TCD with bubble has the highest sensitivity to detect a right to left shunt and TEE with bubble has the highest specificity to diagnose a PFO. Cardiac CT has low sensitivity for PFO. Great work by @nbavar https://t.co/Ei4eLqqEoB
💡 What is the current evidence on coil-only middle meningeal artery embolization (MMAE) for chronic subdural hematoma (cSDH)?
In this JNIS scoping review, authors analyzed 9 studies including 367 patients and 459 embolization procedures evaluating coil-only MMAE for cSDH.
Recurrence rates ranged from 0–17.6%, reintervention rates from 0–15.4%, and complication rates from 0–5%. Techniques varied from proximal MMA trunk occlusion to more distal branch-level coiling, with potential advantages of coil-only MMAE in anatomically challenging cases.
📖 Read more at https://t.co/qDwB9jTRUn
@HakeemShakirMD@OUHealth
In EVT treated M2 occlusion stroke, larger Tmax >4 s perfusion deficit was associated with worse 90-day functional outcomes.
Tmax >4 s volume >113 mL best discriminated outcomes.
MAD-MT study by @vsyedavalli@NANConsortium
https://t.co/QCLfSvIu6F
Should we treat medium-vessel occlusion (MVO) strokes with endovascular thrombectomy?
Previous trials said no, but the new ORIENTAL-MeVO trial reveals a specific group of patients who actually benefit.
Here is the breakdown of the latest findings:
THE CONTEXT
Early endovascular trials focused on large-vessel occlusions, where the clinical benefit of reperfusion is substantial. However, three recent trials for medium-vessel occlusions, such as ESCAPE-MeVO and DISTAL, showed no clinical benefit for thrombectomy over standard medical care.
THE NEW DATA
The ORIENTAL-MeVO trial analyzed 563 patients in China and found a significant advantage for thrombectomy. At 90 days, 58.6% of the thrombectomy group achieved functional independence compared to 46.6% in the control group.
WHY THE DIFFERENCE?
Patient selection is the defining factor. Compared to previous neutral trials, the patients in ORIENTAL-MeVO had distinct characteristics:
🔹 They were younger, median age of 71
🔹 They had higher baseline stroke severity, presenting with a median NIHSS score of 10
🔹 They were less likely to receive intravenous thrombolysis, which may have unmasked the true benefit of the endovascular procedure.
THE TAKEAWAY
Most patients with medium-vessel occlusion strokes will not benefit from endovascular thrombectomy because a small baseline deficit leaves little room for clinical improvement. However, patients presenting early with a higher stroke severity, a younger age, and who do not receive concurrent thrombolysis are the optimal candidates for this intervention.
Reference:
@johanna_ospel Ospel JM, Hill MD. Endovascular Therapy for Medium-Vessel Occlusion Stroke — Narrowing the Target Population. N Engl J Med. 2026;394(19):1955-1957.
https://t.co/5opl9ZT1j7
@ThienHuynh15@MichelleLinMD@SWEnglishMD@KevinMBarrettMD@RabihTawkMD
To call it or not to call it? That is the question!
Do you feel a bit wacky & wobbly when it comes to calling normal pressure hydrocephalus on imaging?
You don’t want to overcall it, but you don’t want to miss it either!
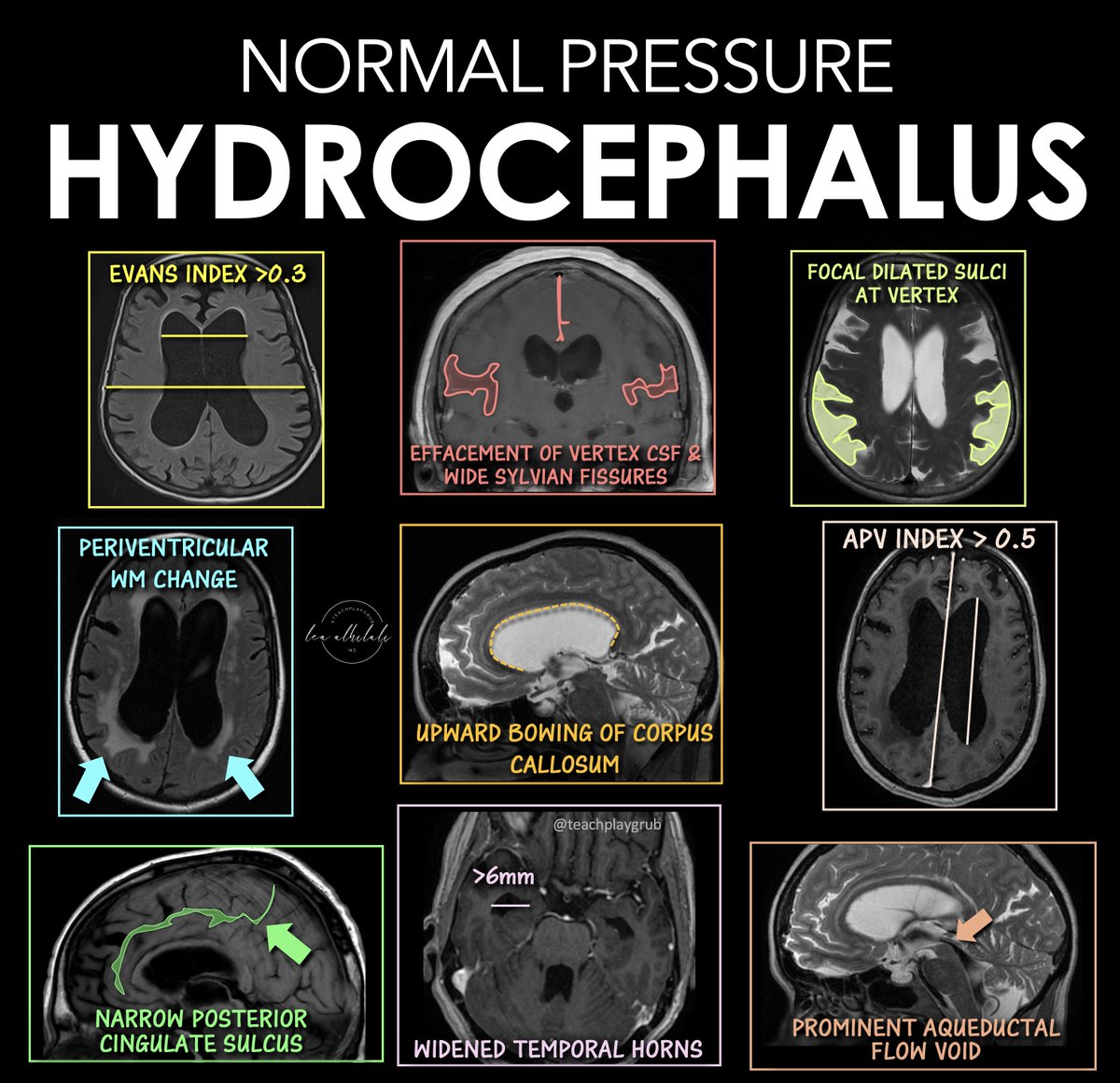
Here are the signs of NPH
🔹 Evans Index > 0.3
--Enlarged frontal horns relative to skull width → ventriculomegaly.
Remember it: “One out of three is too big for me!”
🔹 Periventricular White Matter Change
--T2/FLAIR hyperintensity from transependymal CSF flow.
Remember it: “Leaking pressure leaves a glow.”
🔹 Narrowing of the Posterior Cingulate Sulcus
--Tight high-convexity sulci from crowding at the vertex.
Remember it: “The top gets squeezed shut.”
🔹 Effaced Vertex CSF + Wide Sylvian Fissures
--Tight sulci up top but enlarged fissures laterally (DESH pattern).
Remember it: “Dry on top, wet on the sides.”
🔹 Upward Bowing of the Corpus Callosum
--Ventricular expansion pushes the corpus callosum upward.
Remember it: “If the corpus callosum is arched, the patient can’t march (wobbly)”
🔹 Temporal Horns > 6 mm
--Early temporal horn dilation from hydrocephalus.
Remember it: “Big horns before big vents.”
🔹 Focally Dilated Sulci at the Vertex
--Patchy enlarged sulci despite surrounding crowding.
Remember it: “Holes in a leaky roof = too much water on the brain!”
🔹 APV Index > 0.5
--Increased ventricular-to-parenchymal proportion suggesting hydrocephalus.
Remember it: “Glass half full is too much!”
🔹 Prominent Aqueductal Flow Void
--Increased CSF flow through the aqueduct on MRI.
Remember it: “If the aqueductal flow is super black, the ventricles are out of whack.”
Classic NPH imaging theme: enlarged ventricles + tight high convexities + disproportionate CSF redistribution.
Hopefully now you won't wobble on the diagnosis of NPH!!
Paclitaxel Drug-Coated Balloon Angioplasty for Medically Refractory Intracranial Atherosclerotic Disease: A US Single-Center Experience With the AGENT Balloon
https://t.co/8caq7LSv3G
Just Published
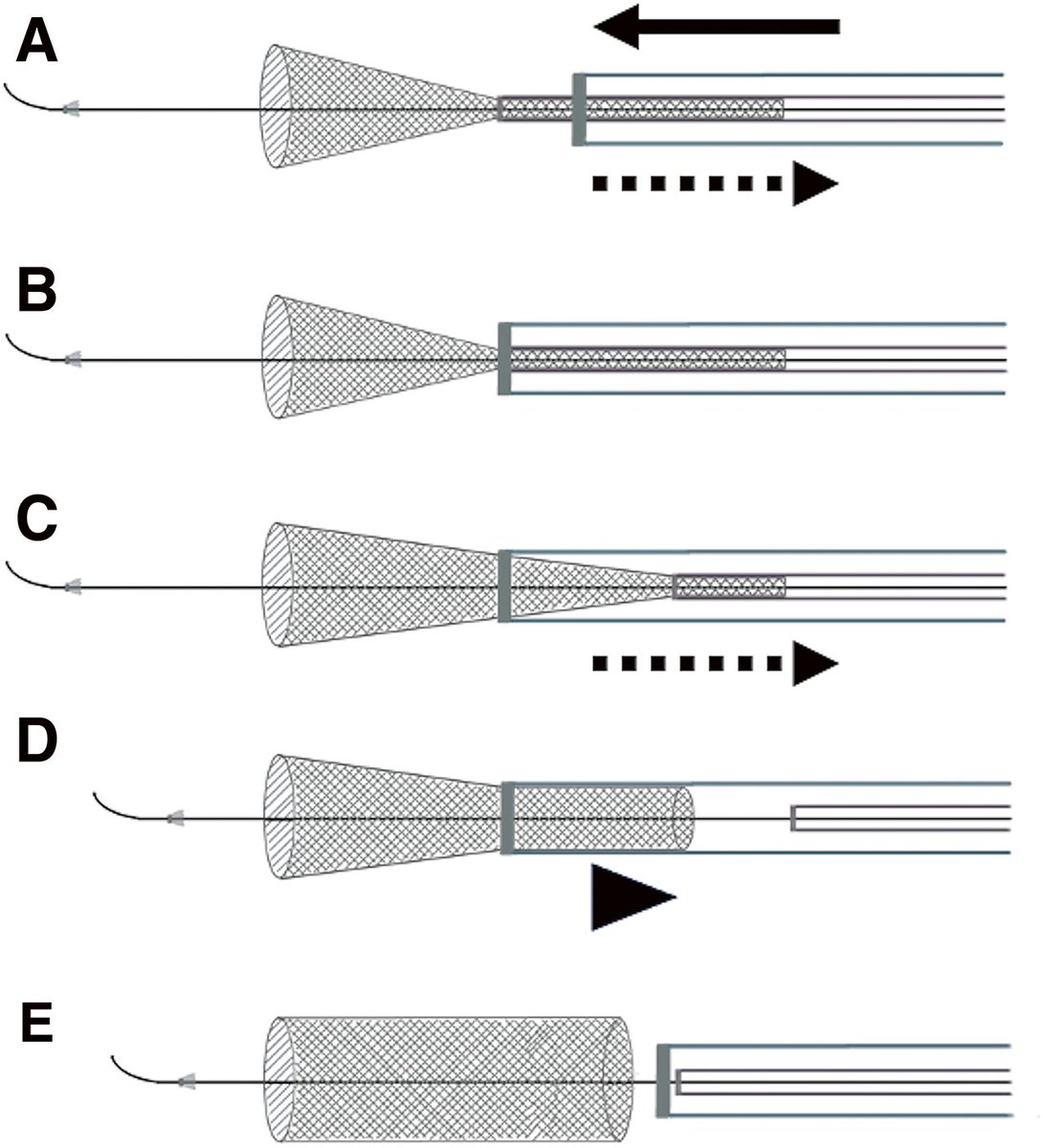
Intra-Distal Access Catheter Deployment of the Surpass Evolve Device: A Novel Technique to Prevent Advancement of the Delivery Wire: A Case Report and Literature Review
https://t.co/vWqw3FTZie
#Neuroendovascular
Tenzingplasty 💪 🎉
"All treated segments had improved narrowing, with 78 (95.1%) having residual narrowing <50%. No procedural complications occurred."
https://t.co/3iWBA3W3Hd
🧠 ESTENOSIS CAROTÍDEA ASINTOMÁTICA: ¿Cuándo revascularizar en 2026?
1️⃣ El riesgo de ictus ipsilateral en estenosis ≥70% bajo terapia médica intensiva es ~1.5%/año (CREST-2, NEJM 2026) — mayor de lo estimado por estudios observacionales previos (0.5–1.0%/año).
2️⃣ CREST-2 (n=2485): Stenting redujo el evento primario vs. terapia médica sola (2.8 vs. 6.0%; NNT=31). CEA no alcanzó significancia estadística (3.7 vs. 5.3%). Ambas técnicas mostraron tasas perioperatorias similares (~1.3–1.5%).
3️⃣ La revascularización en estenosis 70–99% asintomática se sugiere SOLO si: expectativa de vida ≥5 años + riesgo perioperatorio de ACV/muerte <1.5% (umbral actualizado post-CREST-2). Estenosis 50–69%: terapia médica intensiva sin intervención.
4️⃣ Marcadores de alto riesgo que individualizan la decisión: émbolos silentes en TCD, infarto silente ipsilateral en neuroimagen, hemorragia intraplaca en RM (HR 7.9), placa ecolucentе, área negra yuxtacanal >10mm² (stroke rate 5%/año).
5️⃣ La terapia médica intensiva es la base universal: estatinas (LDL <70mg/dL), antiagregación, control PA <130mmHg, cesación tabáquica y actividad física. Sin esto, ninguna revascularización optimiza su beneficio real.
🏥 Clínica Ricardo Palma — Centro Avanzado de Stroke | Lima, Perú
✍🏽 Dr. Manuel A. Moquillaza Valle | Neurólogo Vascular e Intervencionista | CMP 54060 / RNE 25595
#IctusIsquémico #EstenisisCarotídea #NeurologíaVascular #CREST2 #StrokePrevention
In high-risk atrial fibrillation with cerebral amyloid angiopathy, anticoagulation was associated with lower ischemic stroke and mortality without increased risk of intracranial hemorrhage or major bleeding.
By @HAlvinChenNeuro
https://t.co/3086cSBKIH
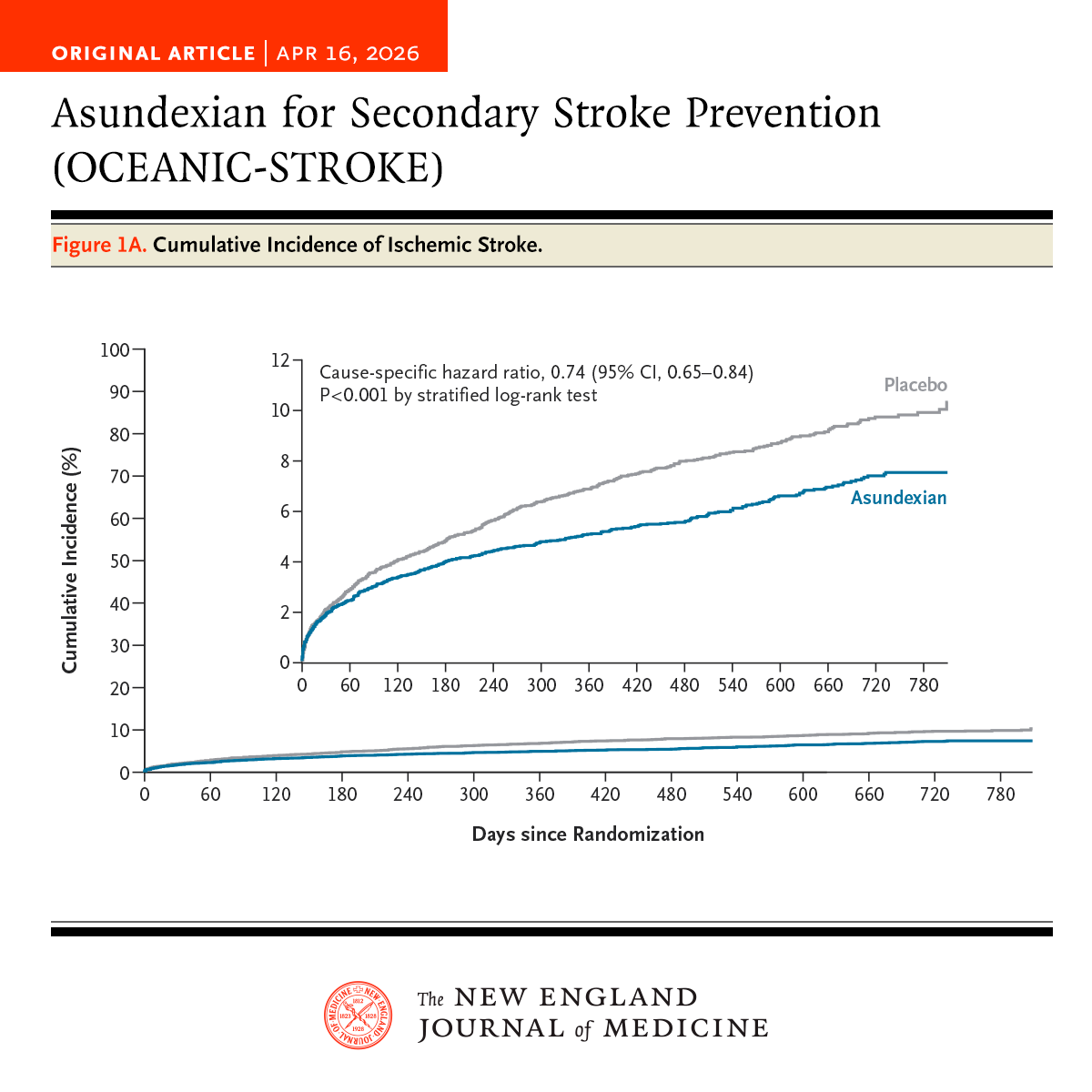
In the phase 3 OCEANIC-STROKE trial involving patients with noncardioembolic ischemic stroke or high-risk TIA, asundexian added to antiplatelet therapy led to a lower risk of ischemic stroke without increasing major bleeding. Full trial results: https://t.co/UPJGedYXFe
Editorial: Asundexian for Noncardioembolic Ischemic Stroke https://t.co/V1dVNbx4T8
More evidence to show that waiting for 7 days after stroke to stent a proximal carotid lesion is NOT necessary
"Delaying the ICAS according to current FDA recommendations may not be necessary when ICAS is indicated."
https://t.co/6i2Vutnn46
Useful information for neurointensivists and neurohospitalists.
When working up autoimmune CNS inflammatory syndromes, the Kappa Free Light Chain Index can distinguish MOGAD (very low to undetectable), NMOSD (moderately elevated), and MS (extremely elevated).
KFLCI is calculated as the ratio of CSF versus plasma levels, with elevated values indicating intrathecal B-cell mediated antobody sysnthesis, a key feature of MS.
https://t.co/tNgXxDKgnk
Don't miss "Comparative Effectiveness of Surgical, Endovascular, and Conservative Strategies for Unruptured Intracranial Aneurysms" in the newest issue of S:VIN.
https://t.co/kvp8eD1O0Y
Endovascular vs Medical Treatment of Basilar Artery Occlusion
@JAMANeuro
“At 3 years, the clinical benefit of EVT in patients with acute BAO was durable, with substantially better functional outcomes and reduced mortality compared with medical management.
These results reinforce EVT as the standard of care for BAO and support broader implementation and timely access to thrombectomy services.”
#curingcoma
https://t.co/DBqsi86MNr