In 1982, scientists named KRAS the first human oncogene. For the next four decades, some of the sharpest minds in cancer biology called it "undruggable."
Today, that word officially expired.
At the ASCO plenary this weekend, the phase 3 RASolute 302 trial showed a once-daily oral pill nearly doubling overall survival in second-line metastatic pancreatic cancer — published simultaneously in the New England Journal of Medicine.
For context on why this is hard: pancreatic cancer is the most RAS-addicted cancer we have, with KRAS mutations in more than 90% of patients. Five-year survival sits around 3%. Second-line chemotherapy has offered modest benefit for years.
The science took four decades and several relay handoffs to get here:
1982 — KRAS identified as the first human oncogene
2013 — Shokat's lab at UCSF finds the hidden switch-II pocket, reopening the field
2021–22 — sotorasib and adagrasib become the first KRAS inhibitors, but only for G12C, which is rare in pancreatic cancer
2026 — daraxonrasib, a multiselective RAS(ON) inhibitor, finally hits the G12 variants that actually drive PDAC — and wild-type RAS too
RASolute 302 randomized roughly 500 previously treated patients to oral daraxonrasib or investigator's-choice chemotherapy. In the intent-to-treat population: median OS 13.2 vs 6.7 months (HR 0.40, p<0.0001), median PFS 7.2 vs 3.6 months, and a response rate of 31.6% vs 11.2% — with benefit across RAS mutation status.
I want to hold two things at once here.
This is a genuine inflection point AND it comes with a real management burden. Daraxonrasib showed no new safety signals, but the rash, stomatitis, and diarrhea are not trivial — they need proactive, dermatology-informed supportive care. That's straightforward at an academic center. It's harder in the community settings where most patients with pancreatic cancer are actually treated. If "undruggable to doubled survival" is going to mean something for every patient, the supportive-care playbook has to travel with the drug.
That's the part of these stories I keep coming back to: the breakthrough and the delivery system have to arrive together.
For the scientists who refused to give up on a target everyone else abandoned — and the patients and families who enrolled when there was no guarantee — this is their result.
As we move RAS(ON) inhibitors toward first-line and into lung and colorectal disease, we have to make sure the supportive-care infrastructure reaches broader oncology community at the same pace as the drug discovery.
#Oncology #PancreaticCancer #KRAS #PrecisionMedicine #ASCO2026 #DrugDevelopment #ClinicalTrials #CommunityOncology #HealthEquity
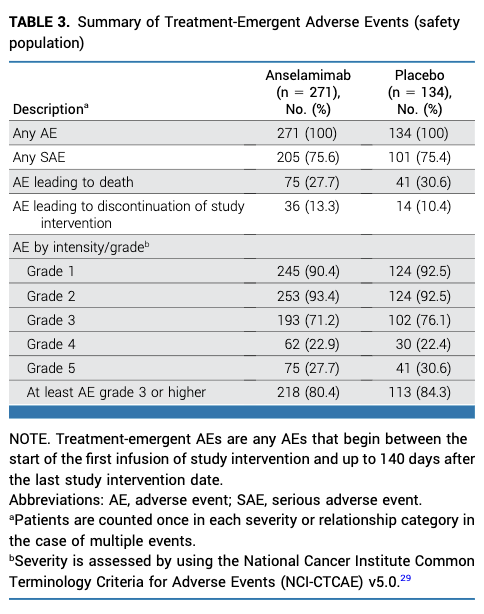
#Myeloma Paper of the Day: Randomized CARES trial of anti-fibril antibody anselamimab in AL #amyloidosis did not meet primary end point in overall population but improved all-cause mortality cardiovascular hospitalizations in patients with kappa AL: https://t.co/939temEkIR. #alsm
The CD123-directed antibody-drug conjugate pivekimab sunirine-pvzy is now approved for adults with blastic plasmacytoid dendritic cell neoplasm (BPDCN).
A meaningful advance in a rare leukemia subtype, with important contributions from Dr. Naveen Pemmaraju and Dr. Naval Daver. https://t.co/j08bRpyZN8 @doctorpemm@Daver_Leukemia #EndCancer
Redefining Early Relapse in Multiple Myeloma — Time to Change the Rules. A thoughtful editorial on MajesTEC-9 by @mvmateos@NEJM#mmsm#bmtsm https://t.co/VkO2GeWdya
MajesTEC-9 trial: Teclistamab vs. VPd or Kd in RRMM, 1-3 prior lines. N=593, median F/U: 17.3 months. 18-month PFS 70% vs. 27%, HR: 0.29. 41% grade 3-4 infections, 6.5% deaths in Teclistamab arm #mmsm#ASCO26@NEJM https://t.co/I4kSOdeoL3
Nonmyeloablative conditioning (Flu-TBI) + anti-CD117 antibody briquilimab in older adults with high-risk AML and MDS. N=32, median age: 70, 1-year OS 75% in both AML and MDS #bmtsm@LoriMuffly https://t.co/zh8TrWa1Xp
With #ASCO26 approaching, here are the potentially practice-changing abstracts in plasma cell disorders that caught my attention. I will update my thoughts as simultaneous publications are released for some of them🧵#MultipleMyeloma#Amyloidosis
Peripheral blood MRD assessment by MALDI-TOF mass spectrometry in NDMM in the Phase III GMMG-HD7 Trial. It complements BM MRD and may emerge as a minimally invasive monitoring tool #mmsm#bmtsm@EliasKarlMai https://t.co/dbZJHmLUUb
How does major clinical practice change happen in medicine? What are the requirements? Do influential voices on social media have influence?
Smoldering multiple myeloma (SMM) offers a great perspective on this with the rapid adoption of daratumumab in the community after the AQUILA trial results.
These 5 points on how practice change happens will apply to any new treatment or disease.
1) Practice change happens when the evidence is strong. This means convincing trial results.
2) Practice change happens when the treatment actually works. The drug must work and work as promised in the trial. This is important. If physicians in practice get outcomes contrary to what a trial reports, they will abandon it.
3) Practice change happens when the treatment is feasible. FDA and EU regulatory approval is essential for major practice changing treatments.
4) Practice change happens when the treatment is aligned to what physicians and patients actually wanted to do all along. This is important. In smoldering myeloma most were uncomfortable with watch and wait. So when there is effective therapy, practice changes.
5) Practice change is probably influenced by influential voices on social media, but only if it rings true, aligns with above 4 points, and is delivered by experts. I don’t think having a lot of followers alone helps; credible subject matter expertise is important.
Background for those not familiar with smoldering myeloma
For decades observation without treatment was the standard of care. After AQUILA trial results for smoldering myeloma came out, many including me (biased of course as the lead investigator) felt that the trial results were compelling. We therefore recommended daratumumab for high risk SMM.
But we were sandwiched on both sides by contrary opinions. One side were some who felt we needed to be even more aggressive and use full myeloma therapy, and on the other side by some who felt we should not use any drug for treatment and just watch and wait. All voices were active on social media.
18 months later, we know from market research is that uptake of daratumumab for high risk SMM is very high. Practice changed. Basically we can criticize and comment all we want but to have real impact it must reflect reality, reflect concerns of patients, reflect clinical practice concerns of physicians, and social media comments and criticisms must be credible.
As I write this, personally I have experienced this many times: adoption of low dose dex and adoption of weekly SQ bortezomib, adoption of DRd, adoption of quads in MM etc. They all fulfilled the 5 points.
@SagarLonialMD@szusmani@Mohty_EBMT@Myeloma_Doc@RahulBanerjeeMD@Transplant_Doc@mtmdphd@DavidSteensma
A suite of new studies links popular weight-loss and diabetes drugs to lower cancer risks and better outcomes for those with the disease, though researchers say more research is needed https://t.co/JrL06oijap via @WSJ
A comprehensive review of prognostic factors and progression biomarkers in AL, categorizing them into: a) disease-specific (clone-related and organ-related) and b) patient-specific factors @rajshekharucms#amyloid https://t.co/j3vRcjA99T
Administration of IV iron therapy during acute infections was associated with improved 14- and 90-day survival #hematology@BloodPortfolio@CAMCHemOncIAM https://t.co/X7ad8vDvyl
With 85% CD38-refractory, we are seeing at least a similar (if not better) PFS with single-agent Teclistamab when compared to Cilta-cel arm of CARTITUDE-4, which had just ~25% CD38-refractory. These results, along with MajesTEC-3, challenge the dogma of “CAR T before BsAbs” in all for early relapse. Looking forward to the manuscript! #ASCO26