One key issue is that <1% of the ADC actually distributes to the tumor
Target expression attempts to predict the benefit from that 1%
Innovative biomarkers are needed to predict benefit from the remaining 99% that distributes across the rest of the body
PANKU-Breast02, Phase 3 trial at #ASCO26: iza-bren (vs chemo) becomes the first bispecific ADC (EGFR×HER3) to hit dual PFS + OS in pretreated metastatic TNBC.
📊 PFS 8.5 vs 3.1 mo (HR 0.29)
📊 OS 15.9 vs 12.5 mo (HR 0.60)
KOL voices + the actual slides 👇
https://t.co/EZRypnZA21
Discussion Leaders: @MamMa_mimumemo, @PTarantinoMD,@kazuki_nozawa, @Dr_Oncologista
2 days.
That’s how quickly the “FDA in chaos“ turned around this expanded access application for a novel therapy for a life threatening disease.
Because the bar for the FDA should be: does strong data support it… not sham trial negative but here’s a historical control arm and desperate patients would take it.
Tec beat a weak control arm, at a real toxicity cost. About 15% weren't truly CD38 refractory but still did not receive additional Dara. The OS signal is likely real but inflated by weak control arm. We should have learned this lesson from CARTITUDE-4. Hopefully future trials will have more rigorous controls reflecting the SOC.
This is a very interesting finding in PROTEUS. pN1 rates similar in both arms, so adding ARPI did not eradicate much extra small-volume metastatic disease. Not very encouraging for ARPI in intact prostate RT. But perhaps another important scientific contribution from this trial.
@PTarantinoMD Great results, but I am always concerned when the comparator is so heterogenous. I think they would be more reliable if all patient in control arm were treated with a drug for which we have more solid and robust data in second line, like capecitabin or eribulin.
One lung cancer.
Different EGFR mutations. Different first choices.
The new ASCO update reminds us: precision begins before treatment starts.
Are we testing early enough? @ASCO@OncoAlert@OpenMedicineHQ
What The Devil Wears Prada 2 Taught Me About Oncology ??
Warning: Mild spoilers.
I know this slide became famous at ASCO 2026, beautifully used by Dr. Brahmer during the HARMONi-6 discussion.
But this post is not about that trial.
I recently watched The Devil Wears Prada 2 in a Mumbai theatre and loved it. Fantastic acting by Meryl Streep @MerylStreepPage , sharp writing, and plenty of witty punch lines. Highly recommend to watch, especially if u have watched first part .
While watching it, I couldn't help thinking about how many of its themes apply to medicine, academia, and oncology.
My 5 cents 🙂👇
1- if you are at the top of the ladder, try to be kind to those below it. It helps them, but eventually it may help you too. One of the striking moments in the movie is that when Miranda's world begins to unravel, Andy is still willing to help her despite everything that happened between them in the first film. Careers are long. Today's junior colleague may become tomorrow's collaborator, supporter, or even savior. Kindness is not merely generosity; it is also good judgment.
2- Be honest and truthful to yourself as far as possible. Throughout the movie, Andy struggles with the tension between ambition and authenticity. She never completely abandons her own values, even when doing so might have made life easier. In the end, she still finds her own path. Medicine constantly tempts us with more titles, more visibility, and more recognition. Ambition is important, but it should not come at the cost of losing sight of who we are.
3- Appreciate your team members in public. Loyalty should count. One of the most satisfying moments in the film is when Miranda finally recognizes Nigel's contribution and publicly entrusts him with a major responsibility. Could it have happened earlier? Certainly. But she eventually corrects her mistake. Every department has a Nigel—the colleague who quietly keeps things running, solves problems, and asks for little in return. Recognition delayed may not be ideal, but it is still far better than recognition denied.
4 - Never burn bridges with your rivals. If possible, become pals. By the end of the movie, Andy and Emily develop genuine respect for each other despite Emily's efforts to undermine Andy while trying to take control of the company. Professional rivalries are inevitable. Lifelong grudges are not. Today's competitor may become tomorrow's collaborator. The bridge you burn today may be the one you need to cross later.
5-
Finally—and perhaps most importantly—no matter how high you climb, one day the climb ends. Miranda is forced to confront a future without the position that defined her for years. In that moment, power, influence, titles, and status suddenly seem far less important. What remains is family. The husband she often neglected is the one who stands beside her, gives her hope, and reminds her that there is life beyond a career. The cost of reaching the top is real, but so is the cost of forgetting those who matter most while getting there.
In oncology, we spend years climbing. We chase publications, podiums, leadership positions, awards, committee memberships, and recognition from our peers. There is nothing wrong with ambition. In fact, many of the advances our patients benefit from today exist because ambitious people refused to settle for the status quo.
But every ladder eventually has a final rung.
The question is not whether we reach the top. The question is what remains when the climb is over. Will we be remembered only for the titles we held, or also for the people we helped, the colleagues we supported, and the relationships we nurtured along the way?
Oncology, fashion, business, politics—the setting changes.
Human nature doesn't. @allisonoconn@Alfdoc2@ErikaHamilton9@drsarahsam@brunolarvol@OncBrothers@KolPulseAI@MedwatchKate@stolaney1@PTarantinoMD@dr_yakupergun@NiuSanford
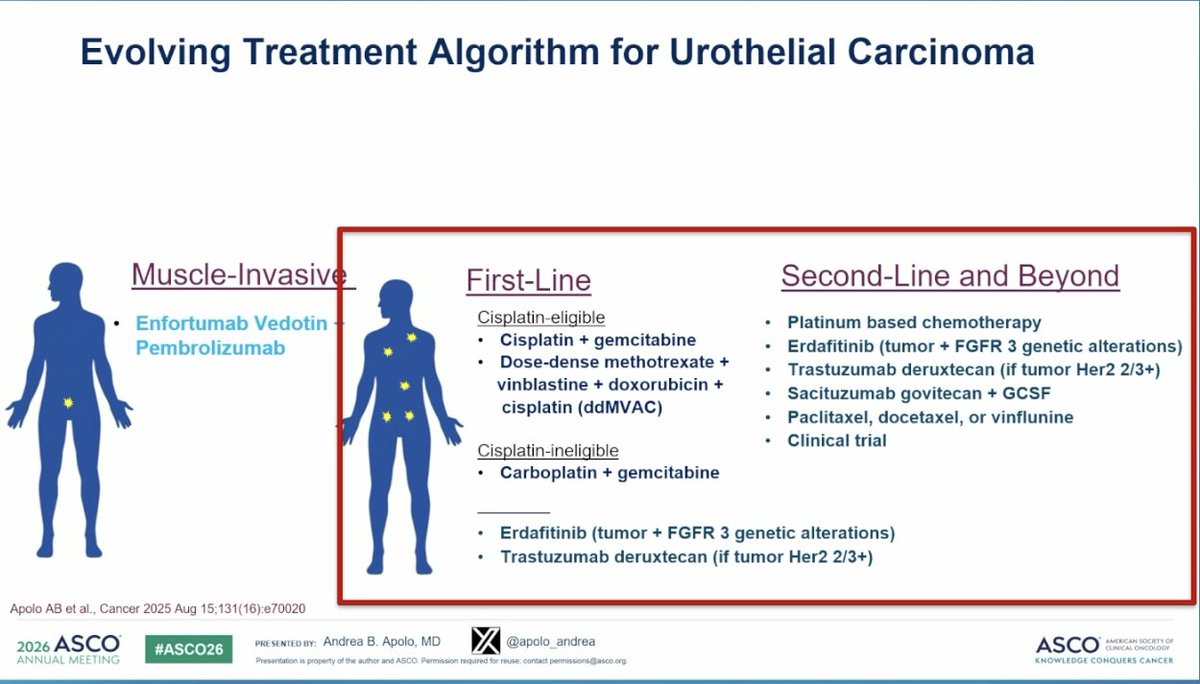
Thoughtful discussion by @apolo_andrea on Nectin-4 biology in urothelial cancer.
She reminds us that breast cancer physicians have already taught us that T-DXd works after T-DM1 failure: same HER2 target, different payload (DESTINY-Breast02: PFS 17.8 vs 6.9 months, HR 0.36). The antibody isn't doing all the work.
LY4052031 is testing the same logic in urothelial. Topo-I payload, same Nectin-4 target as EV.
SHR-A2102, another Nectin-4 Topo-I ADC, in MIBC.
The sequencing question from early stage to refractory metastatic disease may be focused on the payload.
#BladderCancer #UrothelialCA #ASCO26 #GUonc
Both ASCENT-04 and ASCENT-03 efficacy is lbiomarker independent. Is this surprising? Not really. We have seen a similar pattern across the DESTINY-Breast studies, where no biomarker has been statistically meaningful enough to clearly define who benefits.
This may be a fundamental feature of ADC biology. ADCs are not classic targeted therapies in the narrow sense. They use the antibody to deliver a potent payload, and once enough drug reaches the tumor, the payload can effectively annihilate cancer cells. That is why expression level, BRCA mutation status, or HER2-low versus HER2-ultralow may not always behave as clean predictive biomarkers. #ASCO26
HER2CLIMB05 - how do we incorporate maintenance tucatinib in the setting of DestinyBreast-09 1L with TDXd + pertuzumab or PATINA data for triple positive BC. Lot of options for pts but lack of clarity on optimal 1L and 2L Rx. #SABCS25@ErikaHamilton9
Celcuity’s gedatolisib doubled progression-free survival versus standard of care in certain patients with advanced breast cancer. Still, the biotech’s stock dropped more than 25% Tuesday.
https://t.co/mRzTH7dE2B
Was great to chat with @l_ballas, who had many interesting questions beyond what we had time for @APCCC_Lugano. Loved the meeting. Loved the interview discussion @urotoday. Love working with smart people to make care better for our patients!
#APCCC26
#ASCO26: PROTEUS phase 3 reports final data on perioperative apalutamide + ADT before radical prostatectomy in high-risk #ProstateCancer.
Worth read the translational CALGB 90203 analysis after neoadjuvant chemo hormonal therapy in @JNCI_Now
🔗: https://t.co/wE0z4VKGbr
Final 15-year SOFT/TEXT results confirm that ovarian function suppression matters in premenopausal HR+/HER2− early breast cancer.
•Tamoxifen + OFS reduces recurrence vs tamoxifen alone
•Exemestane + OFS further lowers recurrence and distant relapse risk
•Greatest benefit seen in very young women (<35 years) and other high-risk patients
A powerful reminder that treatment escalation should be considered for those at highest risk.
#BreastCancer @OncoAlert@oncodaily@Larvol