marker of myocardial fibrosis.
🔍 Key findings
📈 Myocardial fibrosis increased substantially over time:
Median LGE mass increased from 2.9 g to 8.3 g
LGE prevalence rose from 72% to 91%
Extensive fibrosis (LGE ≥15%) doubled from 7% to 15% of patients.
⚠️ Nearly 70% of patients without LGE at baseline developed fibrosis on follow-up CMR.
💡 The most important finding was the rate of fibrosis progression:
ΔLGE >1.5 g/year independently predicted adverse clinical outcomes
Patients with rapid fibrosis progression had more than a twofold increased risk of death, transplant, HF hospitalization, stroke, or aborted sudden cardiac death
Adding ΔLGE/year to conventional risk models significantly improved risk prediction and reclassification.
❤️ For hard endpoints (death, transplant, aborted SCD), a fibrosis progression rate of >3.75 g/year identified particularly high-risk patients.
🎯 Clinical implications
Current guidelines already recommend repeat CMR every 3–5 years in HCM. This study provides strong support for that recommendation and suggests that:
✅ Serial CMR should be viewed as a dynamic monitoring tool rather than a one-time assessment
✅ Fibrosis progression may identify high-risk patients who appear low-risk according to conventional risk scores
✅ Imaging intervals could potentially be personalised based on fibrosis progression rates.
📚 One particularly striking observation: patients considered "low risk" by traditional ESC or AHA/ACC criteria but showing rapid LGE progression often had worse outcomes than some patients classified as high risk with stable fibrosis.
🧬 The future of HCM risk stratification may therefore move beyond a static fibrosis threshold toward a dynamic assessment of myocardial fibrosis progression.
🏆 Premios a los mejores artículos publicados en #recintervcardiol.
El primer premio es para «Valor pronóstico del volumen global de placa valorado mediante reconstrucción 3D del árbol coronario en pacientes sin enfermedad coronaria significativa. Un estudio multicéntrico».
Recoge el premio Octavio Jiménez-Melo (@Octavio_JiMelo). ¡Felicidades, autores!
👉https://t.co/XzoF7Vrxp8
#ACISEC2026 @shci_sec@secardiologia
Transseptal puncture in cardiovascular interventions: a clinical consensus statement of the European Heart Rhythm Association, the Heart Failure Association, the European Association of Percutaneous Cardiovascular Interventions https://t.co/yjtcQGyqNz
👨🎓🧑🎓The knowledge of atrial anatomy and tissue disposition in these complex structures may enable the electrophysiologist to better understand the 👉🔹pathophysiology of left & right atrial flutter as well as 🔹to perform the ablation procedures.
🫀 Are we underestimating sudden cardiac death risk in HCM?
📊 For years, risk stratification in hypertrophic cardiomyopathy (HCM) has relied on clinical scores…
But are these models too simplistic for such a complex disease?
🔍 A recent editorial challenges the paradigm:
👉 Moving from risk scores → precision cardiology
⚠️ The problem with current models:
✔️ Based on static variables
✔️ Limited integration of imaging & genetics
✔️ “Low-risk” patients can still experience events
💡 Example:
A 5-year SCD risk of 4–6% translates to only ~0.8–1.2% per year…
👉 Small differences, big clinical uncertainty
🧠 New insight: the atrium matters
Traditionally, we focus on the LV… but:
➡️ The left atrium reflects chronic diastolic burden
➡️ Dysfunction may precede structural changes
📈 In “low-risk” HCM patients:
👉 Impaired LA strain (LA-GLS) predicted adverse outcomes
👉 Even when conventional scores were reassuring
🔬 Where are we heading?
The future of SCD prediction in HCM is multidimensional:
✔️ Advanced imaging (CMR, strain, LGE)
✔️ Genetics (variants, polygenic risk)
✔️ AI-driven ECG analysis
➡️ Not one tool… but integration of all
🚀 Take-home message:
We need to move beyond rigid risk categories and embrace a dynamic, patient-specific approach.
👉 Precision cardiology is no longer a concept—it’s becoming a necessity.
#Cardiology #HCM #SuddenCardiacDeath #CardioImaging #CMR #StrainImaging #CardioGenetics #PrecisionMedicine #AIinMedicine #CardiologyResearch #PhDLife 🧬✨
The Empirical Evidence in the Successful Anatomical Ablation of Idiopathic LV Summit Ventricular Arrhythmias: Lessons From Endocardial Mapping | JACC: Clinical Electrophysiology https://t.co/0lxZAre8a1
✨ Mitral annular disjunction (MAD): are we focusing on the right marker for arrhythmic risk? ✨
📄 Read the discussion:
📌 DOI: 10.1093/eurheartj/ehag242
💡 A thought-provoking discussion challenges a key concept in arrhythmic MVP:
👉 Is “true-MAD” really the best marker for ventricular arrhythmic risk?
⚠️ What we thought
Patients with MVP + true inferolateral MAD → ↑ risk of ventricular arrhythmias
(even after mitral valve surgery)
🤔 But here’s the problem…
🔍 MAD is extremely common
– detected in up to 96% of individuals with advanced imaging
📉 Imaging limitations
– TTE may miss true-MAD, especially small disjunctions
– poor agreement between echo and CMR
🧠 Key paradigm shift
👉 It’s not just presence of MAD
👉 It’s the mechanical consequences that matter
✔️ Systolic extent of MAD
✔️ Dynamic systolic–diastolic changes
✔️ Mechanical traction on myocardium
➡️ Leading to fibrosis and arrhythmias
❤️ Role of fibrosis
📌 Myocardial fibrosis (LGE-CMR) strongly linked to malignant arrhythmias
But often not systematically assessed
👉 So what is driving risk?
– Persistent mechanical stress?
– Pre-existing fibrosis?
🚨 Critical questions raised
• Are we overemphasizing true-MAD as a binary marker?
• Should we instead focus on quantitative and dynamic metrics?
• Do we need multimodality imaging + rhythm monitoring for proper risk stratification?
📊 Notably:
👉 No clear increase in sudden cardiac death in true-MAD group
→ challenges a simplistic interpretation of risk
🚀 Take-home message
MAD is not just anatomy — it’s mechanics + substrate + phenotype
🧩 Future direction
• Integrate CMR + echo
• Quantify systolic MAD dynamics
• Assess fibrosis systematically
• Improve arrhythmic monitoring
💬 This discussion reminds us:
👉 In cardiomyopathies and valvular disease, structure alone is rarely enough
#MVP #MAD #Arrhythmias #CardiacImaging #CMR #Echocardiography #Cardiology #Electrophysiology #CardioTwitter 💙
Recognizing the septopulmonary region not as an isolated “bundle,” but as a functional 3D myocardial architecture, is essential for interpreting mapping data & optimizing ablation strategies
@JACCJournals@DrRoderickTung@davidgzcasal@DamianSanc1955
https://t.co/nnirFWiTnc
🔍 #EHRATopicWeek on Atrial Tachycardias
Atrial Tachycardia is more complex than we once thought
Traditionally, rapid regular atrial arrhythmias were divided into “atrial tachycardia” and “atrial flutter” based mainly on ECG appearance. Today, high-resolution mapping shows these distinctions are often oversimplified.
📌 Current concepts classify all regular atrial rhythms >100 bpm as AT:
• Non-reentrant AT
• Reentrant AT (localized or macro-reentrant)
Importantly, many arrhythmias previously labeled as “flutter” may actually represent different AT mechanisms.
⚡ Differentiating AT from organized AF can be challenging, especially in scarred atria or after ablation. ECGs, EP studies, intracardiac mapping, and even wearable devices all play an important role in diagnosis.
💡 Precise classification matters — for diagnosis, treatment strategy, and improving ablation outcomes.
Find out more in the #EHRA_ESC Consensus document on Management of patients with atrial tachycardia 🔗https://t.co/T5EGaHI51q
@escardio@EuropaceEiC
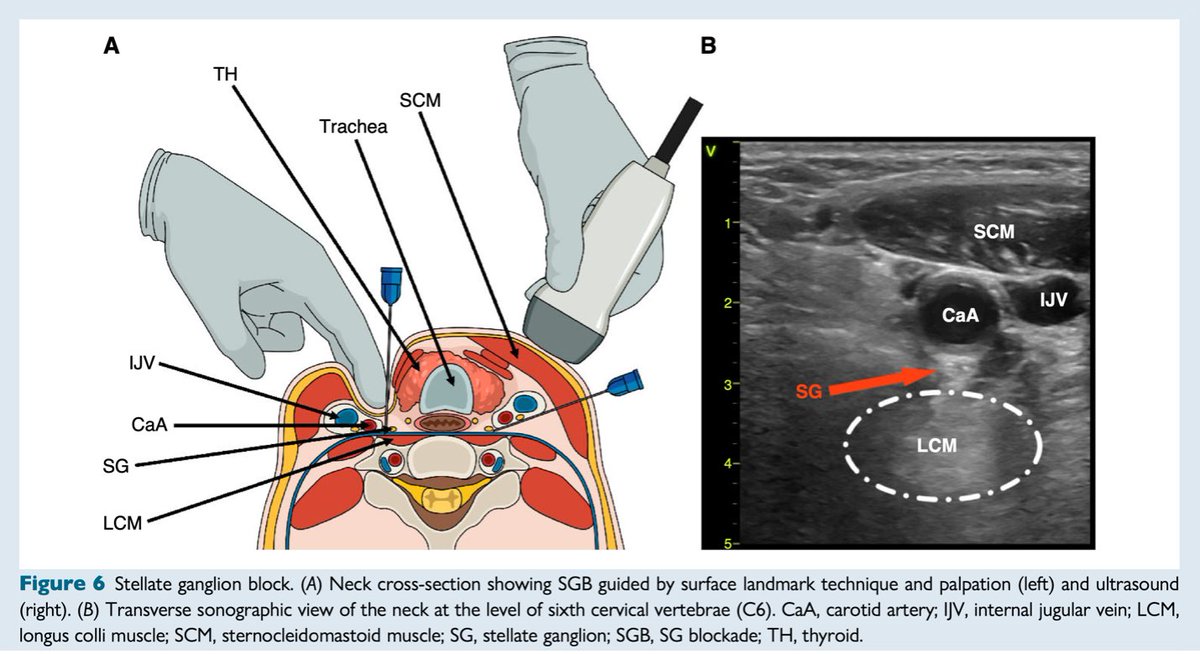
#EHRAtopicweek on electrical storm⚡
What to do when amiodarone and propranolol fail and catheter ablation is not feasible? Stellate ganglion block may be helpful.
Read more #Europace
https://t.co/gLhrxbQX3M
@EuropaceEIC
🫀✨ Rethinking QTc: time to move beyond Bazett?
A new study in the Journal of the American Heart Association evaluated QTc correction formulas in >3200 healthy Asian young adults (18–22 yrs) — and the results are striking.
📊 Key findings:
🔹 Bazett formula → ❌ strongest heart rate (HR) dependence & poorest consistency
🔹 Dmitrienko → 👍 best HR independence
🔹 Framingham & Rautaharju → 🤝 highest agreement
🔹 Framingham → ⭐ best overall performance across HR ranges
⚠️ Bazett tends to:
➡️ Overestimate QTc at high HR
➡️ Undercorrect at low HR
➡️ Potentially mislead clinical decisions
✅ Take-home message:
👉 The Framingham formula emerges as the most robust and clinically reliable method, especially in young populations.
📢 This study supports a shift toward precision-based QTc correction and challenges the routine use of Bazett in modern practice.
💡 Why it matters?
Better QTc correction = better risk stratification, safer drug use, and improved arrhythmia assessment.
#Cardiology #QTc #ECG #Arrhythmia #PrecisionMedicine #HeartRate #CardioTwitter #MedEd #YoungAdults #ClinicalResearch #Electrophysiology #CardioInsights 🫀📈
Epicardial ventricular arrhythmia ablation: a clinical consensus statement of the European Heart Rhythm Association of the European Society of Cardiology and the Heart Rhythm Society, the Asian Pacific Heart Rhythm Society, the Latin American Heart Rhythm https://t.co/8HORHM2bD8
🚨 IVIG vs Steroids in pediatric myocarditis: are we finally getting clarity?
Acute myocarditis in children remains a clinical grey zone —
from diagnosis to treatment decisions.
👉 Supportive care is standard…
but what about immunomodulatory therapy?
✨ This new network meta-analysis (2850 children) provides important insights 👇
📊 Key findings:
✔️ IVIG reduces mortality (in-hospital, long-term, overall)
✔️ Improves cardiac function (↑ LVEF, ↓ LV dilation)
✔️ Best-ranked treatment across major outcomes
❌ Steroids?
➡️ No clear benefit
➡️ No improvement in survival
➡️ Combination with IVIG not superior
📉 IVIG reduced overall mortality by ~50% compared to standard therapy
💡 But nuance matters:
🔹 Evidence quality still limited (few RCTs)
🔹 Possible benefit of steroids in fulminant cases
🔹 Heterogeneity in diagnosis and treatment strategies
🎯 Take-home message:
IVIG may be the most effective adjunctive therapy in pediatric acute myocarditis —
while routine steroid use should be approached with caution.
💬 How do you manage myocarditis in children in your centre? IVIG for all or selected cases only?
#Cardiology #PediatricCardiology #Myocarditis #IVIG
#HeartFailure #CriticalCare #EvidenceBasedMedicine
#CardioTwitter #MedEd #Research #Paediatrics ❤️🫀
https://t.co/1oa48gKZXn
Antiarrhythmic drugs versus catheter ablation as rhythm control for atrial fibrillation: a systematic review and meta-analysis of randomized controlled trials #OpenAccess
https://t.co/vZoCyEp8Hb