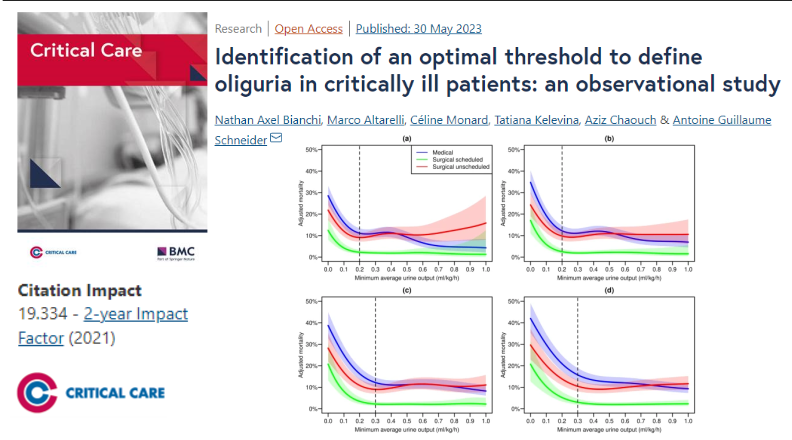
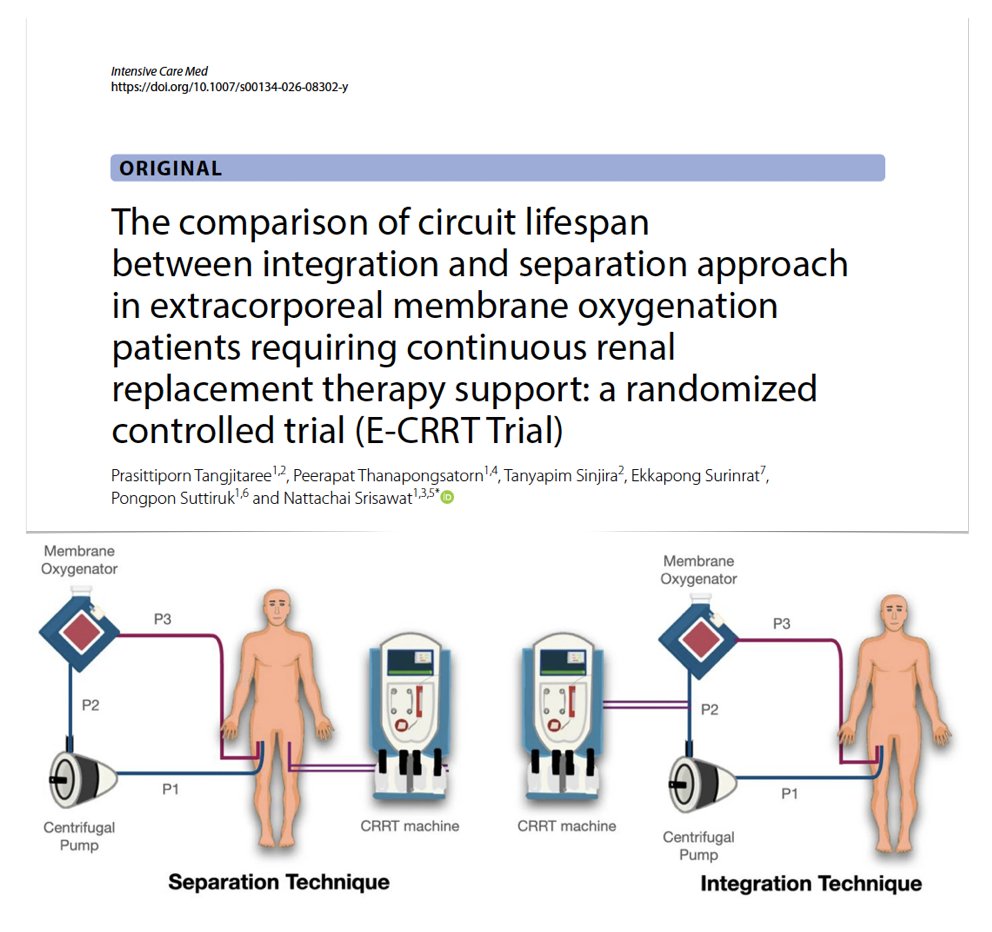
(Circuit) integration or separation approach in #ECMO patients requiring #CRRT? E-CRRT RCT
🔎 80 pts allocated to CRRT/ECMO circuits integration vs separation
⚖️ no significant difference in filter lifespan between integration/separation configurations
🪦 comparable mortality
🫧 no significant differences in serious adverse events, including air embolism
🚨 transmembrane pressure + CRRT machine alarm frequencies similar
#FOAMcc
🔓 https://t.co/SZ0y6Yx0Me
Among patients with early #SepticShock, a personalized hemodynamic resuscitation protocol targeting capillary refill time was superior to usual care for the primary composite outcome, primarily driven by a lower duration of vital support.
#LIVES2025@ESICM
https://t.co/UQH5mSw8Ty
@IM_Crit_ It actually is pseudohyperbocarbonatemia. Other possibility is hyperlipid/hypertriglyceridemia. Doubt monoclonal gammopathy -- no protein gap and hypocalcemic anyways.
I'd have to lit search to find alt. Reason. (Rhabdo or very high LDH can also cause this -- different mech.).
@cgaibor102@PoojaJagadishMD@drjohnm The avg. pt on HD has 19 pills/day. there is evidence of increased rates of adverse effects from statins. Don't force pills when (good) evidence says not to. Uremia in general lowers LDL. They have more calcific dz and hyperTG. They are different from pts with functioning kidneys
@cgaibor102@PoojaJagadishMD@drjohnm I agree with you about transplant but that's just opinion. There is observational data that patients who were on a statin prior to transplant have fewer CV events, and they will be prescribed a statin regardless after transplant.
@NephroSeeker@giovannilandoni@NephJC This is my point. If 2 groups, and 1 got a drug that lowers Cr, I'd expect at least some mathematical analysis of how the lower Cr after surgery compares to expectation from drug effect. Without that the trial seems of low value to me, and even with -- not a "randomized trial."
His serum sodium is 149 mmol/L. You prescribe iHD with a predicted Kt/V of 1.0 against a dialysate sodium of 138 mmol/L.
Ignoring Gibbs-Donnan, what would be the predicted loss of plasma volume l, if any. Would you proceed or adjust your prescription?
#nephrotwitter@PennKidney
Dialysis problem: 64M cirrhosis with high cardiac output state, HRS now on KRT awaiting SLK. Recently resuscitated for UGIB with hemorrhagic shock now 1+d without bleeding. VStable vitals on room air A+Ox3. Diarrhea from lactose. You decide not to remove fluid and to trial iHD.
@acweyand Nephrologist. We routinely get iron studies. Earlier this year I set up a patient for IV iron and, no joke, when our office visit was over and we were about to say goodbye she says, "Oh yeah I was meaning to ask you... Lately I can't stop eating baking soda right out of the box."
@WilliamAird4 As the proud husband of a veterinarian I am peppered every day with amazing things that non-human animals (and their spleens) can do that we cannot.
@captainchloride@thecurbsiders Is the HF observation a dosing issue? The starting dose is 12.5 mg for that indication (even in the pediatric literature it's 1 mg/kg starting dose. I don't have many 12.5 kg patients these days). And in general, at most HF wind up on half the doses seen in cirrhosis at most.