When Insulin causing Hypokalemia is NOT the answer to the MCQ.
AIIMS/INICET Loves this
Everyone knows - Insulin pushes K+ inside the cell and causes Hypokalemia.
But there are two scenarios - where Hypokalemia is not the answer despite pathophysiology dictated by high insulin.
Both asked repeatedly in INI. Because examiner knows - you see Insulin, you pick K+.
A. Infant of diabetic Mother.
High RBS in mother - glucose goes inside fetus - caused fetal hyperinsulinemia.
This causes hypoglycemia in neonates born to diabetic mother - the most common metabolic abnormality.
However - the 2nd most common metabolic abnormality is HypoCalcemia - not HypoK+. This was asked in the exam I gave (May 2018). I picked K+
Don’t make the mistake like I did.
B. Refeeding syndrome.
A high calorie diet in first week to SAM results in sudden surge in insulin which causes K+ and PO4- to go inside cell.
HypoK+ and HypoPO4- occur.
But remember - the hallmark of Refeeding syndrome is Hypophosphatemia - not HypoK+
(why ? - because HypoK+ can occur due to SAM itself, hence not specific to Refeeding Syndrome - while hypophosphatemia only occurs when there is Refeeding syndrome)
Images from my offline class notes at DBMCI- will help.
Milestones
You can try to read revise and remember them 20 times and you’ll forget them 25 times.
But for gross motor milestones - a simple stick figure can help you figure out everything.
See the stick figure given below. Just remember - 3,6,9,12.
3 months - Neck control
6 months - Trunk control - Sit with Support
9 months - Knee Control - Stand with Support.
12 months - Feet control - walk with support.
A child would be able to stand with support only once it gains ability to sit without support.
So sit without support comes one month earlier - at 8 months.
Similarly- you’ll only be able to walk with support - once you’re able to stand independently.
Hence, stand independently comes at 11-12 months.
In Toto, this becomes
3 - NECK control
6 - Sit with support. (Trunk control)
8 months (9-1) month - Sit without support
9 - Stand with support (knee control)
11 months (12-1) - Stand independently
12 - Walk with support. (Feet control)
That’s it - you’ll now never forget Gross motor milestones for 1st year.
A lot of people preparing for NEET PG have issues remembering which disease is autosomal recessive, what is dominant.
While ofcourse - at the end of the day it is a little bit of rote memorisation - there is a certain logic to it.
Remember- enzymes- pretty much of all them in our body are more than what’s required.
So, even a 50% enzyme activity suffices for majority.
Hence, unless enzymes are fully zero - disease won’t manifest.
So, any enzyme deficiency- will be AR - both genes have to be mutated/absent.
PKU
Galactosemia
Glycogen storage disorders
Congenital adrenal hyperplasia
Alpha 1 anti trypsin
Wilson
Even 1/2 Hb causes mild anemia - so even That/Sickle cell are AR.
Contrast this with neuromuscular damage in general.
Anything that causes damage to nerves and Muscle- even 50% damage would result in disease.
If you look at AD diseases - most are have some issues either with nerves or muscles or cytoskeleton.
Huntington
Myotonic dystrophy
Achondroplasia
Marfan
Hypertrophic cardiomyopathy.
Most neurocutaneous syndromes. (tuberous sclerosis/neurofibromatosis)
Ofcourse this is not hard and fast.
But serves to improve your memory and understanding.
X linked is genuinely just rote memorization. Those genes just happened to be on X chromosome.
🧠 FOR RESIDENTS | HOUSE OFFICERS | CONSULTANTS
(STROKE LOCALIZATION MADE SIMPLE)
When a stroke patient arrives, don’t start with scans first.
👉 First question at bedside: Which vascular territory is involved?
This single step predicts the full neurological deficit.
1️⃣ Middle Cerebral Artery (MCA) Stroke
📍 Most common stroke territory
Contralateral face & arm weakness > leg
Contralateral sensory loss
Dominant hemisphere → Aphasia
Broca: non-fluent speech
Wernicke: fluent but meaningless speech
Non-dominant hemisphere → Hemispatial neglect
💡 Key clue: Face + arm > leg = MCA
2️⃣ Anterior Cerebral Artery (ACA) Stroke
Contralateral leg weakness > face/arm
Sensory loss (leg predominant)
Frontal lobe features:
Personality change
Urinary incontinence
💡 Key clue: Leg > face/arm = ACA
3️⃣ Posterior Cerebral Artery (PCA) Stroke
Contralateral homonymous hemianopia
No motor weakness
Memory impairment (hippocampus)
💡 Key clue: Isolated visual field defect = PCA
4️⃣ Basilar Artery Stroke
⚠️ Neurological emergency
Locked-in syndrome
Conscious but quadriplegic
Vertical eye movements preserved only
Bilateral motor deficits ± cranial nerve palsies
💡 Key clue: Locked-in = basilar until proven otherwise
5️⃣ Lacunar Strokes (Small vessel disease)
Seen in HTN & diabetes
Deep brain involvement:
Pure motor hemiparesis (internal capsule)
Pure sensory stroke (thalamus)
Ataxic hemiparesis (pons)
Dysarthria–clumsy hand syndrome
❗ No cortical signs:
No aphasia
No neglect
No visual field defects
💡 Key clue: Pure motor OR pure sensory = lacunar
🔑 ONE-LINE PATTERN RECOGNITION:
Face/arm > leg → MCA
Leg > face/arm → ACA
Visual field cut only → PCA
Locked-in → Basilar
Pure motor/sensory → Lacunar
🧠 If you can localize, you can diagnose before imaging.
🧵 “Doctor, why is my BP still 190/110 despite 4 medicines?”
Because sometimes hypertension is NOT the disease.
It’s the symptom.
Clinical cases that reveal the hidden causes of SECONDARY HYPERTENSION 👇
The night shift was quiet until my intern yelled...
"Sir, the COPD patient in Bed 2 came in gasping with an O2 saturation of 82%! I fixed it, but now he won't wake up!"
The Catch:
The intern had put him on a 15-Liter Non-Rebreather mask.
The monitor now showed an SpO2 of 100%, but the patient was unarousable, breathing shallowly and bounding pulses.
The intern was confused: "His saturation is perfect now! Why is his GCS dropping?"
A classic ward tragedy.
Med-X, what did the intern just do, and how do we fix it?
🚨 Cardio pearls you should never miss 6️⃣
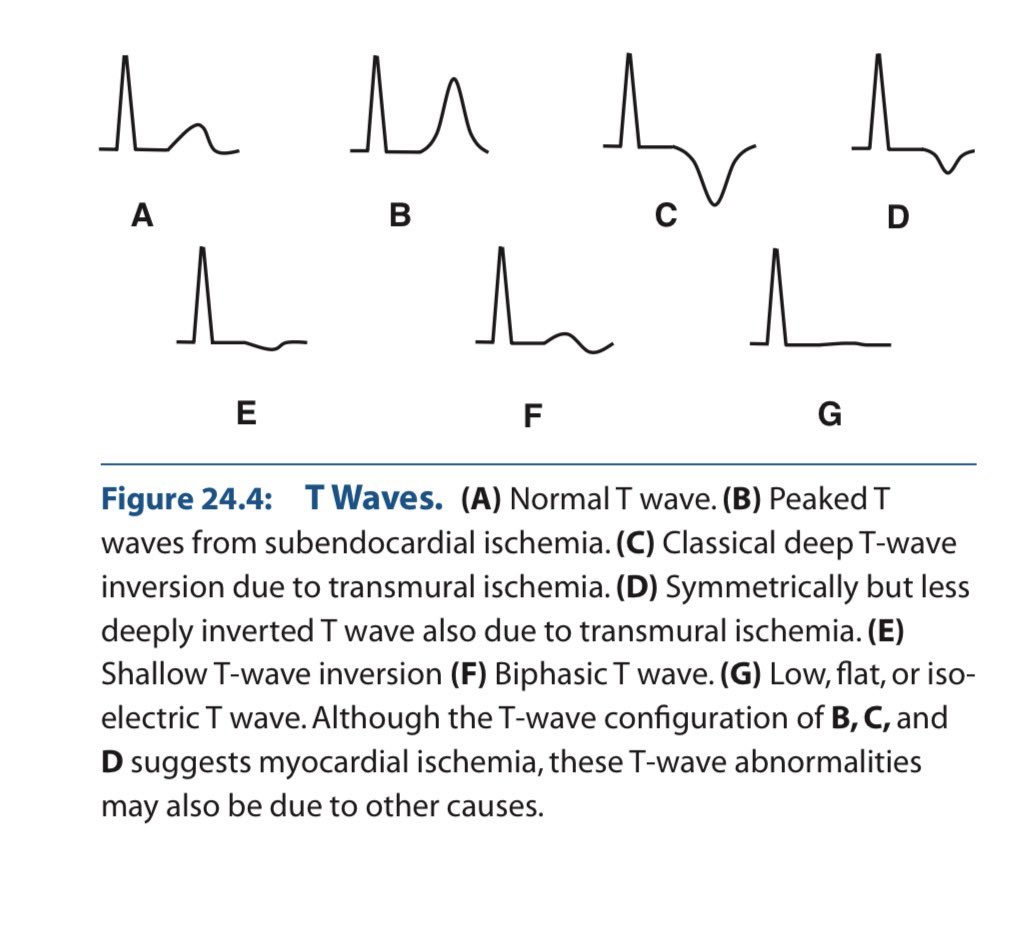
The T wave in the ECG is a story about repolarisation not a random squiggle.
When it inverts, something changed in the direction or timing of ventricular recovery.
Let’s clear the confusion once for all & understand in depth.
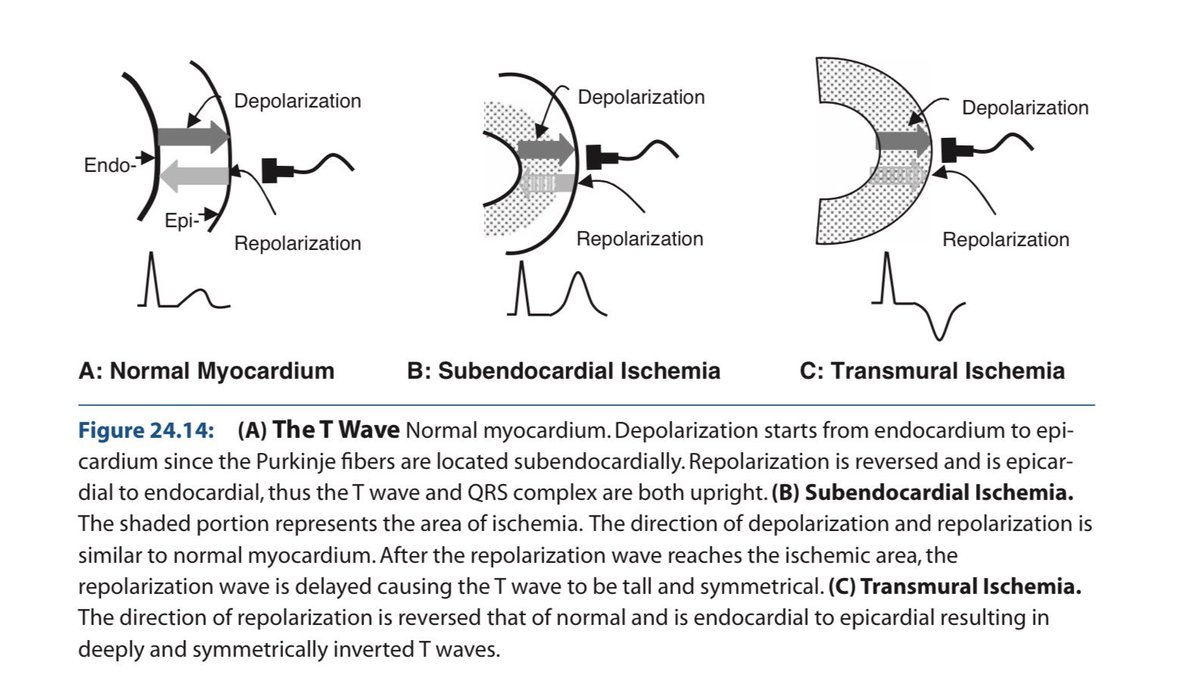
1️⃣ Why is the normal T wave upright?
✔ Purkinje fibers are subendocardial in location.
So:
Depolarization → Endocardium → Epicardium
Repolarization → Epicardium → Endocardium
Epicardial cells:
🔻Shorter action potential duration
🔻Larger transient outward K⁺ current (Ito)
🔻Faster phase 3 repolarization
Repolarization is a negative wave moving opposite depolarization → vector aligns with QRS.
👉 Upright T wave.
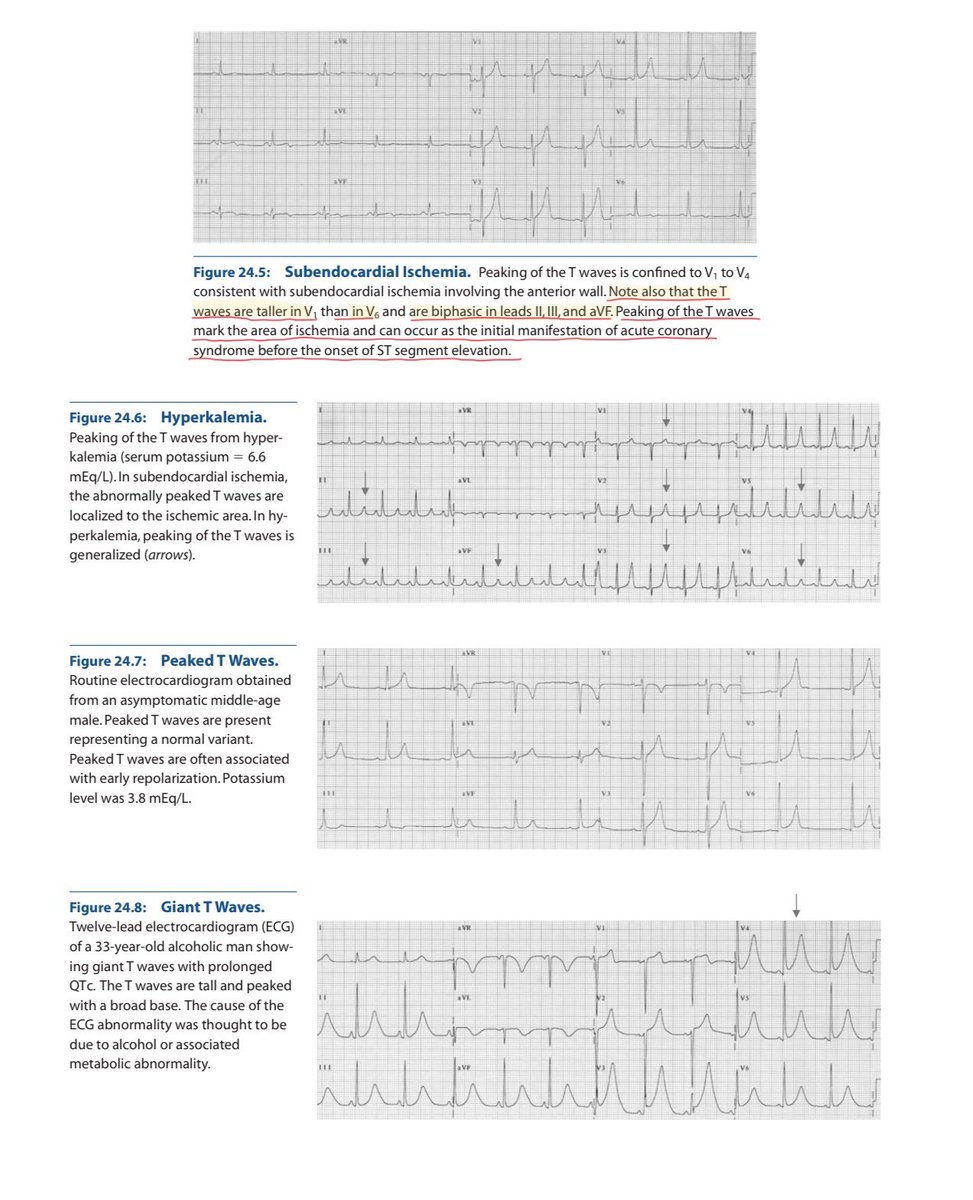
2️⃣ Subendocardial ischemia (early)
Inner myocardium + Purkinje network suffer first.
Ischemia causes:
🔻ATP depletion
🔻KATP channel opening
🔻Extracellular K⁺ accumulation
🔻Shortened action potential in ischemic zone
🔻Slowed Purkinje conduction
ECG:
→ Tall, symmetric, broad-based T waves
(Hyperacute phase)
3️⃣ Transmural ischemia
Repolarization sequence reverses abnormally.
Vector flips.
→ Deep, symmetric T-wave inversion
Seen in:
🔻Evolving MI
🔻Wellens pattern
🔻Reperfusion
Deep + symmetric + territorial + dynamic = ischemia until proven otherwise.
4️⃣ Hyperkalemia
Global extracellular K⁺ elevation.
ECG:
🔻Narrow, tented T waves
🔻Short QT
Sharp, narrow spikes ≠ broad ischemic T waves.
5️⃣ Hypokalemia
Delayed repolarization.
ECG:
🔻Flat T waves
🔻ST depression
🔻Prominent U waves
U waves help differentiate from ischemia.
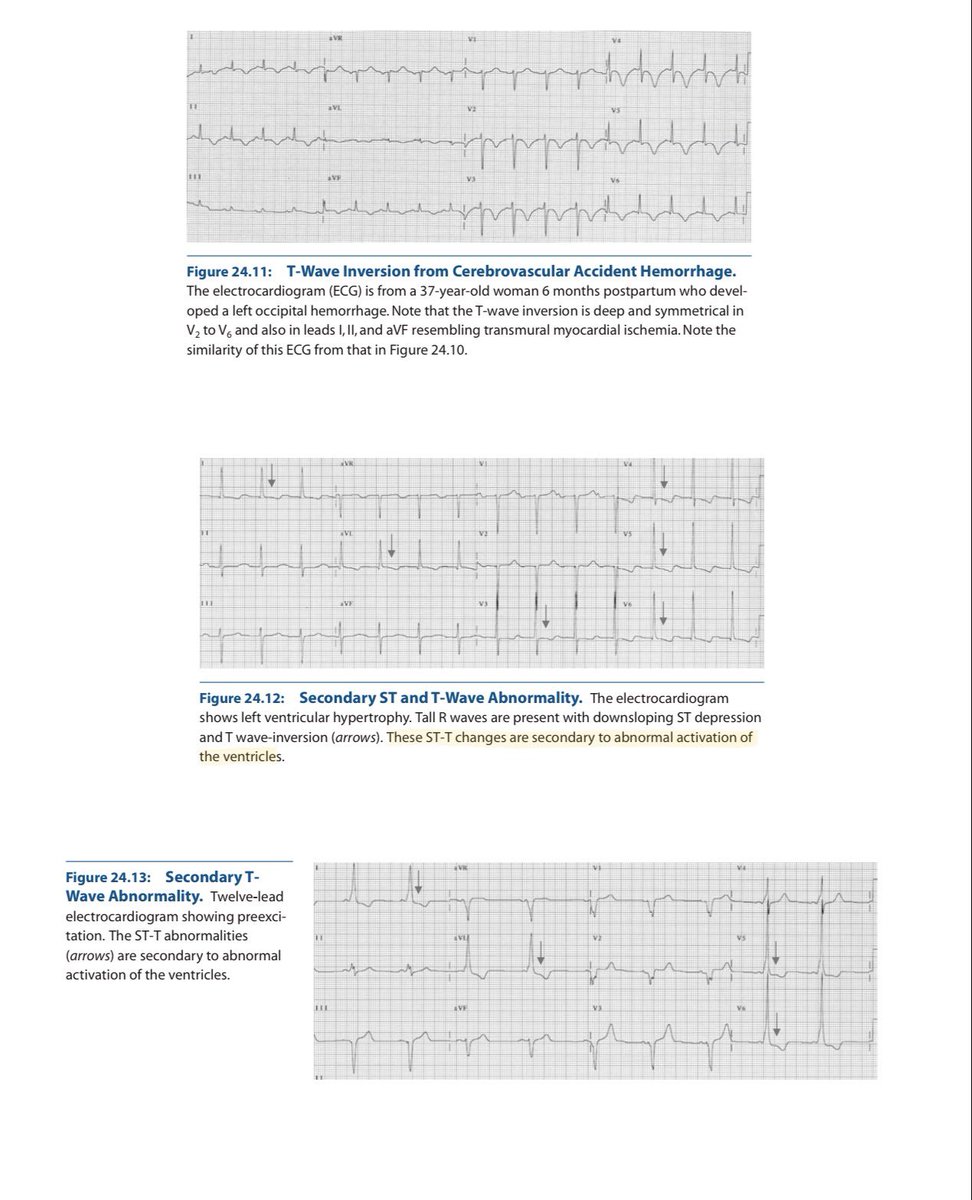
6️⃣ CNS / Neurogenic T waves
Catecholamine surge → myocardial stunning.
ECG:
🔻Deep, diffuse T inversions
🔻QT prolongation
🔻Not vascular territory specific
Distribution matters.
7️⃣ LVH & Strain Pattern
This is not primary ischemia.
It’s repolarization abnormality secondary to abnormal depolarization.
In LVH:
🔻Increased myocardial mass
🔻Prolonged depolarization
🔻Delayed repolarization in hypertrophied wall
ECG:
✔ High-voltage QRS
✔ Downsloping ST depression
✔ Asymmetric T-wave inversion
(Usually lateral leads: I, aVL, V5–V6)
Key point:
Strain T waves are asymmetric, gradual downstroke + rapid return.
Ischemic T waves are symmetric.
8️⃣ Cardiomyopathies
Hypertrophic cardiomyopathy (HCM)
🔻Deep T inversions (often in precordial leads)
🔻May mimic ischemia
🔻Often associated with large voltages
Apical HCM
🔻Giant negative T waves in precordial leads
Dilated cardiomyopathy
🔻Nonspecific ST-T changes
🔻Often diffuse
Mechanism:
Structural remodeling alters repolarization gradients.
Not vascular. Not dynamic like ACS.
9️⃣ Final Differentiation Framework
✔ Symmetric + territorial + dynamic → Ischemia
✔ Narrow tented + short QT → Hyperkalemia
✔ Flat T + U waves → Hypokalemia
✔ Diffuse deep T + long QT + neuro event → CNS
✔ High voltage + asymmetric lateral T inversion → LVH strain
✔ Giant precordial inversions + echo changes → HCM
✔ Stable V1–V3 inversion in young → Benign variant
T waves reflect:
• Repolarization timing
• Potassium currents
• Myocardial thickness
• Conduction sequence
• Autonomic tone
If you understand vectors + ionic physiology, the ECG becomes logical.
Electrophysiology > memorized patterns.
(Ref: Marriott’s Practical Electrocardiography; Surawicz & Knilans)
#MedTwitter #MedX #ECG #Cardiology
In Canadian medical training, we had oral exams with high-pressure “short cases.”
Mine:
Two examiners at the bedside. Silence.
“Dr. Aird, please examine this patient for an MCV of 140.”
How would you approach this?
A thread on Snake Bite management, focusing on approach in the ER and ICU in a tertiary care center
Topics:
History and examination in ER
Assessment in ICU
Investigations
ASV
Specific Bite management
Recovery
Surgical Procedures
Shifting Out
Long-term complications
My fav med twitter interaction tweet is someone saying TB can cause everything except pregnancy and someone in the comments mentioning OCP failure by rifampicin can lead to pregnancy and hence, TB in fact can cause everything