@VincentRK How do you know that AI wasn't used. Agree on the excellent accomplishments of humans, but AI has been around for a long time, and I would bet the house it was used at every conceivable level in small or large part. This isn't a knock on human ingenuity, its flag in it's cap.
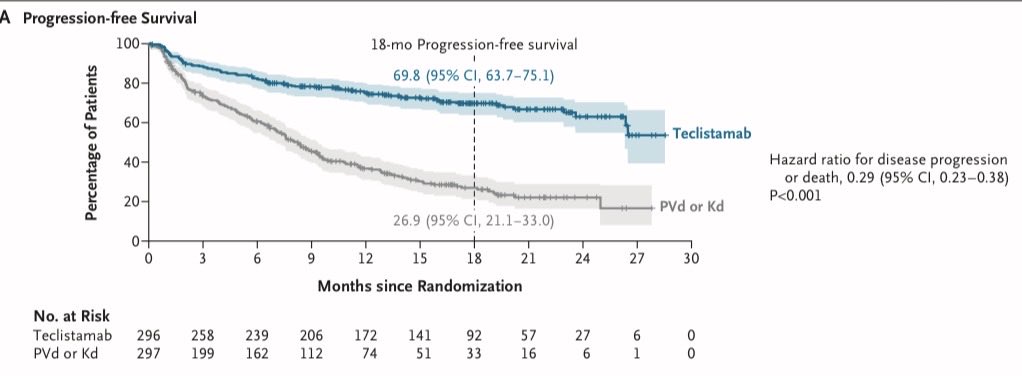
MajesTEC-9 is now out in @NEJM! 18-month PFS ~70% and DoR~80% with Tec! Infection risk mostly front-loaded (1st 6 months) but doesn't plateau [G3+ infections remains at ~10% in each time window beyond 12 months]. The slope of PFS curve in Tec arms progressively flattens with time➡️will there be a plateau with long-term follow-up?
#ASCO26
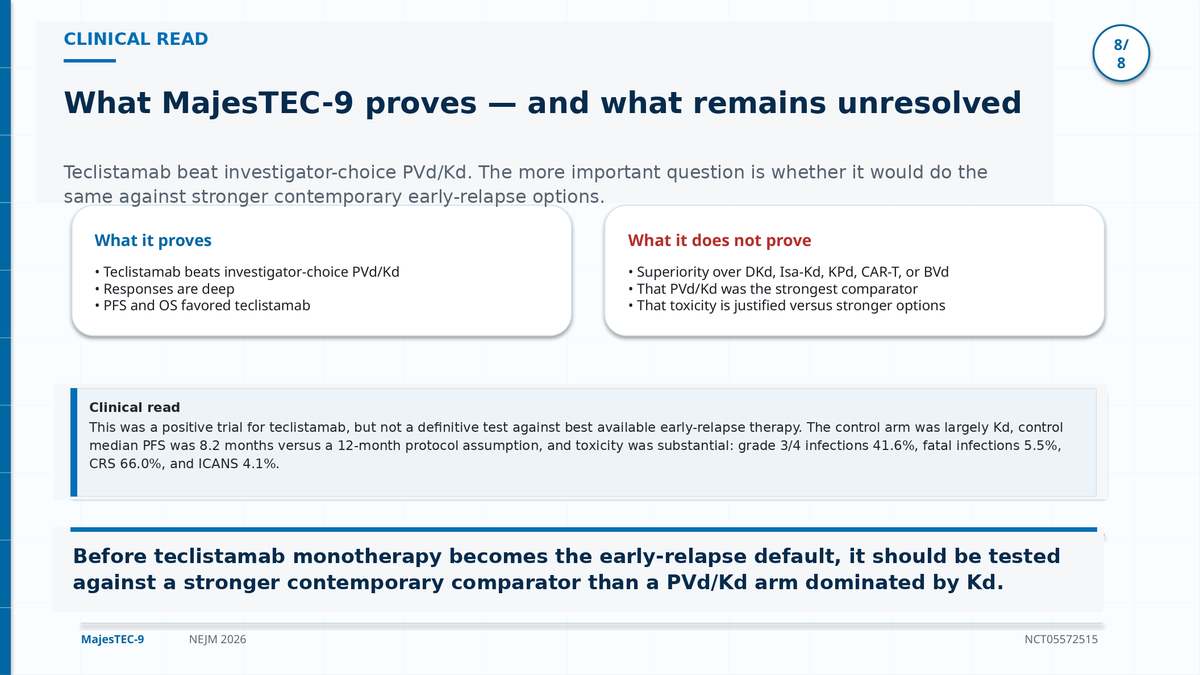
The comparator was weak, unclear of real benefit against a better control. The toxicity may be front loaded but it is very significant. This trial at face value is tantalizing, but under the hood it becomes much more problematic to conclude it as a "new standard" although many will.
Concomitant publication in @NEJM#ASCO26
BCMA bispecific moves earlier in myeloma.
MajesTEC-9 | NEJM 2026
Teclistamab monotherapy vs PVd/Kd in RRMM after 1-3 prior lines, all exposed to anti-CD38 + lenalidomide.
🧬 18-mo PFS
69.8% vs 26.9%
HR 0.29
🫀 18-mo OS
79.2% vs 68.6%
HR 0.60
🎯 CR or better
65.9% vs 16.8%
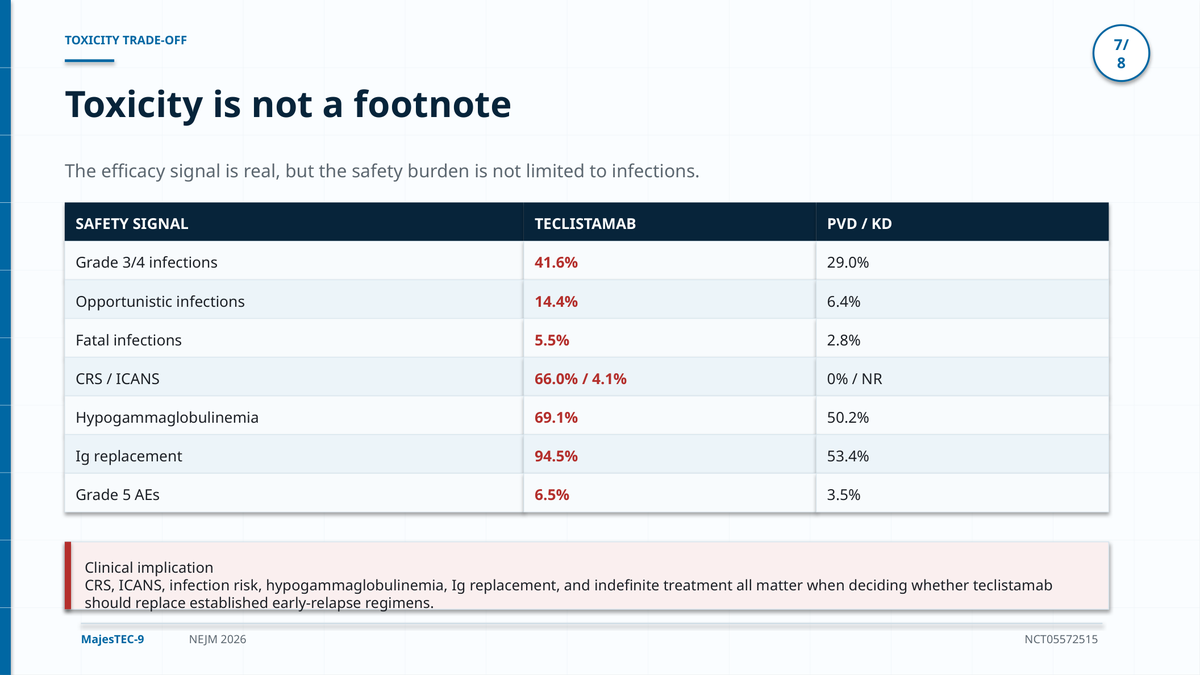
But the price is real:
Grade 3/4 infections 41.6%
CRS 66%, mostly grade 1-2
ICANS 4.1%
Takeaway:
Teclistamab is no longer just a late-line rescue story.
Early BCMA targeting is becoming a serious relapse strategy - but infection prevention is not optional.
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #MultipleMyeloma #Myeloma @OncoAlert@myesmo@esmo_open
@Dr_RShatsky@allisonoconn@PTarantinoMD I would argue that at the very least it should be done within the first 3 months. I have found ways to make this a relatively easy reality in conjunction with pulmonology and well defined pathways in our office.
@allisonoconn The most severe cases occur early, my practice is to strictly check CT scans in addition to pfts frequently in the first 3 months, sometimes more often than the trials as this was just an arbitrary trial recommendation that is not evidence-based.
@jeremyeorr@PTarantinoMD@Dr_RShatsky@allisonoconn High resolution CT has a higher sensitivity that is significant over pfts, both should be done but pfts should not replace a CT. Decreasing dlco is the earliest sign but it's also nonspecific.
The future of hematology may no longer be “disease control.”
It may become relapse extinction.
Old paradigm:
Treat → remission → relapse → treat again
This cycle can improve:
• PFS
• response rates
• MRD negativity
…but may not truly change destiny.
Emerging paradigm:
Early deep immune intervention before:
• T-cell exhaustion
• clonal complexity
• immune escape
• resistant biology
The future may depend on:
• earlier CAR-T
• rational combinations
• MRD-adapted therapy
• immune fitness
• elimination of relapse-capable clones
The real question is no longer:
“Can we prolong remission?”
The real question is:
“Can we eliminate the relapse-capable clone?”
PFS improvement is progress.
OS improvement is the purpose.
Cure is the destiny.
#MultipleMyeloma #AML #lymphoma #CART #BMT #Hemetwitter
Dr. Fun + G
Sunday Hematology Thoughts ☕️🩸
2005:
“Why are the transplant physicians giving IVIG to everyone after MUD transplant?! No randomized OS benefit! Too expensive!”
2026:
“If your bispecific patient has IgG 397 and sneezed twice without IVIG… is that ethical?” 😱
IVIG really said:
“Y’all MISSED me?” 🎤
The funniest part of medicine is watching supportive care therapies disappear for 15 years and then return like a Marvel character with a new costume.
To be fair… BCMA bispecifics changed the game:
• prolonged plasma cell aplasia
• chronic hypogammaglobulinemia
• real infection mortality
But somewhere between “never IVIG” and “monthly IVIG forever after one rhinovirus” lies… science 😂
The Circle of Life continues.
#MultipleMyeloma #Lymphoma #Hemetwitter
@Papa_Heme My last MCL ASCT was probably 2 years ago now, with good induction most get to negative MRD (we know ASCT is useless there), and those who are MRD positive (mostly biologically high risk) I don’t know if ASCT will help much (vs BTK/BCL2 inh at relapse +/- CAR)
It has been a tremendous resource however whether this resource continues to exist depends heavily on how it embraces AI which can already instantly do things better with even more voices that matter.
Here is the inside story on how @UpToDate does what it does.
From my experience as an author/section editor for UpToDate for 20 years, here is how it works. It’s amazing!
Every day a team of people @UpToDate scour the top medical journals (and major meeting abstracts) for articles of importance. In my case they pertain to myeloma and related disorders. Any article that is felt to be important is sent to a expert MD medical editor at UpToDate who reviews the paper. If the information is felt to be important, the relevant chapter is updated with this content, summarized in a few sentences in Word track and then sent to the author of the chapter who is a top expert in the field.
As an author I have to review the update in detail and then make a decision whether to include the new information, and whether the way it has been incorporated is correct or needs to be edited.
Once I make a decision, it is then reviewed by an expert section editor. For 15 years for me, the section editor was Dr. Robert Kyle! (Currently I’m the section editor and we have about 6 experts serve as authors on over 40 chapters pertaining to myeloma and related disorders). The section editor independently decides whether the author made the right call and either approves or we have a back and forth till we agree.
The updated chapter is then reviewed again by the expert MD editor at UpToDate and then posted.
For important phase III trials or FDA approvals we usually make the update within a week. Sometimes by the next day! With so many important papers, every week there are 2-3 updates pertaining to my chapters that go through the above process! It’s hard work but it keeps me ridiculously current. And more importantly it keeps the content accurate and current. This is not random addition of new information. It’s vetted information that’s added.
Every UpToDate chapter is also peer reviewed annually. Each chapter also undergoes an annual author and editor review to make sure that the overall content and flow is good and to delete content that may be no longer important or accurate. The extraordinary process and rigor involved is why it’s such an invaluable irreplaceable resource. It is AMAZING and hard to replicate.
UpToDate is easy to navigate. But the newly launched UpToDate Expert AI takes it to the next level! It makes the entire content available to query just like you query a top ranked LLM. But it’s not searching the random internet or a stack of published articles. It’s primarily trained and derives vetted and adjudicated UpToDate content. It will not randomly hallucinate. It will not list 10 options for treatment newly diagnosed myeloma but will give you what experts currently feel is the best option based on the latest evidence. All answers are referenced and pointing to specific content sections in UpToDate (which also has links to source material). So you can immediately get all the background information if you need more detail.
Working with UpToDate has helped my career immensely. For the last 20 years it has been impossible for me to not know about every important study related to myeloma and related disorders as they get published! For 20 years, I have received a precise summary of every important article published in my field. More importantly I am forced to read them, review the source material, and make a judgment call. As a result I remember this stuff. A gift indeed!


![rajshekharucms's tweet photo. MajesTEC-9 is now out in @NEJM! 18-month PFS ~70% and DoR~80% with Tec! Infection risk mostly front-loaded (1st 6 months) but doesn't plateau [G3+ infections remains at ~10% in each time window beyond 12 months]. The slope of PFS curve in Tec arms progressively flattens with time➡️will there be a plateau with long-term follow-up?
#ASCO26](https://pbs.twimg.com/media/HJf6ZiUXYAAcEYV.png)
![rajshekharucms's tweet photo. MajesTEC-9 is now out in @NEJM! 18-month PFS ~70% and DoR~80% with Tec! Infection risk mostly front-loaded (1st 6 months) but doesn't plateau [G3+ infections remains at ~10% in each time window beyond 12 months]. The slope of PFS curve in Tec arms progressively flattens with time➡️will there be a plateau with long-term follow-up?
#ASCO26](https://pbs.twimg.com/media/HJf53ZUWoAIT5fK.png)




















![rajshekharucms's tweet photo. MajesTEC-9 is now out in @NEJM! 18-month PFS ~70% and DoR~80% with Tec! Infection risk mostly front-loaded (1st 6 months) but doesn't plateau [G3+ infections remains at ~10% in each time window beyond 12 months]. The slope of PFS curve in Tec arms progressively flattens with time➡️will there be a plateau with long-term follow-up?
#ASCO26](https://pbs.twimg.com/media/HJf6Zi0WQAEYo92.png)