I count 12 abstracts on GLP1s for cancer prevention at ASCO
All of them are observational, and it's clear a proper randomized trial is needed here – two things on that
1. Lilly and Novo are not currently interested in doing it (thanks to @theglpman for helping to figure this out)
2. The first randomized trial is planned (called INSPIRE, from the ECOG-ACRIN research group) – for primary and secondary prevention of breast cancer in 11,000 overweight (non-obese) women, with a 5 year follow-up
🆕 Results from the POSITIVE trial with longer term follow-up are now out in @Annals_Oncology
Temporary interruption of endocrine therapy to attempt pregnancy is safe and does not increase the risk of #breastcancer events @AnnPartridgeMD
https://t.co/vyBN0TtPyM
🆕 article in press: Final outcomes of the SOFT and TEXT phase III trials in premenopausal hormone receptor-positive early breast cancer @DrHBurstein@LoiSher
https://t.co/cpHhlv21vo
Dijo una vez Rafael Nadal en su documental Rafael Nadal: Behind the Racket (2024): “La gente ve los trofeos, las victorias y los títulos… pero no ve que casi toda mi carrera he jugado con dolor. He pasado más tiempo lesionado que sano. Hubo temporadas en las que pensaba que no podría volver a competir. Pero seguí adelante. No porque sea un héroe, sino porque el tenis es mi vida y aprendí a convivir con el dolor.”
En el documental, Nadal habla con una crudeza y realismo poco habitual en él: revela que ha jugado finales de Grand Slam con fracturas por estrés, con el pie destrozado, con el brazo inflamado y bajo fuertes infiltraciones. Admite que en varios momentos de su carrera pensó seriamente en retirarse, pero que su mentalidad y su amor por el juego lo mantuvieron en pie.
Esta reflexión muestra la otra cara de la leyenda: detrás del “Rey de la Tierra” hay un atleta que ha competido durante casi dos décadas con el cuerpo roto, convirtiendo el dolor crónico en parte de su rutina diaria.
Una lección brutal de resiliencia: el verdadero campeón no es el que nunca cae, sino el que aprende a jugar y ganar mientras duele.
Feliz cumpleaños, Rafa. Tu ejemplo va mucho más allá del tenis.
A new study links GLP-1 drugs and 30-35% reduced incidence of breast cancer, using matched-pair propensity analysis
https://t.co/AjNYlDM3A3
Confirms other association studies but still no proof
SOFT/TEXT 15-year final results: tamoxifen remains reasonable for low-risk premenopausal HR+ disease; in young, HER2−, high-risk patients, OFS—and especially exemestane+OFS—provides a stronger endocrine backbone.
https://t.co/Ki645zigZz
📢 Gianni Bonadonna Fellowship open to applications❗️
Would you like to become a physician scientist?
This is the opportunity you were looking for.
We need passionate and motivated physician scientists for accelerating breakthrough innovation and therapies by cancer research
ASCO 2026 in breast cancer was not about “more treatment.”
It was about smarter treatment.
TROP2 ADCs are expanding options in TNBC.
ctDNA is shaping endocrine strategy.
Chemo can be safely omitted in selected early HR+ disease.
Supportive care and de-escalation are finally getting the attention they deserve.
This is what meaningful progress looks like.
#ASCO2026 #BreastCancer #Oncology @JCOGO_ASCO@ASCO@JCO_ASCO@DFCI_BreastOnc@OncoDailyBreast@oncodaily@OncoAlert@ConquerCancerFd@BCRFcure@KolPulseAI
Iza-Bren (EGFR-HER3 ADC) vs investigator choice of chemotherapy in pretreated mTNBC, most had received 1st line tx, less second line, did include prior taxane, mPFS 8.5 mo vs 3.1 with TPC, HR 0.29, OS 15.9 mo vs 12.5 mo with TPC, HR 0.60, most frequent high grade TRAE were hematologic, in the age of ADC use in the first line mTNBC, subsequent studies evaluating this agent in earlier settings will be important to see! @OncoAlert
OPTIMA: Genetic Test–Determined Chemo Is Noninferior to Chemo + Endocrine Therapy in Selected Patients With Early Breast Cancer https://t.co/gb5YNRwke4 @ASCOPost Someone should correct this headline: 1. ET (not Chemo) is noninferior 2. It's a Genomic test (did AI write this?)
Landmark Advance:
ASCENT-04 Redefines First Line Therapy in PD-L1+ mTNBC with Sacituzumab Govitecan + Pembrolizumab
@OncoAlert#ASCO26#BreastCancer#bcsm
#ASCO26 Practice-Changing:
The ASCENT-03 Trial, presented by @stolaney1 establishes Sacituzumab Govitecan as the new first line standard of care for PD-(L)1-ineligible metastatic TNBC, delivering superior and durable disease control beyond chemotherapy.
@OncoAlert#bcsm
One of my favorite abstracts of this #ASCO26 - reduced denosumab dose intensity (q12w) is NON inferior to q4w in pts with mBC or mCRPC, with improved safety profile in terms of risk of hypocalcemia and osteonecrosis of the jaw
Practice changing!!
@OncoAlert
🧬 ASCENT-03 Biomarker Analysis Presented At ASCO 2026
A preplanned exploratory analysis of ASCENT-03, presented by Carlos H. Barrios, MD, evaluated sacituzumab govitecan versus chemotherapy across biomarker-defined subgroups in previously untreated advanced triple-negative breast cancer patients who were not candidates for PD-(L)1 inhibitors.
Median PFS was longer with sacituzumab govitecan across Trop-2 expression quartiles, tumor BRCA wild-type and mutant subgroups, and HER2 IHC 0 and HER2-low subgroups.
The findings reinforce the clinically meaningful benefit of sacituzumab govitecan as a first-line treatment option in this advanced TNBC population, while supporting its activity across multiple biomarker categories.
https://t.co/9BoejxTH9u
@stolaney1@JavierCortesMD@kevinpunie@breastoncdoc@MOliveira_MD@dradityabardia
#ASCENT03 #TNBC
#ASCO26 🚨 ASCENT-03 reinforces the case for frontline sacituzumab govitecan in PD-L1–ineligible mTNBC.
Despite heavy crossover (82% of chemo arm later received SG), SG still improved PFS2:
🔹 PFS2: 18.2 vs 14.0 mo
���� HR 0.70
🔹 30% lower risk of progression after next-line therapy
Patients receiving upfront SG also had:
⏳ Longer TFST: 11.2 vs 7.9 mo
⏳ Longer TSST: 17.3 vs 16.6 mo
Key message:
Using SG earlier may provide more durable disease control rather than “saving it for later.”
@OncoAlert @myesmo @asco @esmo_open @GileadSciences
#BreastCancer #TNBC #OncoTwitter
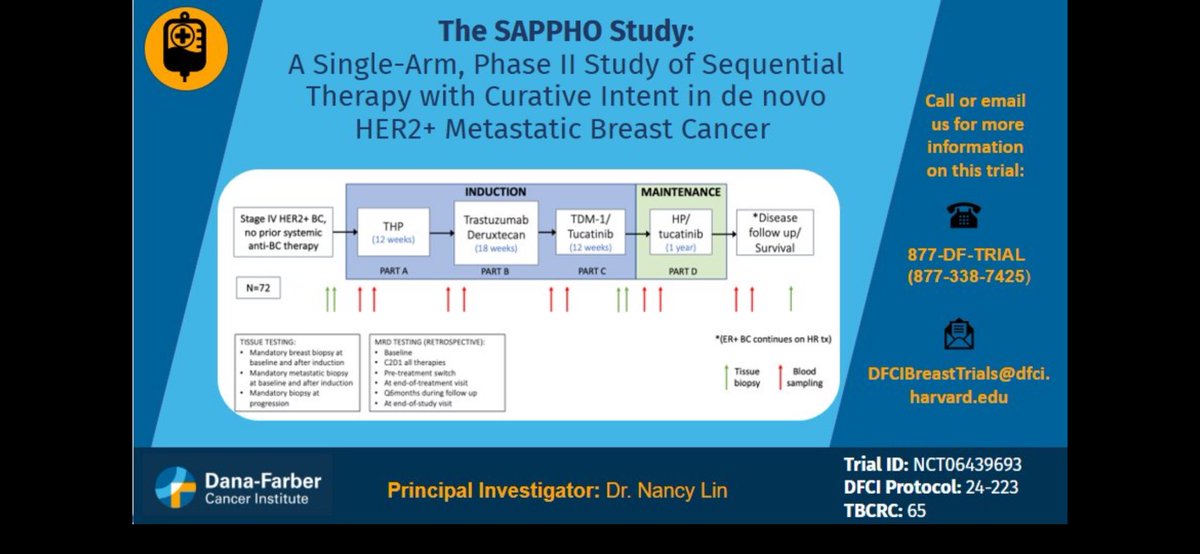
📣 @thetbcrc 065 SAPPHO Study 📣
🔹Open & enrolling!
💭Does sequential intensive tx in HER2+ de novo MBC increase the probability of being disease free at 4 years?
🔹 THP or TDXd➡️THP or TDXd➡️TDM1 +tucatinib ➡️HP/tucatinib ➡️
🔹If progression free ➡️stop HER2 tx (continue ET)
📌persevERA BC📌
♦️1L HR+ MBC, recurrence >12 months from ET stop➡️ giredestrant + palbo vs letrozole + palbo
♦️PFS 33.1 m vs 28.2 m HR 0.89 (p=0.1553) not significant
♦️ORR, CBR similar, DoR 38.5 m vs 30.4 m
♦️OS immature