🧬 EHA2026 | Precision Hematology
🎤 Speaker: Sören Lehmann
🧪 Topic: Treatment strategies in TP53-mutated AML/MDS
🚨 TP53-mutated AML/MDS remains a major therapeutic challenge
💊 VEN + HMA has become a common standard approach in TP53-mutated AML
📌 Reported with VEN/HMA:
CR rates ≈ 43–67%
EFS ≈ 6–7 months
OS ≈ 5–7 months
⚠️ VIALE-A signal:
VEN/AZA improved response in TP53-mutated AML vs AZA alone
But OS remained short and similar ≈ 6 months
🧠 Key message:
VEN/HMA increases remission rate
But remissions are often short
And survival remains poor
💉 HMA monotherapy in TP53-mutated disease:
AZA CR ≈ 20–40%
Decitabine CR ≈ 30%
Median OS often ≈ 7 months
📌 In MDS:
Lower TP53 VAF = better survival
Platelets >50 ×10⁹/L = better OS
🔥 Intensive chemotherapy in TP53-mutated MN is limited
3+7 chemotherapy:
CR ≈ 20–48%
Median OS ≈ 4–9 months
3-year survival ≈ 1–8%
⚠️ CPX-351 does not appear to overcome TP53-mutated chemoresistance
📊 Meta-analysis message:
IC, HMA, and VEN/HMA may produce CR/CRi
But OS remains clustered around very short medians
🧪 Metronomic VEN/AZA is emerging in TP53-mutated AML/HR-MDS
📌 Presented regimen:
Azacitidine 0.2 mg/kg SC weekly
Venetoclax 400 mg PO days 1, 8, 15, 22
28-day cycles
📊 Cohort: VEN/AZA-naïve HR-MDS n=26 + AML n=14
Median age ≈ 76.5 years
82% had biallelic TP53 mutations
✅ Outcomes:
AML OS ≈ 11.6 months
HR-MDS OS ≈ 9.9 months
48% of responders became MRD negative
Low toxicity reported
⚠️ Neutropenic fever ≈ 15%
No therapy-related fatalities
100-day mortality ≈ 7.5%
🎯 Clinical takeaway:
For TP53-mutated AML/MDS, higher response does not always mean durable survival
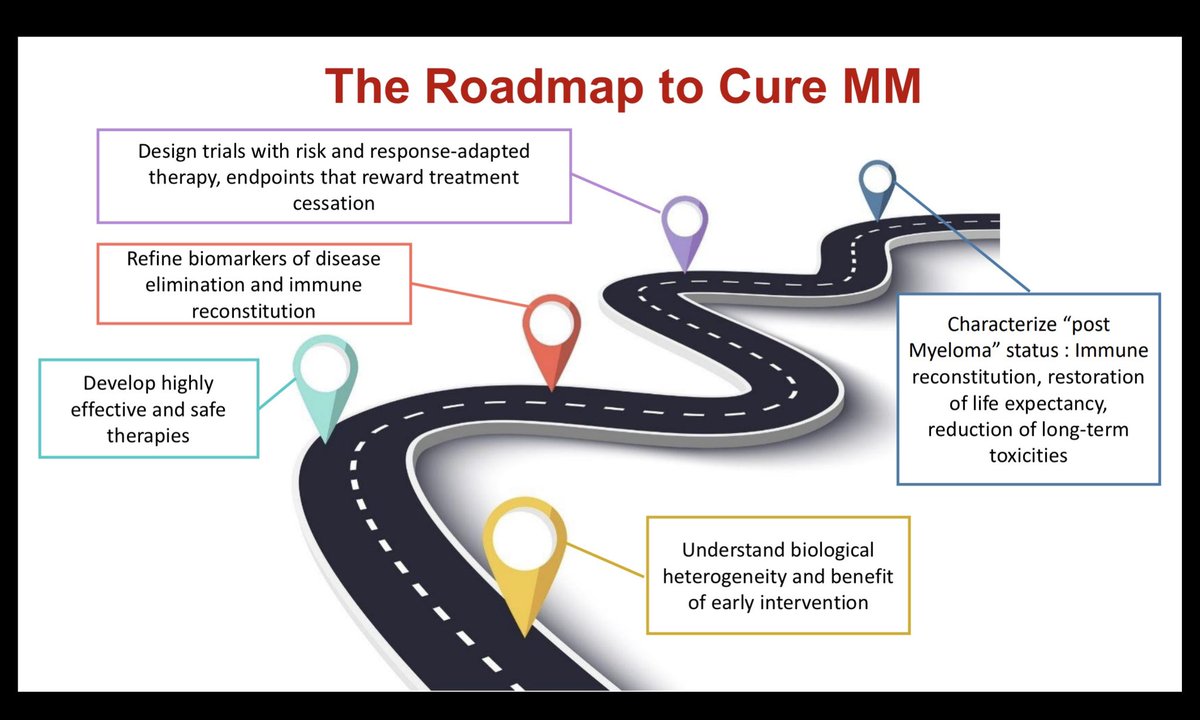
💡 Precision treatment must focus on:
depth of response 🧬
MRD negativity 🔍
toxicity balance ⚖️
bridging to transplant when feasible 🧫
novel TP53-directed combinations 🚀
#EHA2026 #PrecisionHematology #TP53 #AML #MDS #HRMDS #Venetoclax #Azacitidine #HMA #MyeloidMalignancies #Hematology #KFSHRC #ESH
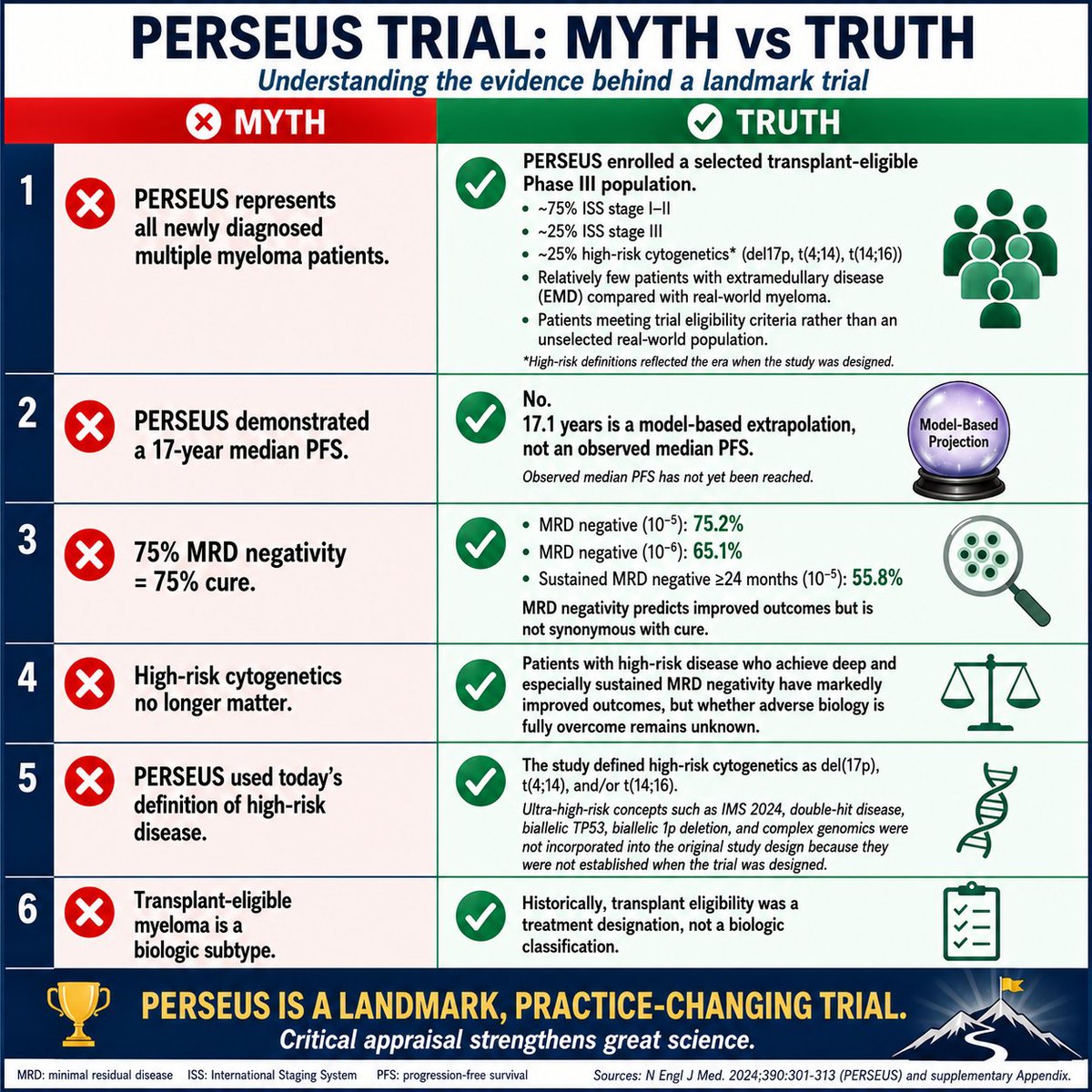
Landmark trials deserve landmark scrutiny.
The PERSEUS trial has transformed frontline treatment for transplant-eligible multiple myeloma and established a new standard of care.
But practice-changing does not mean scientific discussion should stop.
As clinicians and educators, we should distinguish observed evidence from model-based projections, MRD negativity from cure, and trial populations from real-world patients.
This PSNS Myth vs Truth summarizes six common misconceptions surrounding PERSEUS.
The goal is not to criticize a landmark trial.
The goal is to better understand it.
Great science welcomes thoughtful discussion.
#MultipleMyeloma #Medwatch
I think this is the best evidence we’re going to get, and it probably settles the issue. We need to move forward with different strategies.
Congratulations to the authors!
https://t.co/xPzZ7mRDdr
#EHA2026
HD-MTX for CNS prophylaxis in high-risk DLBCL? The answer is finally here.
3-yr CNS relapse: 6.6% (HD-MTX) vs 6.7% (no HD-MTX). Adjusted HR 0.95 (0.62–1.44).
Isolated CNS relapse: HR 0.81 (0.50–1.33).
n=1,923 UHR patients. No difference. None.
Time to move on. #EHA2026
PFS is not always OS.
One of the biggest misconceptions in oncology is assuming that delaying progression automatically means patients live longer.
Many strategies consistently improve:
• PFS
• depth of response
• MRD negativity
…but OS often barely moves.
Examples:
• Upfront vs delayed AutoSCT
• Lenalidomide maintenance
• HD melphalan intensification
• Many maintenance strategies in lymphoma
Why?
Because:
• crossover therapies matter
• salvage therapies work
• toxicity matters
• resistant clones survive
• biology evolves
A longer remission is meaningful.
But it is not always a longer life.
The critical question is no longer:
“Did the curve separate?”
The question is:
“What happened to OS?”
#MultipleMyeloma #lymphoma #CART #Hemtwitter
Dr. Fun + G
The future question in myeloma may not be:
“Transplant or no transplant?”
It may be:
“Which biology deserves a different first strike?”
Modern quadruplets and AutoSCT produce deep responses, but emerging real-world genomic-risk data suggest that biologically ultra-high-risk disease, especially TP53-abnormal myeloma, may still relapse early despite MRD negativity.
If “high-risk” patients already have median PFS ~2–3 years…
what happens in true bi-allelic TP53 disease?
A cartoon reflection on del17p / TP53-mutated myeloma, modern quadruplets, and the emerging frontline CAR-T debate. 🧬☕🚀
Inspired by recent IMS/IMWG genomic-risk real-world outcomes data from the MSKCC cohort.
#MultipleMyeloma #Hemetwitter #CAR_T
TP53 in MDS is not binary.
It’s a spectrum.
And we’re oversimplifying it !
Large SCT dataset confirms:
• TP53-mut = adverse
• “Biallelic” = worst
Important work.
But the biology is more nuanced.
Monoallelic TP53?
Bad.
But how bad?
We all have long-term SCT survivors →
👉 suggests residual function / heterogeneity
True biallelic (multi-hit)?
• Functional TP53 loss
• Genomic instability
• Near chemo-resistant state
👉 Very difficult to rescue, even with SCT
But here’s the issue:
“Biallelic” often defined as VAF >50%
👉 Useful shortcut
👉 Not biology
VAF >50% ≠ biallelic
VAF reflects:
• Tumor purity
• Clonal dominance
• Copy number
A dominant monoallelic clone
can look like “50%”
More importantly:
👉 What if TP53 is a 10% subclone?
Different biology:
• Less genomic dominance
• Less clonal fitness
👉 GVL may still control this
So TP53-mut disease is not one entity:
• Monoallelic dominant
• True multi-hit
• Small subclonal TP53
➡️ Different biology
➡️ Different outcomes
Retrospective studies like this are critical
—but limited by simplified definitions
TP53 is a spectrum
VAF is not allelic state
True biallelic = genomic collapse
Subclonal TP53 → may be GVL-sensitive
See figure 👇
Dr Fun + G
#MDS #AML #Hemetwitter
Vamos perdiendo la batalla más importante en las aulas... la capacidad de leer un texto largo sin desconectar. No es que los alumnos no sepan leer; es que han perdido el hábito de la paciencia. Sin lectura no hay comprensión, y sin comprensión solo hay la NADA. 🧵va...
Check out the full paper for more detailed insights !
https://t.co/2a0hnlqyNa
Thanks for following, thanks to my co-authors 🙏@vkprasadlab
Also covered here : https://t.co/CxT5UTILI8
Subscribe for free to my letter!
16/16
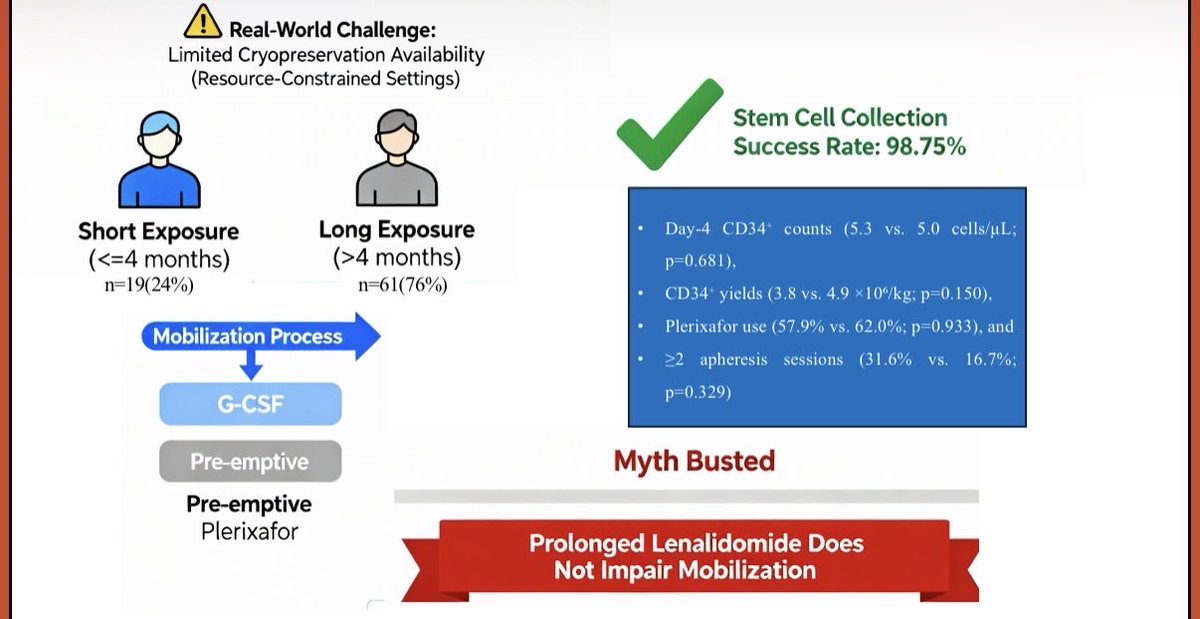
👉🏻👉🏻📖Our work on stem cell mobilisation in multiple myeloma is now published in Leukemia & Lymphoma!
Full text:
https://t.co/DxncQdso1I
📊 Highlights:
• 80 NDMM patients undergoing ASCT
• 97% successful mobilisation with G-CSF + plerixafor
• No difference in CD34 yield between ≤4 vs >4 months lenalidomide
• Even extended exposure (>10 months in ~30%) did not compromise outcomes
• Practical, cost-effective strategy for resource-limited settings
⚠️ Caution: prolonged DARA-VRd may be associated with lower CD34 yields and higher plerixafor need—plan mobilisation carefully.
💡 Implication:
We may not need early collection or lenalidomide interruption in the plerixafor era—a major shift for real-world practice.
🔗 DOI: https://t.co/jGUhcyTMar
Thank you @DrPMPGI@LeukemiaLymph
#hematology #ASCT #myeloma #stemcell @MM_Hub@TheEBMT@SikshyaO@MirghSumeet@IndMyAcGp
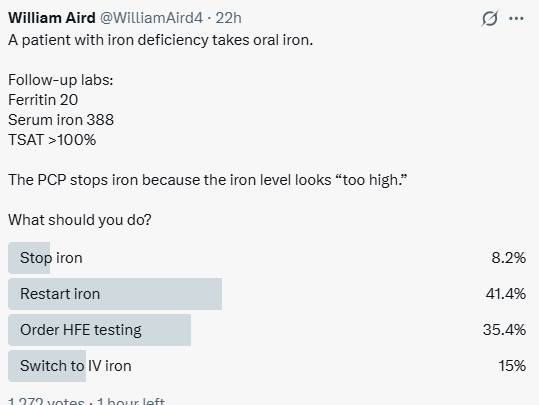
The Fe Paradox: High Serum Fe in Fe Deficiency
Poll results are in (≈1,200 votes).
Iron deficient patient with:
Ferritin 20
Serum Fe 388
TSAT >100%
The PCP stopped oral Fe because the Fe looked “too high.”
Interesting split in responses.
Let’s walk through the physiology.