Jewish UK NHS Doctor Says Colleagues Would Refuse To Save Dying Israelis:
A Jewish doctor working in Britain’s National Health Service told ITV News that fellow doctors said they would refuse to treat Israeli patients, including in life-threatening emergencies. The doctor, also said he witnessed Jewish patients being denied kosher meals and is now preparing to move to Israel with his family, citing rising antisemitism in Britain.
Ya van 10 días de la detención en libia de los 10 idiotas que quisieron llegar vía Egipto a Gaza
Ni una sola denuncia de secuestro
Ni una sola condena institucional de ningún país
Ni una solo grupo organizándose para ir a buscarlos o hacer marchas ante la embajada de libia
Silencio total, ser anti israelí compulsivo y hacer silencio de todo lo que no se puede criticar a israel DA ASCO
Diez miembros, entre ellos una española, del convoy terrestre de la flotilla pro Hamás fueron detenidos por milicias libias HACE ONCE DÍAS y acaban de ver extendida su prisión (que vayan preguntando los @GPPopular y @VOX_Congreso en la Comisión de Exteriores a @jmalbares cuanto nos va a costar a los españoles el pago del rescate de la activista antisemita).
Por otro lado, no hemos visto un clamor global ni una cobertura obsesiva por parte de los medios.
Nos preguntamos por qué.
Previewing some data that will report at next week's American Diabetes Association Scientific Sessions:
Pfizer's monthly GLP-1 berobenatide phase 2b trial in adults with obesity. Both those with type 2 diabetes and without type 2 diabetes.
Top line results report 12.3% weight loss at week 28.
Looking forward to VESPER-3 presentation June 6th
https://t.co/741edHlVcR
El Ministerio de Interior ha presentado el Informe de Delitos de Odio del año pasado cuya tendencia en el aumento del antisemitismo coincide con los datos del Observatorio de Antisemitismo que próximamente publicará su informe. @interiorgob
🚨 Should obesity always be considered a disease?
A provocative new Nature Comment argues that the answer is no.
Francesco Rubino, chair of the 2025 Lancet Commission on Clinical Obesity, challenges the growing movement to classify all obesity as a chronic disease. Instead, he proposes a more nuanced framework distinguishing clinical obesity from preclinical obesity, with major implications for diagnosis, treatment, health policy, and research.
The central argument
For years, obesity was viewed primarily as a risk factor for diabetes, cardiovascular disease, cancer, and premature mortality.
More recently, advocacy groups and professional societies have increasingly promoted obesity as a chronic disease to reduce stigma and improve access to treatment.
However, Rubino argues that this shift may oversimplify a highly heterogeneous condition.
Two individuals with exactly the same BMI can have dramatically different health states:
✅ One may have preserved organ function and remain healthy for decades.
❌ Another may experience heart failure, respiratory impairment, metabolic dysfunction, and severe mobility limitations.
Yet current classifications often place both under a single disease label.
Clinical vs Preclinical Obesity
The 2025 Lancet Commission proposed a distinction:
🔴 Clinical obesity
Excess adiposity directly causes organ dysfunction
Impairs daily activities
Produces measurable physiological abnormalities
Represents a true disease state
🟡 Preclinical obesity
Excess adiposity is present
Organ function remains preserved
Future risk is elevated
Disease has not yet developed
This framework treats risk as risk and disease as disease.
Why BMI alone is insufficient
The article emphasizes that obesity differs from diseases such as diabetes or COVID-19.
Classic diseases are usually defined through:
Consistent symptoms
Predictable clinical trajectories
Shared biological mechanisms
Obesity lacks this uniformity.
BMI predicts population-level risk but often fails to predict:
Individual prognosis
Current health status
Treatment response
Underlying biology
As a result, obesity cannot always be interpreted as a disease at the individual level.
The biological argument
Another key point:
There is no single biological abnormality shared by all people with obesity.
While genetics, environment, aging, sleep disruption, medications, and food environments contribute, obesity represents multiple biological pathways rather than one disease mechanism.
The success of GLP-1 receptor agonists demonstrates that body weight is biologically modifiable—but not necessarily that every case of obesity constitutes disease.
Policy implications
The consequences are enormous.
If every person with obesity were classified as having a chronic disease:
Hundreds of millions could become eligible for lifelong treatment
Health systems could face unsustainable costs
Access criteria might become increasingly arbitrary
Some individuals may receive therapies with limited clinical benefit relative to risk
The author argues that treatment intensity should be proportional to demonstrated disease burden rather than BMI alone.
Take-home message
The debate is not whether obesity can be a disease.
The debate is whether all obesity should be considered disease.
Rubino argues that diagnostic precision matters:
Clinical obesity = disease.
Preclinical obesity = elevated risk, but not disease.
Recognizing this distinction could improve patient-centered care, sharpen research, reduce overtreatment, and create more sustainable health policy.
Reference
Rubino F. Why obesity shouldn’t always be considered a disease. Nature. 2026;654:33–36.
#Obesity #GLP1 #MetabolicHealth #Endocrinology #PublicHealth #PrecisionMedicine #ObesityMedicine #NatureJournal #Metabolism #HealthcarePolicy
Palestinian terrorists in Gaza are using an elementary school as a terror base and moving weapons from a tunnel shaft leading into Hamas’ underground terror tunnel.
Share this. The mainstream media won't.
🧠 La obesidad no suele ser un problema de falta de leptina, sino de resistencia a la leptina.
Aunque los niveles de leptina están elevados, el cerebro deja de interpretar la señal de saciedad.
Resultado:
🍽️ Más hambre
📉 Menor gasto energético
⚠️ Problemas con el peso
Nuevo estudio (UK Biobank, 24.000 personas) en síndrome cardio-reno-metabólico:
El riesgo cardiovascular que queda tras aplicar los modelos clásicos tiene firma molecular. Y es inflamatoria.
63 proteínas (inflamación, daño renal, remodelado) → 2,5× más riesgo CV.
La inflamación no es ruido de fondo. Es el eje.
Diabetes Obes Metab. 2026. https://t.co/6b9U5k212Q
¿Por qué importa vacunar de gripe a las personas con diabetes?
Mayor vulnerabilidad inmunitaria, peor control metabólico y más eventos cardiovasculares.
La vacunación anual reduce hospitalizaciones, MACE y mortalidad, es coste-efectiva y puede ayudar frente a la resistencia antimicrobiana.
Revisión en @endocDiabNutric
👇
🔗 https://t.co/rO3ylqlqn7
Phase 3 obesity data at #ADA Scientific Sessions this week 📉
Survodutide (Boehringer Ingelheim / Zealand Pharma), a glucagon/GLP-1 dual agonist 💉
16.6% weight loss at 76 weeks vs 3.2% with placebo in phase 3 SYNCHRONIZE-1 🔥
Excited to see full SYNCHRONIZE-1 + SYNCHRONIZE-MASLD data at ADA.
Curious to compare fat-mass vs lean-mass loss ratio & liver fat reduction to other related incretin mimetics
🔗 https://t.co/kMxxKKsR5G
Este interesante paper nos acerca a
#MASLD: una epidemia cardiometabólica global🌍 íntimamente ligada a la #obesidad y #DM2.
Afecta a ~33% de la población adulta mundial, pero en el caso de #personas con #DM2 la prevalencia es ≈ 65%.
Toca estar atentos a este entidad.👀
#Obesity is increasingly managed with medications as disease-modifying therapies, reflecting its role as a gateway disease driving metabolic, cardiovascular, reproductive, neuropsychiatric, and mechanical conditions https://t.co/IFPyEU8bKn
#weightloss#GLP-1 receptor agonists
I had a patient last month who did everything right. 60 lbs down on tirzepatide. A1c from 6.4 to 5.3.
She told me: "I'm scared my body is just waiting to take it all back."
Six new papers just proved her right.
Weight regain isn't moral failure. It's cellular memory.
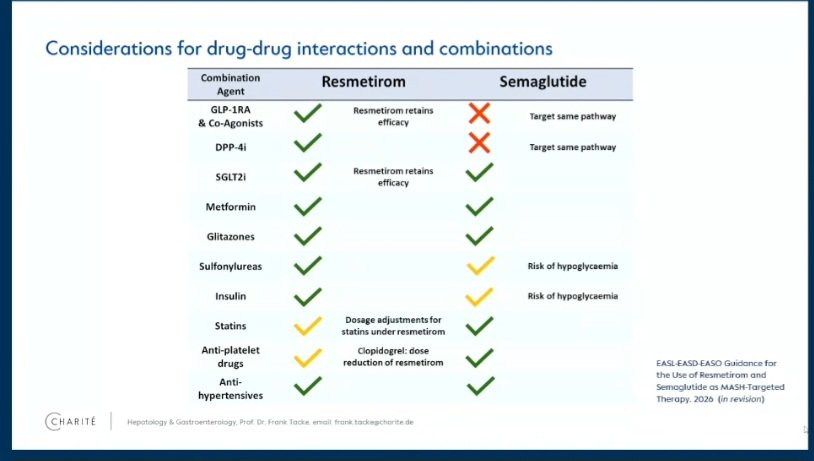
Preview of upcoming EASL-EASD-EASO guidance at EASL congress 2026. Full publication will be out within the next 4 to 6 weeks. Exciting time ahead for treatment of MASLD.
Insulin resistance is often reduced to “high glucose”. But that is only the surface of the problem.
Insulin is not simply a hormone that lowers blood sugar.
It is a systemic anabolic signal.
After a meal, insulin tells the body that nutrients are available and that energy can be stored, used, or redirected.
In skeletal muscle, insulin promotes glucose uptake through GLUT4 translocation.
This is one of its most familiar actions: glucose leaves the bloodstream and enters muscle fibres, where it can be oxidised or stored as glycogen.
In the liver, insulin suppresses glucose production.
It inhibits gluconeogenesis and glycogen breakdown, while favouring glycogen synthesis. In other words, after eating, the liver should stop behaving as if the body were fasting.
In adipose tissue, insulin inhibits lipolysis.
It tells fat cells not to release fatty acids into the circulation, because energy is already abundant. At the same time, it favours lipid storage.
But insulin also regulates protein metabolism, vascular tone, mitochondrial function, inflammation, and cellular growth pathways. It is not a “glucose hormone”; it is a metabolic coordinator.
Insulin resistance appears when tissues no longer respond adequately to that signal.
The pancreas compensates by secreting more insulin, often for years. This creates a paradox: insulin levels are high, but insulin action is incomplete.
The consequence is not uniform failure.
Some insulin pathways become resistant, while others remain active. Glucose uptake in muscle may fall, and hepatic glucose production may remain inappropriately high. Yet lipogenesis in the liver can continue, contributing to fatty liver and hypertriglyceridaemia.
Meanwhile, adipose tissue releases more fatty acids, feeding hepatic fat accumulation and interfering with insulin signalling in muscle and liver. Chronic low-grade inflammation, ectopic lipid deposition, mitochondrial stress, and adipokine imbalance amplify the loop.
This is why insulin resistance is not just a prelude to type 2 diabetes. It is a whole-body disorder of nutrient partitioning.
Insulin resistance means that the body hears abundance, but its tissues behave as if the message were distorted. The problem is not only excess sugar in blood, but a loss of metabolic synchrony.
🕯️ October 7, 2023. We Will Never Forget 🕯️
More than 1,200 people were brutally murdered in southern Israel in the Hamas terrorist massacre. 251 men, women, children, and elderly were taken hostage. 364 young people were massacred at the Nova Music Festival. Over 20 communities and multiple military bases across southern Israel came under attack.
October 7, 2023, was the deadliest day for the Jewish people since the Holocaust.
Hamas terrorists tortured, raped, burned families alive, kidnapped babies and grandparents, and celebrated these atrocities.
We remember every life stolen. We will never forget. 🕯️
Jojojojojo…
🥷🏻🇨🇳 Flotilleros de la @globalsumudflotilla “La flotilla de los condones” secuestrados en Libia por milicias Armadas Árabes Libias.
No oíste nada porque la prensa lo oculta
‼️Pero como no ha sido 🇮🇱Israel. No tiene interés.‼️