Continuous EEG Monitoring in Canadian Hospitals: A Nationwide Cross-Sectional Survey
🔑 5 Key Points
1.🏥 Severely Limited Availability – Only 2% of Canadian hospitals and 68% of tertiary care centers offer continuous EEG (cEEG), showing widespread underutilization.
2.🌍 Geographic Inequities – Geographic disparities were significant, with 3 provinces and all 3 territories lacking cEEG access.
3.⏰ Restricted ICU Access – Even in hospitals with cEEG, monitoring is often limited to select ICUs, with no 24/7 technologist coverage and limited after-hours setups.
4.💻 Technological Gaps – Only 26% of hospitals with cEEG use quantitative EEG (qEEG), and few have access to abbreviated montages or point-of-care devices, tools that could improve efficiency and coverage.
5.🇨🇦 National Health Implications – Findings reveal major infrastructure gaps in neurocritical care, emphasizing the urgent need for national strategies to ensure equitable access to cEEG across Canada.
⸻
📖 Reference:
Niznick N, Tang H, Kromm J, et al. Continuous EEG monitoring in Canadian hospitals: a nationwide cross-sectional survey. Neurol Clin Pract. 2025;15(5):e200522.
🔗 Read the full article here https://t.co/FOktH3yvvu
Comment: is there a role for AI-EEG limited montage in offhours to screen until daytime conventional cEEG is possible?
Quote from article: “In addition, commercially available point-of-care EEG devices such as Ceribell (CA), Zeto (CA), and Emotiv (CA) could provide a cost-effective approach to implementing screening EEG monitoring outside typical clinical hours. The only point-of-care device currently available in Canada is VEEGix (Montreal, Canada), which is a more limited device with only 3 prefrontal electrodes. However, none of these devices is currently available in Canada. The deployment of point-of-care EEG devices could enable rapid cEEG initiation in resource-limited settings and improve access in remote areas.”
Editorial on this too:
Keezer MR, Lapalme-Remis S. Inequities in critical care continuous EEG coverage in Canada. Neurol Clin Pract. 2025;15(5):e200530. doi:10.1212/CPJ.0000000000200530. Full text
Thank you Dr. David Okonkwo for a great talk on the role biomarkers play in traumatic brain injury management!! Congratulations to you and your team for the innovations in TBI management!
@PittNeurosurg@umichmedicine@umichneuro@Aditya_S_Pandey
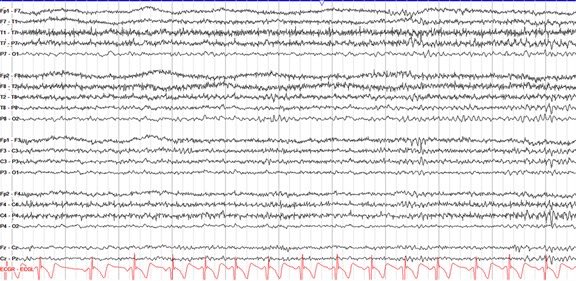
A 24 year old comes in for episodic loss of awareness
1-2 episodes/month, triggered by school stress
All unwitnessed
Diagnosed with epilepsy, modest response to levetiracetam + lamotrigine
Ambulatory EEG (below) + MRI completely normal
Is it time to reconsider the diagnosis?
@FlyTPA Our Southwest flight 1889 to Tampa from ATL was just delayed 12 hours due to "volume" issues at Tampa airport. Should we consider flying into another location or will the issues be resolved today?
Minimally Invasive Surgery for Spontaneous ICH: Meta‐Analysis of High‐Quality Randomized Clinical Trials
Over 3000 pts in 14 high quality trials
MIS wins!
Nice work @chriskellnerMD and all!
https://t.co/vZCe9ccSSW
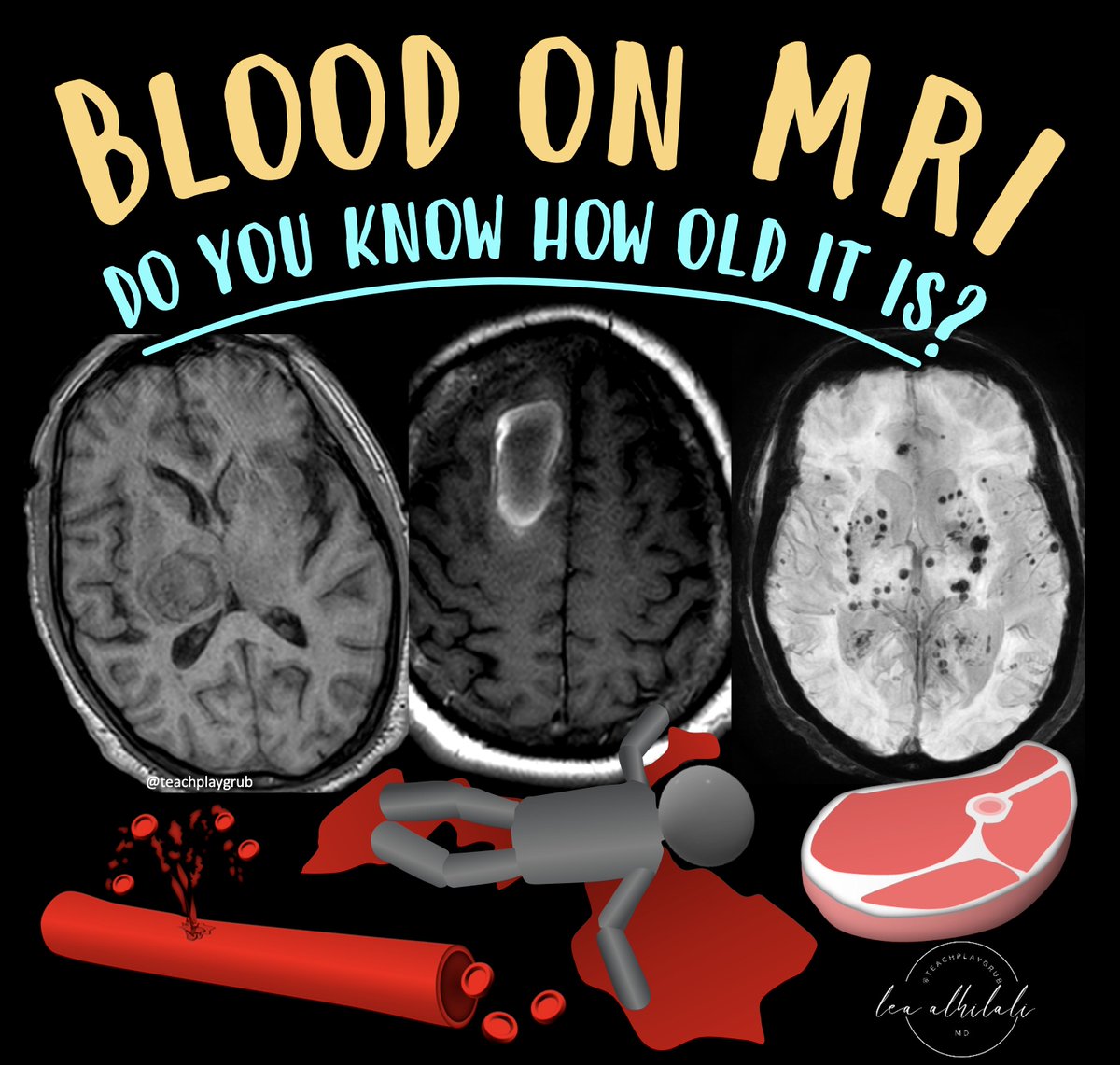
1/Asking “How old are you?” can be dicey—both in real life & on MRI! Do you know how to tell the age of blood on MRI?
Here’s a thread on how to date blood on MRI so that the next time you see a hemorrhage, your guess on when it happened will always be in the right vein!
The CNS is deeply saddened to hear of the passing of neurosurgeon Dr. Justin Singer. Dr. Singer was an accomplished and respected cerebrovascular and endovascular neurosurgeon. He was a passionate CNS volunteer for our educational programs and scientific program committee. His enthusiasm for neurosurgical education and commitment to service were remarkable. The legacy of his contributions to the CNS and our field will live on in our community. We extend our condolences to his family, friends, and the Corewell Health community during this difficult time.
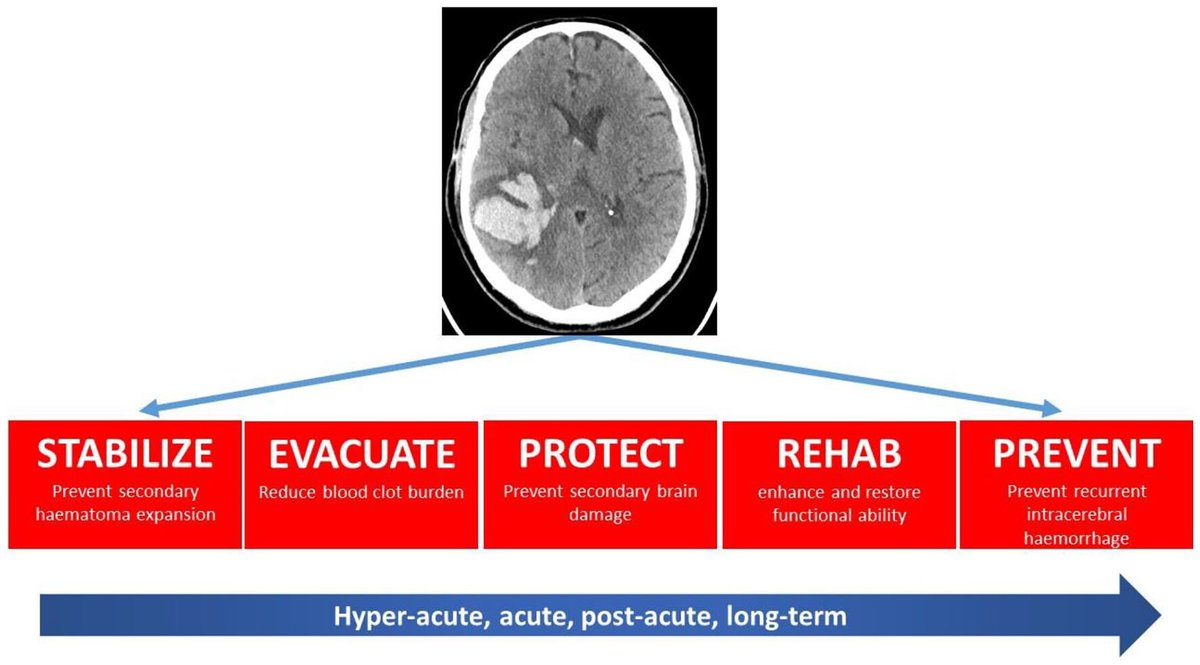
5 key points from the paper “Code-ICH: A New Paradigm for Emergency Intervention” by Aleksandra Yakhkind, W Yu, Q Li, JN Goldstein and @stephanamayer
1.🧠⏰ Urgency in ICH Treatment: Intracerebral hemorrhage (ICH) treatment needs the same urgency as ischemic strokes. Early intervention, especially in the first few hours, is critical for better outcomes.
2.💉🔍 Blood Pressure Control: Intensive blood pressure reduction, when implemented quickly and smoothly, helps minimize hematoma expansion and improve patient outcomes.
3.🛡️🔄 Anticoagulation Reversal: Rapid reversal of anticoagulation in patients with ICH is essential to reduce hematoma growth and improve survival rates.
4.🏥📊 Bundled Care Approach: A multifaceted, bundled care approach, combining blood pressure control, anticoagulation reversal, and other treatments, has shown promise in improving functional outcomes in ICH patients.
5.🌐📋 Standardized Protocols: Adoption of standardized, time-based protocols like Code-ICH can help reduce disparities in care, improve tracking of patient outcomes, and facilitate better emergency intervention for ICH.
@NIH #FASTEST #LaurenNg
https://t.co/mdrBu0vsMK
Great paper by @DanOrringerMD, @MILOLab2 and team in @natBME integrating two translational brain tumor imaging technologies: SRH and 5-ALA. This paper shows how to move the needle on glioma care through imaging research! Impressive work.
https://t.co/6HxRDnLsV9
NICO is excited to attend SNIS from the 22 – 25 of July. Please stop by and see us at booth #305 and join us at the Golden Bee Restaurant to hear about unlocking the future of ICH evacuation.
Another important trial for surgery in ICH patients. Again it is not if surgery is beneficial but which patients should receive intervention based on patient and disease characteristics.
New blog post! How to handle thrombolytic reversal
What do you do when a patient experienced symptomatic hemorrhagic conversion after alteplase/tenecteplase? There is surprisingly little data guiding how to treat a potentially devastating complication.
https://t.co/AqiWanKMW3