🧠🫁 In neurocritical care, extubation is not simply a respiratory decision.
It is a brain protection strategy.
The article proposes an important shift:
Weaning in neurocritical patients should not only evaluate:
✅ oxygenation
✅ ventilation
✅ secretion management
but also:
🧠 neurological stability
🧠 intracranial pressure dynamics
🧠 cerebral perfusion
🧠 delirium prevention
🧠 neuroinflammatory risk
One of the strongest messages of this review is that: Mechanical ventilation is not biologically neutral for the brain.
The review summarizes emerging evidence showing that ventilator induced lung injury (VILI) may trigger systemic cytokine cascades involving:
⚠️ IL 1
⚠️ IL 6
⚠️ TNF α
⚠️ NF κB activation
with potential downstream neuroinflammation and secondary brain injury.
Particularly interesting is the discussion around: 🧠 IL 6 mediated neuroinflammation 🧠 microglial activation 🧠 post extubation delirium 🧠 long term cognitive impairment after prolonged ventilation
The review also highlights an uncomfortable clinical reality:
📌 Failed extubation in neurocritical patients is not a benign event.
It is associated with:
• increased mortality
• longer ICU stay
• higher pneumonia rates
• prolonged mechanical ventilation
• higher tracheostomy rates
One of the most valuable contributions is the proposed CAPREVI algorithm.
Rather than asking: “Can this patient breathe?”
the algorithm asks: 🧠 “Is the brain stable enough to tolerate extubation?”
That distinction is fundamental.
The proposed framework integrates:
• neurological stability
• ICP considerations
• airway secretion control
• hemodynamic status
• delirium prevention
• sedation optimization
• respiratory muscle strength
• spontaneous breathing trials
• multimodal neuromonitoring
Another highly important point:
⚠️ traditional ICU weaning protocols may inadequately account for cerebral vulnerability.
This is particularly relevant in:
• severe TBI
• SAH
• ICH
• neuro postoperative patients
• prolonged neuro ICU admissions
The review also appropriately emphasizes resource limited settings.
Advanced multimodal neuromonitoring is ideal, but neuroprotection can still be approached systematically using:
📌 bedside clinical examination
📌 airway evaluation
📌 ultrasound
📌 CT imaging
📌 structured neurological assessment
Perhaps the most important conceptual takeaway is this:
🧠 Extubation failure in neurocritical care may itself constitute a form of secondary brain injury.
And that changes how we should think about ventilator liberation in this population.
Modern neurocritical care increasingly requires us to stop separating:
🫁 lung physiology
from
🧠 brain physiology
because critically ill patients experience both simultaneously.
📖 Zarra F,. Brain Circulation. 2026. DOI: 10.4103/bc.bc_10_26
This review considers pathophysiology & natural history of malignant MCA stroke, indications for DHC, technical considerations of craniectomy & cranioplasty, & importance of clear communication in shared decision-making.🧠
https://t.co/KPEZ2bdRUm
#SCCMNeuro#NeuroICU#NeuroX
🧠⚡ EEG may be one of the most underused monitoring tools in modern intensive care.
This new 2026 perspective in Critical Care argues something provocative:
EEG should evolve from a specialist diagnostic test into a true bedside monitoring system for intensivists.
The paper highlights a reality we face daily in ICU:
Many critically ill patients develop: • delirium
• non convulsive seizures
• metabolic encephalopathy
• hypoxic ischemic injury
• sedation related cortical suppression
Yet much of this cerebral dysfunction remains clinically invisible.
Especially in: ⚠️ sedated
⚠️ mechanically ventilated
⚠️ unconscious patients
Clinical examination alone is often insufficient.
One of the strongest points of the article:
The authors argue EEG should follow the same trajectory as: 📌 bedside echocardiography
📌 lung ultrasound
Not every intensivist needs to become a neurophysiologist.
But intensivists should learn to recognize: • background suppression
• asymmetry
• burst suppression
• epileptiform activity
In the same way we identify: • RV failure
• tamponade
• B lines
• pneumothorax
This is a major conceptual shift.
The proposed model is particularly interesting.
The authors describe a tiered EEG system: 🟢 simple bedside alarms for nurses
🟡 simplified interpretation for ICU physicians
🔵 qEEG trend analysis for trained intensivists
🔴 full raw EEG interpretation for neurophysiologists
Combined with: 🤖 AI assisted pattern recognition
The objective is not replacing experts.
The objective is: faster recognition of dangerous brain physiology.
One of the most important messages:
Current ICU monitoring focuses heavily on: • blood pressure
• oxygenation
• cardiac output
• ventilation
But often ignores the organ we are ultimately trying to protect: 🧠 the brain.
EEG may become the missing physiological layer of multimodal ICU monitoring.
The article also raises a very practical concern: alarm fatigue.
If EEG systems generate excessive false positives, ICU staff will rapidly ignore them.
This is where AI may become transformative: continuous surveillance without fatigue.
Particularly fascinating is the potential future of:
📡 point of care EEG
📡 emergency department EEG
📡 prehospital EEG
📡 tele neurophysiology
Imagine: an ambulance transmitting simplified cerebral activity before hospital arrival.
That possibility no longer sounds futuristic.
My personal takeaway:
Critical care spent decades refining cardiovascular monitoring.
The next frontier may be: continuous functional brain monitoring.
Not simply detecting seizures.
But integrating cerebral physiology into real time ICU decision making.
📖 Reference
Taccone, F. S., Critical Care, 30, 195. https://t.co/RqVX8PXbkv
Presenting at the Emirates Critical Care Conference 2026 🇦🇪 ,in the country where I spent 19 years of my life and childhood — feels incredibly special. From attending my first critical care conference here to presenting at one today…. Surreal. #ECCC2026#CriticalCare
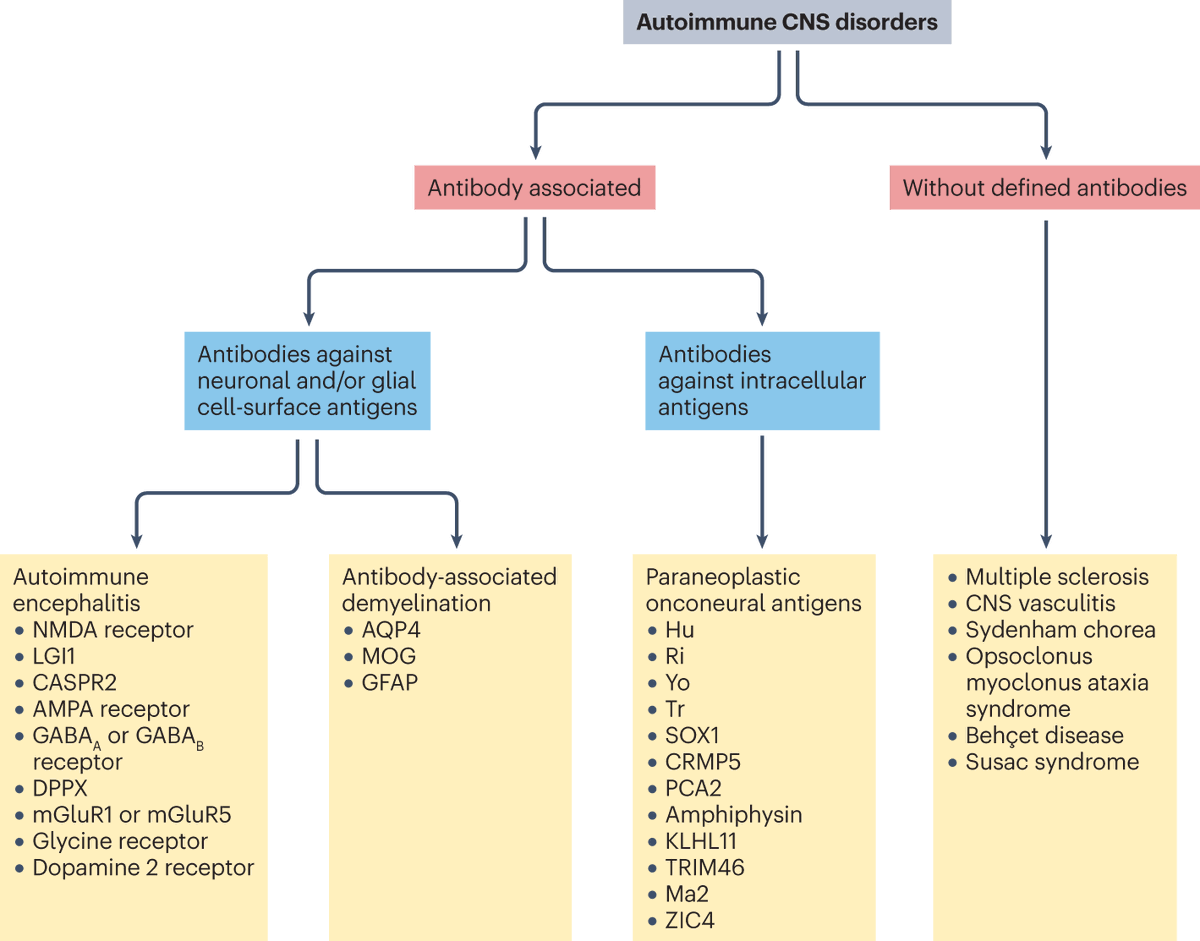
A structured overview of Autoimmune Central Nervous System (CNS) disorders, categorizing them based on the presence and type of associated antibodies.
https://t.co/w5382UVIOX
Incredible energy and enthusiasm on display at American Academy of Neurology this year by @UNMCCOM medical students and residents, their research, curiosity, and drive to push the boundaries of neuroscience are truly inspiring 👏@UNMC_neurology
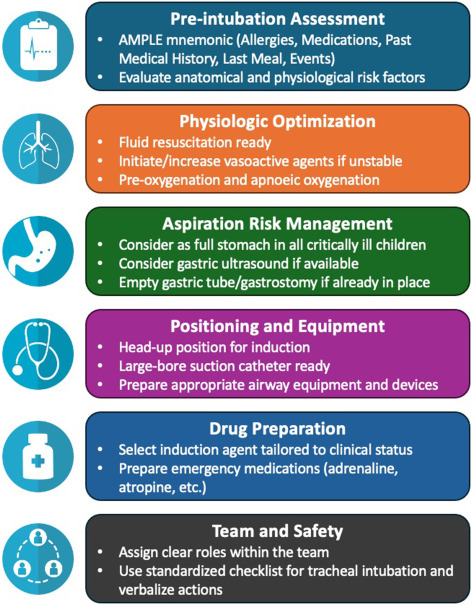
The invisible emergencies: metabolic and neuro-critical disorders often missed in the pediatric ED — a narrative review
CCR Journal Watch
https://t.co/Sp06oA6IDG
AKI guidelines hadn’t been updated since 2012.
The KDIGO 2026 AKI/AKD Public Review Draft just dropped and it changes how we define, diagnose, and follow up after acute kidney injury.
Here’s what every nephrologist, intensivist, and internist needs to know 🧵
⚠️ Public review draft only · Not yet final guidelines
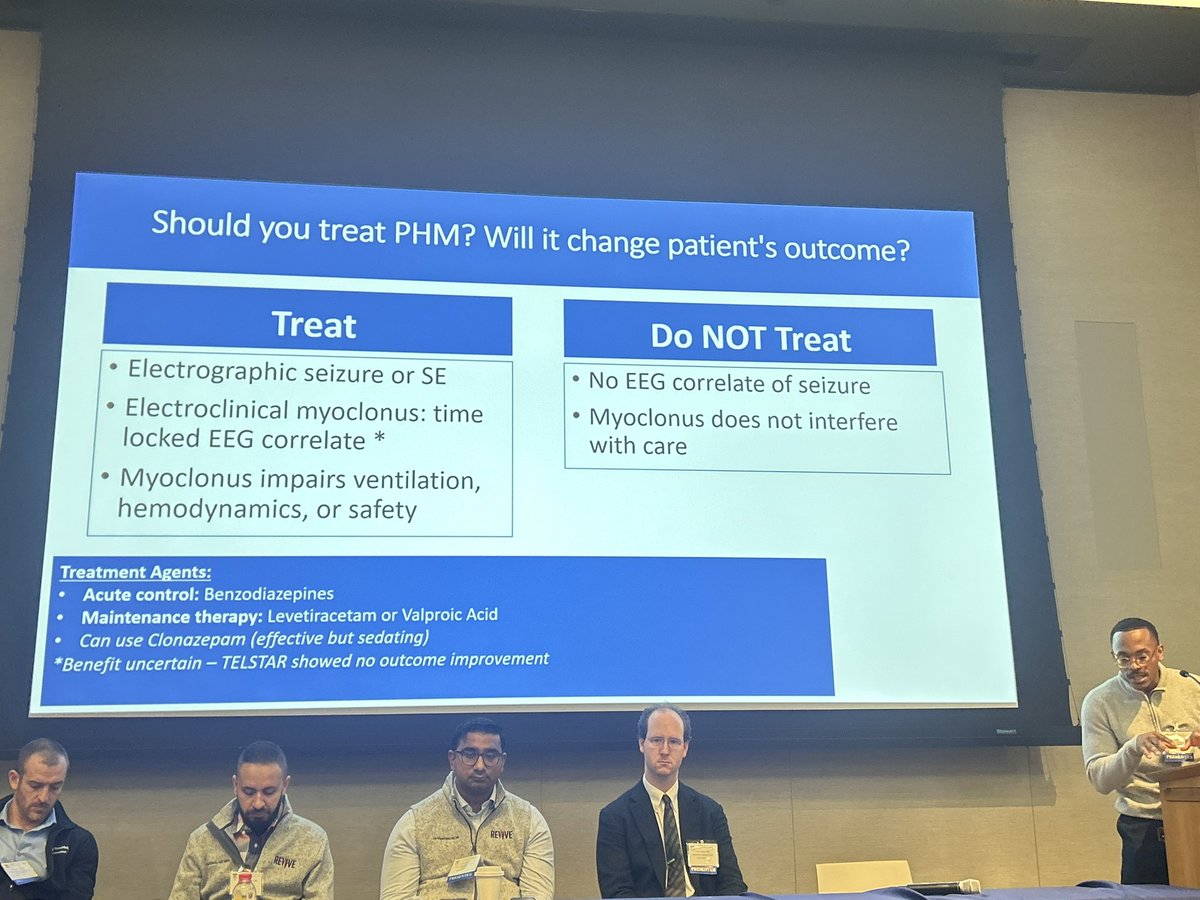
Post-Arrest Myoclonus by Dr. Joshua Madden
❇️Myoclonus should not be synonymous with poor outcome
❇️Myoclonus can be difficult to discern
❇️Obtain an EEG to help you
#REVIVE2026@OscarJMitchell@CardioNerds
Catherine Chu, MD, MA, MSc will present #Grandrounds Thursday, February 5th at 12:00 p.m. (CST)
Dr. Chu is the Director of Child Neurology and Pediatric Epilepsy, Vice President of Neurology at Kennedy Krieger Institute at Johns Hopkins University
Her topic: Sleep Rhythms, Epilepsy, and Memory Dysfunction
Shyam Prabhakaran, MD will present #Grandrounds Thursday, January 29th at 12:00 p.m. (CST)
Dr. Prabhakaran is Professor and Chair for the Department of neurology at University of Chicago
His topic: Symptomatic Intracranial Atherosclerotic Disease Management.
@aszelikovich, @gabifpucci, Jonathan, and I created this infographic on a simple step-by-step method for interpreting a nerve conduction study. I hope you find this helpful! 🤓 Thank you @GreenJournal for publishing it!
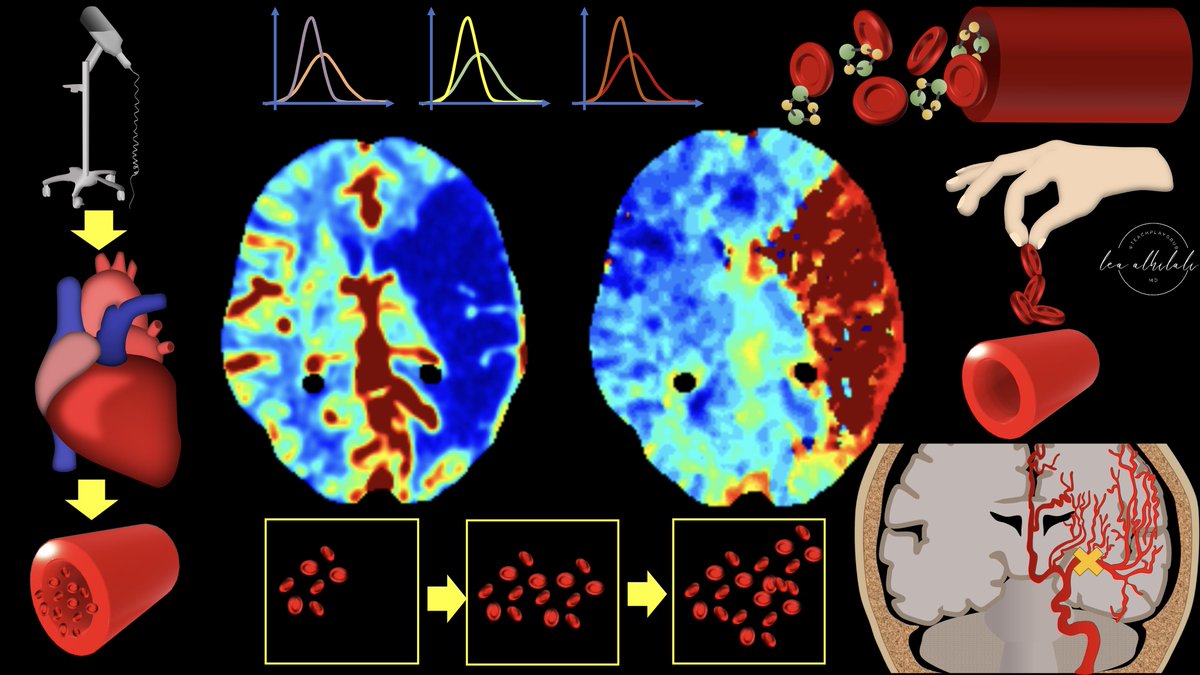
1/My hardest thread yet! Are you up for the challenge?
How stroke perfusion imaging works!
Ever wonder why it’s Tmax & not Tmin?
Do you not question & let RAPID read the perfusion for you? Not anymore!