[Editor’s Choice: April 2026] Matteo Conti, Davide Mascioli, Clara Simonetta, Jacopo Bissacco, Valerio Ferrari, Silvio Bagetta, Federico Carparelli, Stefano Borrelli, Nicola Biagio Mercuri, Silvia Minosse, Mariangela Pierantozzi, Francesca Di Giuliano, Eliseo Picchi, Alessandro Stefani, Tommaso Schirinzi. Morpho-functional correlates of gait impairment in early Parkinson’s disease patients: insights from a multimodal path modeling framework. Clinical Neurophysiology 2026;184:2111700. https://t.co/ZWx3qe8MYF
Editor's Commentary: The development of effective treatment for gait impairment is a major unmet need in Parkinson’s disease because issues such as freezing of gait often do not respond to dopaminergic medications or even deep brain stimulation. In this volume of Clinical Neurophysiology, Conti et al. studied 73 Parkinson’s disease patients using brain MRI and EEG. MR Parkinson Index (MRPI), which assesses midbrain atrophy using ratios of pons to midbrain area and middle to superior cerebellar peduncle width, correlated with clinical gait scores. EEG α band functional coupling negatively correlated with both MRPI and gait scores. The study highlights the use of multimodal biomarkers to understand gait impairment, delineate clinical heterogeneity and potentially could be used to design personalized neuromodulation treatment for PD.
By Robert Chen
Editor-in-Chief, Clinical Neurophysiology
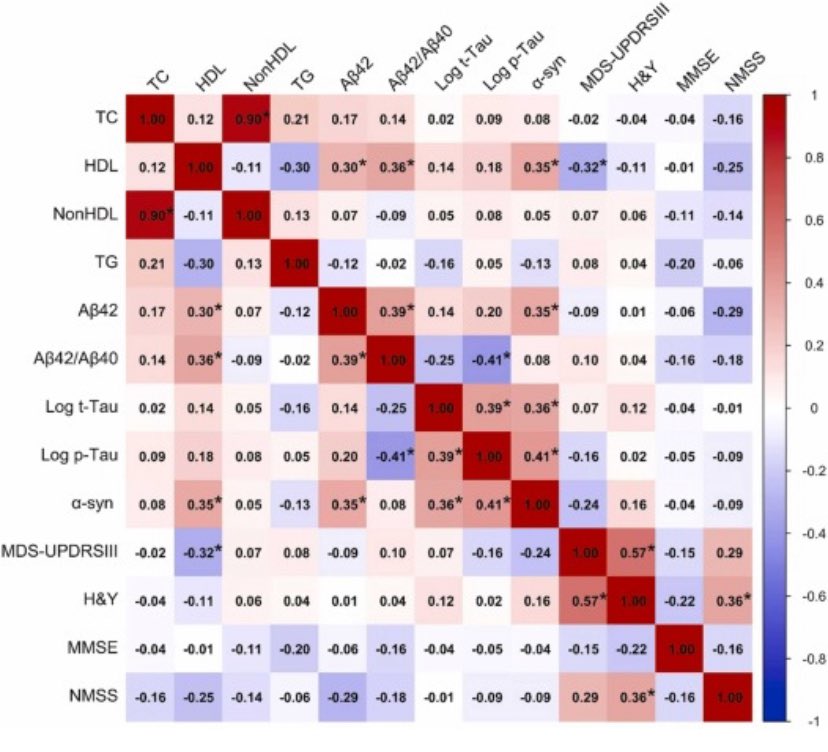
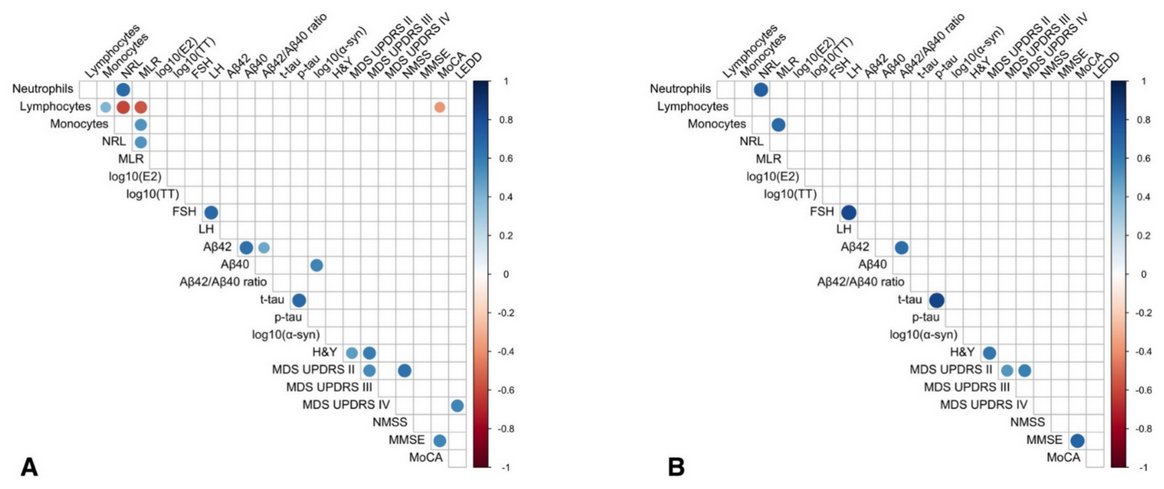
Just published in @GreenJournal our work demonstrating that #APOE4 carriers with de novo #Parkinson’s disease exhibit higher clinical severity associated with amyloid-mediated network disruption.
@unitorvergata@ptvonline2001
https://t.co/8Izqf3pyxR
La nostra ricerca su “#Ormoni sessuali e differenze di sesso nella malattia di #Parkinson ad esordio precoce” è nella Newsletter della Medicina di Genere dell’ @istsupsan Ist. Sup. di Sanità.
Grazie a @robe_bo che da tempo si occupa del tema. @unitorvergata@ptvonline2001
Should we be stimulating the old vagus nerve (e.g. VNS) to steady movement and quiet inflammation in Parkinson’s and beyond? How about a 2025 update? The vagus nerve is the major parasympathetic highway linking brainstem nuclei to body organs and it can be electrically stimulated to modulate circuits involved in movement, mood and immune system tone. Proietti and colleagues describe in a new paper just published in Movement Disorders how invasive and non-invasive vagus nerve stimulation may treat Parkinson’s and other movement disorders by tuning brain networks and possibly calming inflammation.
Key Points:
- The evidence for the vagus nerve approach spans many diseases including Parkinson’s tremor, cervical dystonia and Tourette.
- There are signals for possible motor and nonmotor improvement using vagus stimulation.
- Vagus nerve stimulation (VNS) engages multiple transmitters (brain chemicals) including GABA, norepinephrine and acetylcholine.
- VNS may possibly reduce neuroinflammation while enhancing plasticity.
- Transcutaneous auricular VNS has shown promise as a potentially safer and more scalable option.
My take: I am less confident that the author’s that VNS is ready for prime time as an add on strategy if you have persistent Parkinson’s symptoms (e.g. gait freezing, tremor, anxiety or GI issues). I do think VNS for movement disorders is promising and should be in used in the context of a research study. Here are 5 interesting points that resonated w/ me about this paper. 1- Non-invasive ear or neck stimulation is different from deep brain stimulation (DBS). 2- Non-invasive stimulation is largely designed to nudge circuits rather than to ablate or directly pace deep targets. 3- Early trials have shown improved step length, gait stability and sometimes tremor improvement w/ taVNS (ear based) or tcVNS (neck based), however the effects have varied across studies. 4- Safety has been reasonable w/ only mild skin or autonomic sensations in many reports, although long term outcomes will still require more rigorous tracking. 5- The field critically needs bigger as well as sham-controlled trials w/ clear dosing schedules. It sure would be helpful to have an electrical (bio)marker like STN beta power!
https://t.co/k0UhacriCB @FixelInstitute@ParkinsonDotOrg@MDCP_Journal@movedisorder
Here our work on #olfactory mucosa derived from #Parkinson patients. Oligomeric a-synuclein localizes in dysfunctional mitochondria. Nrf2-cytoprotective response is impared although with changes along the disease course due to the dopaminergic therapy. https://t.co/oDcbpiam4r
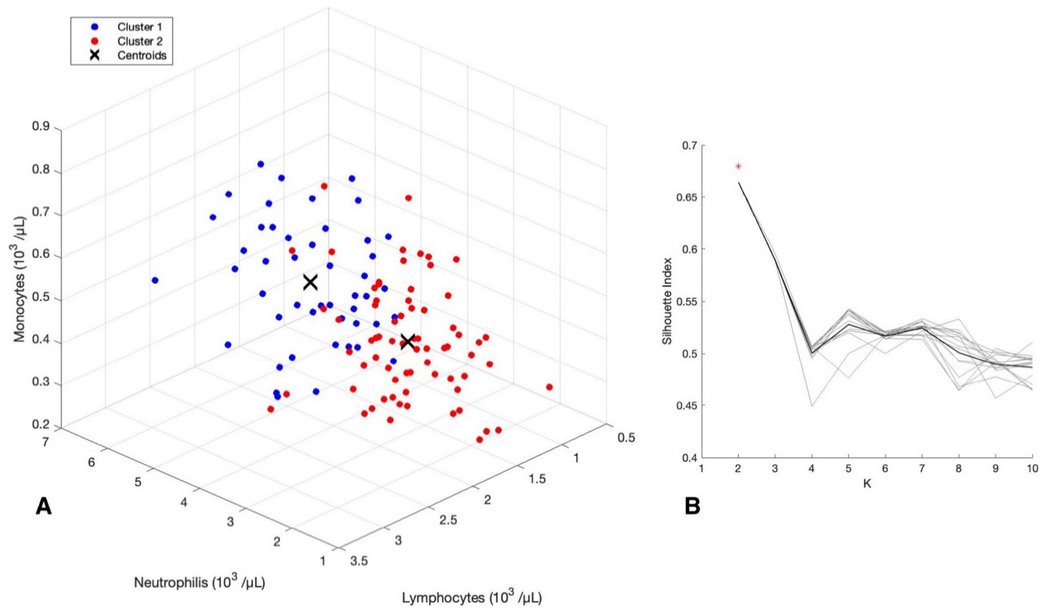
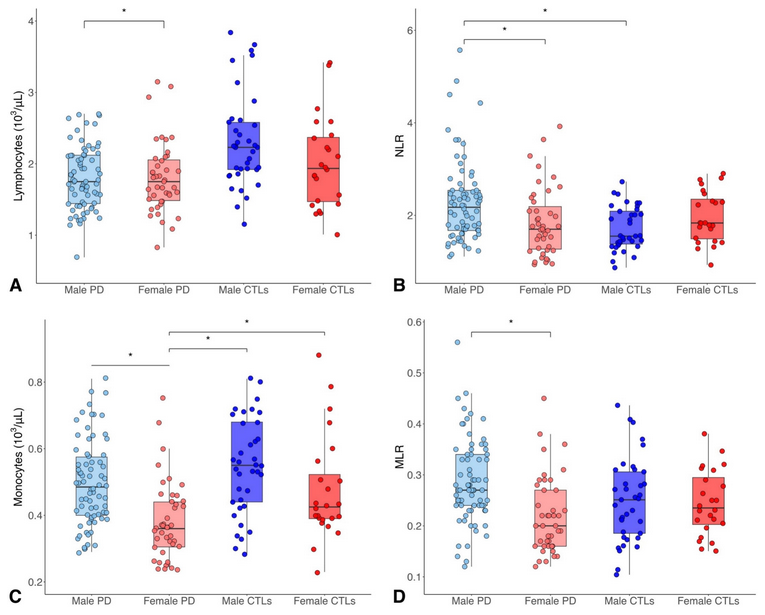
Immunity might have a role in #Parkinsons sexual dimorphism; New study compares blood samples from 117 PD patients & 86 controls; ♂️PD cases had⬇️lymphocyte counts &⬆️neutrophil-to-lymphocyte ratio than♂️controls. ♀️PD had⬇️monocyte counts than ♂️PD
https://t.co/m8JQbqfgdt
We tried to dissect the complex interplay among #sex, sexual #hormones, #immunity and the #biology of #Parkinson’s disease finding significant patterns of association
https://t.co/Th67Af1TMD
Neuroinflammation is strongly considered a major player in the pathogenesis of neurodegenerative disease. Dr. Tommaso Schirinzi shares how the results of his study evaluating peripheral leukocytes in PSP patients adds to this growing body of evidence. https://t.co/gDZ8GAHzCb
Just out by Bissacco et al:
GIDS-PD Constipation scores correlated with PD motor severity and CSF α-synuclein and t-tau protein load in 55 de novo PD patients. Very glad to see the GIDS-PD used as a useful tool in PD research!
https://t.co/qZjxGS1qCy
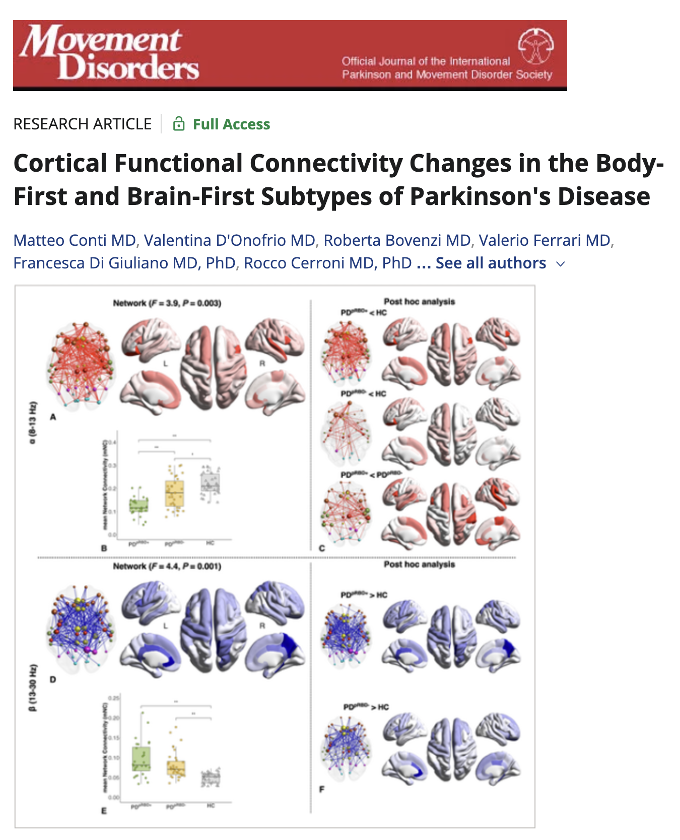
Check out these cortical functional connectivity changes in the body-first and brain-first subtypes of Parkinson's. Can you say cholinergic and 'the α band.' Pretty cool study by Conti and colleagues @MDJ_Journal.
Key Points:
- There were 28 PD RBD+, 35 PDpRBD− folks and 35 controls.
- 64-channel EEG system.
- Compared to PDpRBD- the brain-first subtype, the PDpRBD+ group the body-first subtype demonstrated specific EEG-FC dysfunctions in the α band.
- The authors argue early involvement of the cholinergic ascending system.
My take: The authors noticed that the most prominent difference between PDpRBD+ and PDpRBD− was in prefrontal, anterior cingulum, and temporal regions of the brain. Interestingly, the increased β network was related to bradykinesia severity in both subgroups. They opine changes could reflect the neurophysiological substrate of body-first and brain-first subtypes. Body-first patients had reduced connectivity in the α band in prefrontal, temporal, and limbic regions, and the authors hypothesize this may be 'mirroring the early cholinergic denervation.' I love the hypothesis, however this type of study will need some replication.
https://t.co/NOXXKKlVm1 #Parkinson



















![ClinicalNeuroph's tweet photo. [Editor’s Choice: April 2026] Matteo Conti, Davide Mascioli, Clara Simonetta, Jacopo Bissacco, Valerio Ferrari, Silvio Bagetta, Federico Carparelli, Stefano Borrelli, Nicola Biagio Mercuri, Silvia Minosse, Mariangela Pierantozzi, Francesca Di Giuliano, Eliseo Picchi, Alessandro Stefani, Tommaso Schirinzi. Morpho-functional correlates of gait impairment in early Parkinson’s disease patients: insights from a multimodal path modeling framework. Clinical Neurophysiology 2026;184:2111700. https://t.co/ZWx3qe8MYF
Editor's Commentary: The development of effective treatment for gait impairment is a major unmet need in Parkinson’s disease because issues such as freezing of gait often do not respond to dopaminergic medications or even deep brain stimulation. In this volume of Clinical Neurophysiology, Conti et al. studied 73 Parkinson’s disease patients using brain MRI and EEG. MR Parkinson Index (MRPI), which assesses midbrain atrophy using ratios of pons to midbrain area and middle to superior cerebellar peduncle width, correlated with clinical gait scores. EEG α band functional coupling negatively correlated with both MRPI and gait scores. The study highlights the use of multimodal biomarkers to understand gait impairment, delineate clinical heterogeneity and potentially could be used to design personalized neuromodulation treatment for PD.
By Robert Chen
Editor-in-Chief, Clinical Neurophysiology](https://pbs.twimg.com/media/HE0ZWlYXQAAYJcG.jpg)