I already know the answer to this, but I would like to know why Medicare Part D plans don’t cover generic Restasis.
Brand name Restasis costs $630 a month.
The generic costs roughly $30 a month.
We need to end PBM kick-back exemptions.
🚨 Please watch: While casually walking in NYC, a man goes unhinged by my presence. He yells and screams that I am “Islamophobic and racist” but can’t give one example.
Shouts “someone is going to find you” while signaling a gunshot to the head.
“I want you to go into any leftist organization and show them my photo and they will know who I am” he yells when I ask him how he has helped society.
Uncovering fraud and helping America has become the most dangerous job in America, unfortunately.
It's one thing for the PBM lobby to announce a 7-figure ad campaign to repair their reputation as harmful middlemen who drive up the cost of prescription drugs. But now they claim to be "the most transparent part of the drug supply chain.” 🤯
Why in the hell is epinephrine (EpiPen) not covered across all insurance plans for an affordable price?
Around here, anyone and their brother can pick up as many Narcan’s as they need for $0.
Just ran a claim for a patient who needs an EpiPen and their insurance makes them pay $395 for the cheapest generic option.
Pharmacy wholesale cost is north of $170 a box.
So, even running it as a cash-pay is unaffordable for majority of patients.
THIS is the legacy of PBMs, America's WORST corporate citizens.
CVS/Caremark, ExpressScripts, Optum - this is on YOU.
All those politicians that enable this, YOU TOO are complicit.
BAN PBMs. Then investigate, indict and incarcerate.
Eliminating fraud, waste and abuse should be the most nonpartisan issue in America as it affects everyone.
Those who are against it are simply anti-American and are the fraudsters.
For instance, Tim Walz and Ilhan Omar are SILENT about the fraud because they are the fraudsters
Meanwhile, our government @AFergusonFTC@MeadorFTC@AlMeyer19 allows $CVS fortune 7, $UNH fortune 3, and $CI fortune 13 to steal and use the theft to pay fines. Never put on @OIGatHHS exclusion list nor dropped from @CMSGov networks. Malfeasance
https://t.co/CutTOHFtjx
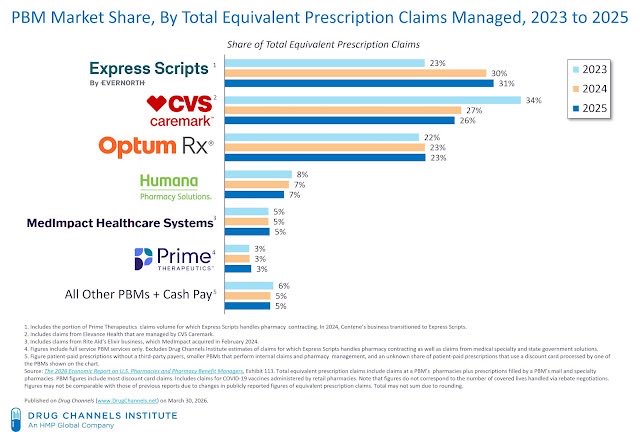
3 PBMs have 80% of pharmacy business
Same 3 run mail order and specialty
Same 3 owned by healthcare conglomerate
Result:
They control competitor access to insurance networks
Offer competitors take or leave contracts
They pay competitors below cost, below what they pay themselves
They charge back, clawback fees and audit competitors
They use competitor dispense data to market their mail order
They bill payers 10X, 100X, 1000X what they pay competitors
Tennessee just did what Congress can't.
They passed a law to break up the health insurance giants.
Specifically, they made it illegal for pharmacy benefit managers — the companies in charge of pharmacy insurance — and pharmacies to be owned by the same company.
That makes perfect sense.
For example: CVS Caremark is the PBM, and CVS is the pharmacy. So if you have Aetna insurance, you have CVS Caremark as your PBM, and they're going to do everything they can to make sure you use CVS as your pharmacy. Aetna, Caremark, CVS — all the same company.
That causes all kinds of incredibly obvious problems that this law hopes to fix.
If your insurance company is in charge of approving your medication, deciding how much to pay for it, AND deciding who gets that money — while also being the pharmacy that gets paid at the end — guess what happens to prices?
They go up.
Governor Lee signed the law last week. CVS immediately filed a federal lawsuit because they said it will force them to close all 136 stores they have in Tennessee.
Let that sink in.
I'm not sure most people realize what that says about CVS and health insurance in general. They had to choose between owning the middleman (the PBM) or the healthcare provider (the pharmacy).
Without hesitation, they chose the middleman.
The biggest pharmacy chain in the country — with a store on every corner — would drop all 136 of their Tennessee locations in a second if it means keeping their middleman business.
It is more profitable for them to be a health insurance middleman getting between you and your healthcare than it is to actually provide the healthcare.
That is the problem with healthcare in America.
We have made the middleman so powerful that they've taken complete control of the entire system. Three PBMs — Caremark, Express Scripts, and OptumRx — handle around 80% of all prescriptions in this country.
How on earth can we expect healthcare to work well and remain affordable if that's where the money is?
We all auto-pay our insurance straight out of our paycheck before we even see the money. And not surprisingly, they're keeping a ton of it.
That's why we fired them.
And they can't file a lawsuit to stop us.
That lets us offer fair, transparent prices. No PBMs. No insurance games. No hidden markups. You see the cost, you pay the cost.
The worst decision in my life as a born and raised Nashvillian? Shutting down Opryland to open a shopping mall they could have built anywhere. Opryland would be even more popular today than it was when I was a kid. Huge whiff by the city. Loved it. Miss it.
🎉 The Patients Before Monopolies Act was reintroduced today in both chambers of Congress — and NCPA is proud to endorse it! This bill aims squarely at the conflicts of interest created by vertically integrated PBMs by prohibiting a parent company from owning both a PBM/health insurer and a pharmacy; requiring divestiture of pharmacy assets within one year; establishing strong enforcement; enabling private right of action; and preventing re-consolidation that would recreate the same anticompetitive structure.
“PBMs have a choice — operate as a PBM or operate as a pharmacy, but you can’t have it both ways. Having both functions under one roof is a huge conflict of interest and drives up prescription drug prices," said NCPA CEO Douglas Hoey. Read the rest of his statement: https://t.co/4wEhK5oxgf
The US healthcare system is fundamentally broken, and it’s being fueled by a $10,000 price tag on a $6 medication. 💊📉
Glenda and I opened Forest Park Pharmacy three years ago to build something better. We had no idea we were walking into a financial minefield where the "math" simply doesn't add up for small businesses or patients.
Here is the truth about how Pharmacy Benefit Managers (PBMs) are draining your wallet:
The Insurance Trap
After four months of operation, we realized we were making 2% less than the cost of the medications we dispensed. Our only income was insurance reimbursements, and they weren’t even covering the wholesale cost of the drugs.
The Great Copay Lie
We discovered that our patient’s copays were often higher than the actual price we would charge for the medication without insurance. You’re paying for a "benefit" that actually costs you more.
The "AWP" Scam
Ever heard of Average Wholesale Price (AWP)? It sounds like a standard metric, but it’s a phantom number. For example:
Teriflunomide: Our cost is $6. Our cost-plus price is $17.
Medicare pays: $3,700 per prescription.
Published AWP: $10,000.
Medicare is overpaying by $9 BILLION on just 50 common drugs because of these inflated metrics.
The Middleman Problem
PBMs (Pharmacy Benefit Managers) are hired to "control costs," but they take a percentage of the prescription cost. This means they are incentivized to keep prices high. The FTC estimates they take 41% of every dollar spent on generic drugs—and they don’t prescribe, manufacture, or dispense a single pill.
We’ve Had Enough.
We canceled every insurance contract and switched to a Cost-Plus Model:
✅ Drug Cost + 15% Markup + $10 Service Fee.
When we told our customers they’d save money by not using their insurance, we immediately lost 70% of our business. People are so conditioned to trust their "benefits" that they’d rather pay a higher copay than a lower cash price.
It’s time to pull back the curtain on the PBM disaster. High drug costs aren't an accident—they're the system working exactly as designed.